

Volume 13, Issue 1 (Winter 2025)
PCP 2025, 13(1): 47-56 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Demehri F, Heydarloo R. The Effectiveness of Cognitive Rehabilitation on Behavioral Problems and Emotional Regulation Hearing Impairment’s Children. PCP 2025; 13 (1) :47-56
URL: http://jpcp.uswr.ac.ir/article-1-951-en.html
URL: http://jpcp.uswr.ac.ir/article-1-951-en.html



1- Department of Psychology, Faculty of Psychology, Science and Arts University, Yazd, Iran. , farangis_demehri@yahoo.com
2- Department of Psychology, Faculty of Psychology, Science and Arts University, Yazd, Iran.
2- Department of Psychology, Faculty of Psychology, Science and Arts University, Yazd, Iran.
Keywords: Cognitive rehabilitation (CR), Behavioral problems, Emotional self-regulation (ESR), Hearing impairment
Full-Text [PDF 599 kb]
(1020 Downloads)
| Abstract (HTML) (3633 Views)
Full-Text: (707 Views)
Introduction
Adequate sensory stimuli and typical sensory reception are necessary for the complete development of neural activity (Kral et al., 2016). Hearing impairment is one of the most frequent sensory deficits (Lieu et al., 2020). Sensorineural hearing loss is the most common type of hearing impairment, impacting 1 to 2 out of every 1000 newborns and 1 in 1000 adolescents. Children experiencing hearing impairment encounter challenges in fostering communication skills, comprehending others’ feelings and thoughts, and self-regulation. Consequently, they struggle to form strong bonds with peers, leading to limited social interactions and low emotional management (Morgan et al., 2021). The medical treatment of childhood hearing loss includes hearing aids, cochlear or brainstem implants, enhancement of signal-to-noise ratio in educational environments, speech therapy, and the utilization of sign language (Brennan & Bally, 2007).
Hearing impairment places a child in a challenging position between the hearing and deaf communities, leading to more significant behavioral issues in children with hearing impairment than their hearing peers (Korver et al., 2017).
A relationship exists between internalizing behaviors and hearing impairment in children that may continue even after cochlear implantation. Behavioral issues, such as conduct disorders, hyperactivity, and difficulties with emotional and executive functions in people with hearing impairment may stem from inadequate language development (Bigler et al., 2019). While individuals with hearing impairment are at a higher risk of developing behavioral issues, including elevated aggression, psychopathic traits, oppositional defiant disorder, and other behavioral disorders, some may also experience depression.(Yigider et al., 2020). Individuals with hearing impairment often have a heightened risk of depression, which can potentially lead to suicidal ideation (Adigun, 2017).
Emotional self-regulation (ESR) pertains to comprehending, adapting, and conveying emotions (Domaradzka & Fajkowska, 2018). Individuals with hearing impairment articulate their social and emotional encounters related to hearing loss using terms, such as adverse outcomes, feeling overwhelmed socially, fatigue, bereavement, exclusion, identity influence, emotional distress, frustration, sorrow, anxiety, isolation, and feelings of being burdensome (Bennett et al., 2022). Pensacola et al. reported that participants with hearing loss scored higher on alexithymia and lower for positive relationships. However, no significant differences were observed in emotional regulation between deaf adults and those with typical hearing (Peñacoba et al., 2020). Adults experiencing hearing impairment encounter challenges in recognizing emotions, resulting in lower scores in facial emotion discrimination, cognitive empathy, and tasks involving naming expressions, particularly the expression of fear (Martins et al., 2019). Since a significant and direct correlation is observed between emotional regulation and adaptive environmental behaviors, people with hearing loss show less adaptive behaviors when dealing with the environment because they have problems regulating emotions (Hintermair et al., 2013). On the other hand, one of the crucial components of cognition is emotion regulation (Mahrogi et al., 2021), therefore, if we can improve emotion regulation in hearing-impaired children by improving cognitive components, their behavioral problems may also decrease. Cognitive rehabilitation (CR) therapy significantly reduces cognitive failures and improves emotion regulation (Franco-Martín et al., 2020).
CR aims to identify and tackle individual requirements and objectives, which may involve employing new knowledge or compensatory techniques, such as utilizing memory aids (Bahar‐Fuchs et al., 2013). The meta-analysis results indicate that computer-based CR can be an effective method for cognitive recovery (Nie et al., 2022). Darvishi reported that motored-based CR can improve neuropsychological and orientation in nonverbal learning children (Darvishi et al., 2020). The research results showed that computer-based cognitive training enhances working memory (Oba et al., 2013), executive function, verbal memory, and attention in individuals with cochlear implants (Bansal, 2014). A systematic review study reported that the effect of cognitive training in improving cognition for adults with hearing loss is very low (Lawrence et al., 2018).
Since hearing impairment is linked to higher levels of mental distress, it can impact daily functioning and overall health (Dalton et al., 2003), interventions are required to reduce some behavioral issues in children with hearing impairment to improve psychological functioning. Due to the lack of agreement on the effectiveness of CR on the mental health of children with hearing impairment and the lack of research about the effectiveness of CR on behavioral problems of children with hearing impairment in Iran, this study was conducted to determine the effectiveness of CR programs on behavioral problems and ESR in children with hearing impairment.
Materials and Methods
Study design
The present research was a quasi-experimental study with a pre-test-post-test design and a control group. The study samples included 24 girls with hearing impairments aged 7 to 11 years living in Yazd City, Iran. They were randomly chosen using a convenience sampling method from children with hearing impairment referring to Naghmeh Clinic. A clinic audiologist assessed the level of hearing impairment of these children. Then the children were randomly split into two groups of 12 (intervention and control). The inclusion criteria included an age range from 7 to 11 years, a diagnosis of mild (hearing loss of 20 to 40 decibels) and moderate hearing impairment (hearing loss of 41 to 60 decibels) as assessed by an audiologist, no mental disability based on the children’s Wechsler test (score above 70) and no epilepsy or seizure. The exclusion criteria included cochlear implants, incomplete questionnaires, and non-participation in training sessions. Before beginning the research, the objective and process were presented to all participants. The mothers of the children in the sample group were present to cooperate in completing the children’s questionnaires in the research.
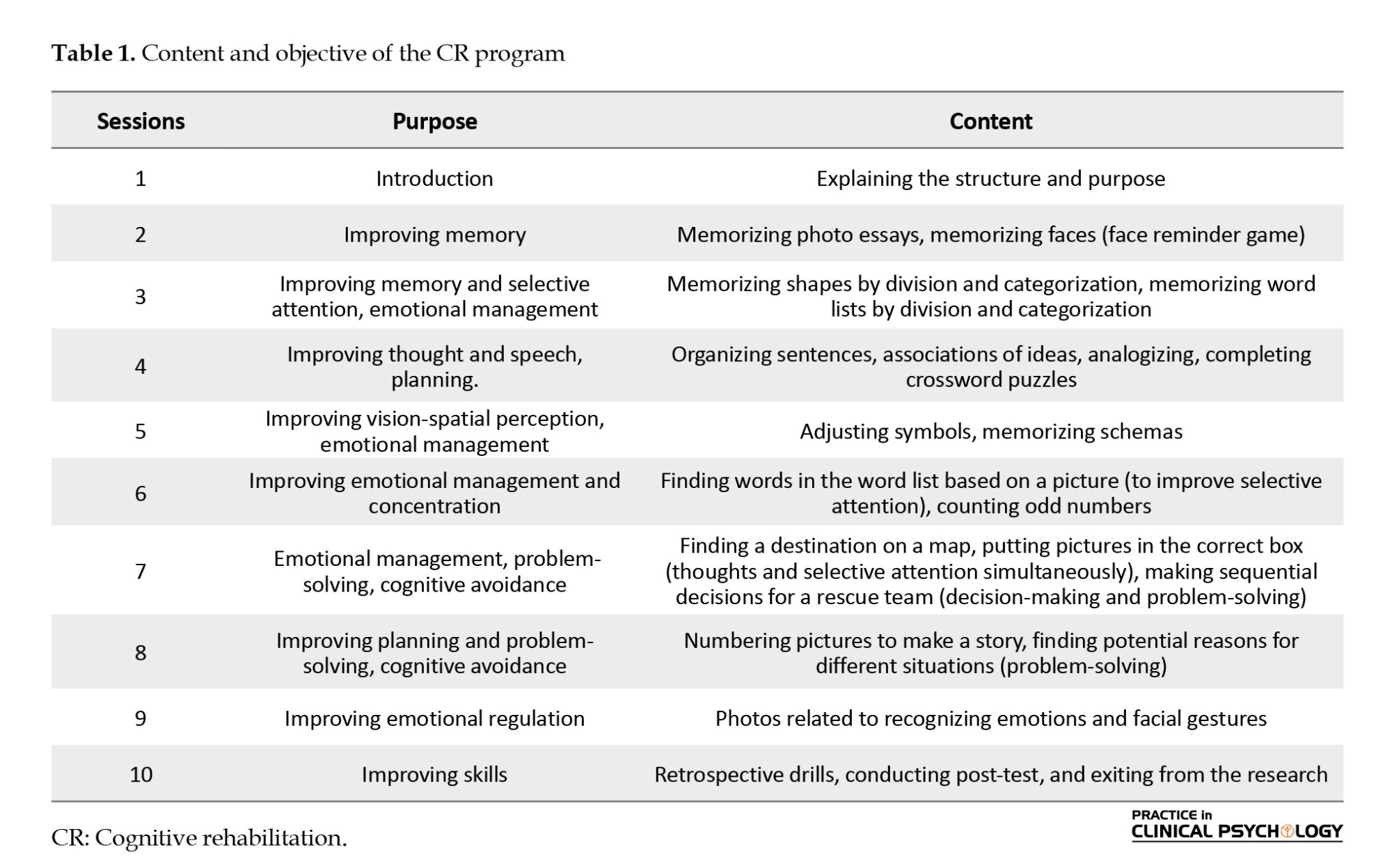
The intervention group underwent 10 sessions of a CR program based on Samuel (2008) and Nazarboland et al. (2019)., CR protocol. In this research, two protocols developed in Iran and abroad have been used to make them more suitable for Iranian children with hearing loss. Experts have checked the validity of this protocol. The CR package is an educational protocol based on Captain’s log cognitive trainer. This protocol helps improve memory, attention, perception, reasoning, planning, and emotional management. Although this protocol can be used with computers, in our research, this protocol was used for children based on computers and play with toys concerning ethical issues. After the end of the study, CR treatment was also performed for the control group.
Table 1 presents the educational content of the sessions. Each meeting lasted 90 minutes (two sessions every week). Since the children had hearing impairment, most of the exercises were based on images and games and emojis to regulate emotions. The control group did not receive the treatment.
Study instruments
Conners’ parent rating scale (CPRS)
The CPRS is a widely recognized tool in research and clinical practice for collecting parents’ observations on behavioral issues in children. The parent form has 48 items that parents fill out. Parents use the Likert scale to fill each item, and the answering spectrum starts with 0 (not true at all, never, or barely) to 3 (entirely true, mostly, almost always). Subscales of Conner’s test include cognitive problems, oppositional, hyperactive-impulsivity, anxiety-shy, perfectionism, social problems, and psychosomatic (Conners et al., 1998). The test reliability was reported between 0.41 to 0.57 for all scales (Gianarris et al., 2001). Factor analysis of this questionnaire in Iran showed four factors, including conduct problems, social problems, anxiety-shy, and psychosomatic problems. External problems are conduct and social problems. Internal problems include anxiety-shy and psychosomatic. In Iran, the validity and reliability of questionnaire for the re-test method was 0.58. Also the Cronbach α method, the coefficient of internal consistency of this questionnaire was 0/73 (Shahaeian et al., 2007). The Cronbach α was 0.75 in this research. Parents completed the questionnaire for their children.
ESR questionnaire (ESRQ)
The ESRQ includes 20 items, each rated on a 5-point Likert scale, where five represents “completely true about me” and one signifies “never true about me.” The possible scores range from 20 to 100. After translation and back-translation, psychology experts, to ensure both validity and content validity, reviewed the questionnaire, which was confirmed. This questionnaire assesses three key components or sub-scales, secrecy, compromise, and tolerance, with 5, 7, and 8 items assigned to each. Cronbach’s α reliability for the sub-scales of secrecy, compromise, and tolerance were calculated at 0.70, 0.68, and 0.50, with an overall reliability of 0.81. Additionally, indicator validity was satisfactory (Hofmann & Kashdan, 2010). In Iran, reliability and validity scores were reported as 0.70, 0.75, and 0.50 for the sub-scales, with an overall reliability of 0.81 (Karashki, 2013). In the present study, Cronbach’s α values for secrecy, compromise, and tolerance were 0.72, 0.7, and 0.69, respectively, and 0.76. For this research, parents filled out the questionnaire on behalf of their children.
Interventional sessions
The experimental group’s participants performed two sessions every week and underwent 10 CR therapy sessions. Each meeting lasted 90 minutes. Since the children had hearing impairment, most of the exercises were based on images and games and emojis to regulate emotions. The control group did not receive the treatment. Table 1 presents the educational content of the sessions.
Results
Twenty-four girls aged between 7 and 11 (mean age=9.17±3.32 years) with hearing impairment participated in the study. Their mean hearing score was 54.65 dB. All participants utilized hearing aids; none underwent cochlear implantation. Table 2 presents the demographic characteristics of the subjects. The study found no significant difference in the speech levels of the children. Only three children over three years old experienced hearing disability and used hearing aids.
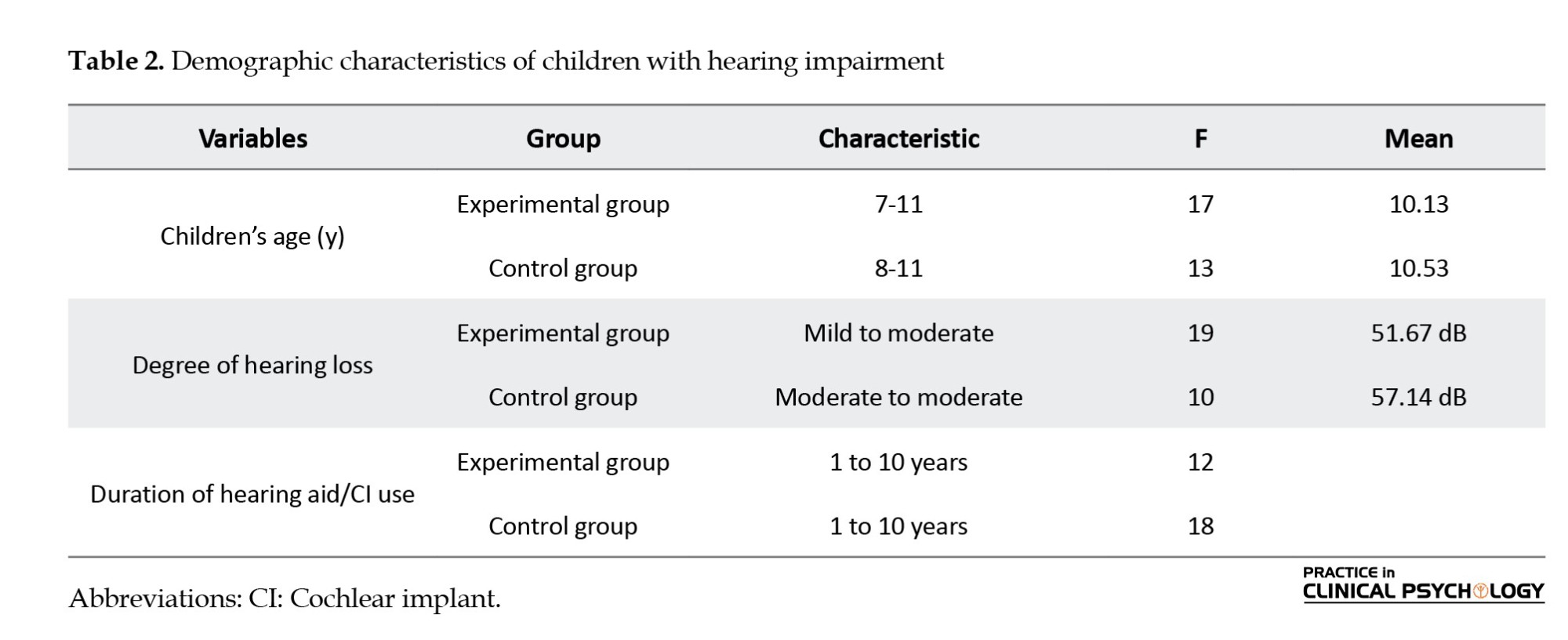
Table 3 presents the Mean±SD of the behavioral problems and ESR.
As shown in Table 3, the mean scores of behavioral problems in the intervention group decreased after the treatment and the scores of ESR increased after treatment. We use ANCOVA to search more about these observed differences. Before testing the hypothesis, the Kolmogorov-Smirnov test was utilized to examine the normality of scores for both variables, and the non-significance variables showed that their distribution was normal (P>0.05). According to Levine’s test and the non-significance of all variables, the assumption of the equality of inter-group variances for behavioral problems was also met (P≤005, F=8.2), and self-emotional regulation (P≤0.05, F=10.3). Also, the condition of variance-covariance material was established based on Box’s M test, which was insignificant for all variables (Box’s M=4.17, F=1.12). To evaluate whether there are statistically significant differences between the experimental and control groups, we employ a multivariate analysis of covariance (MANCOVA).
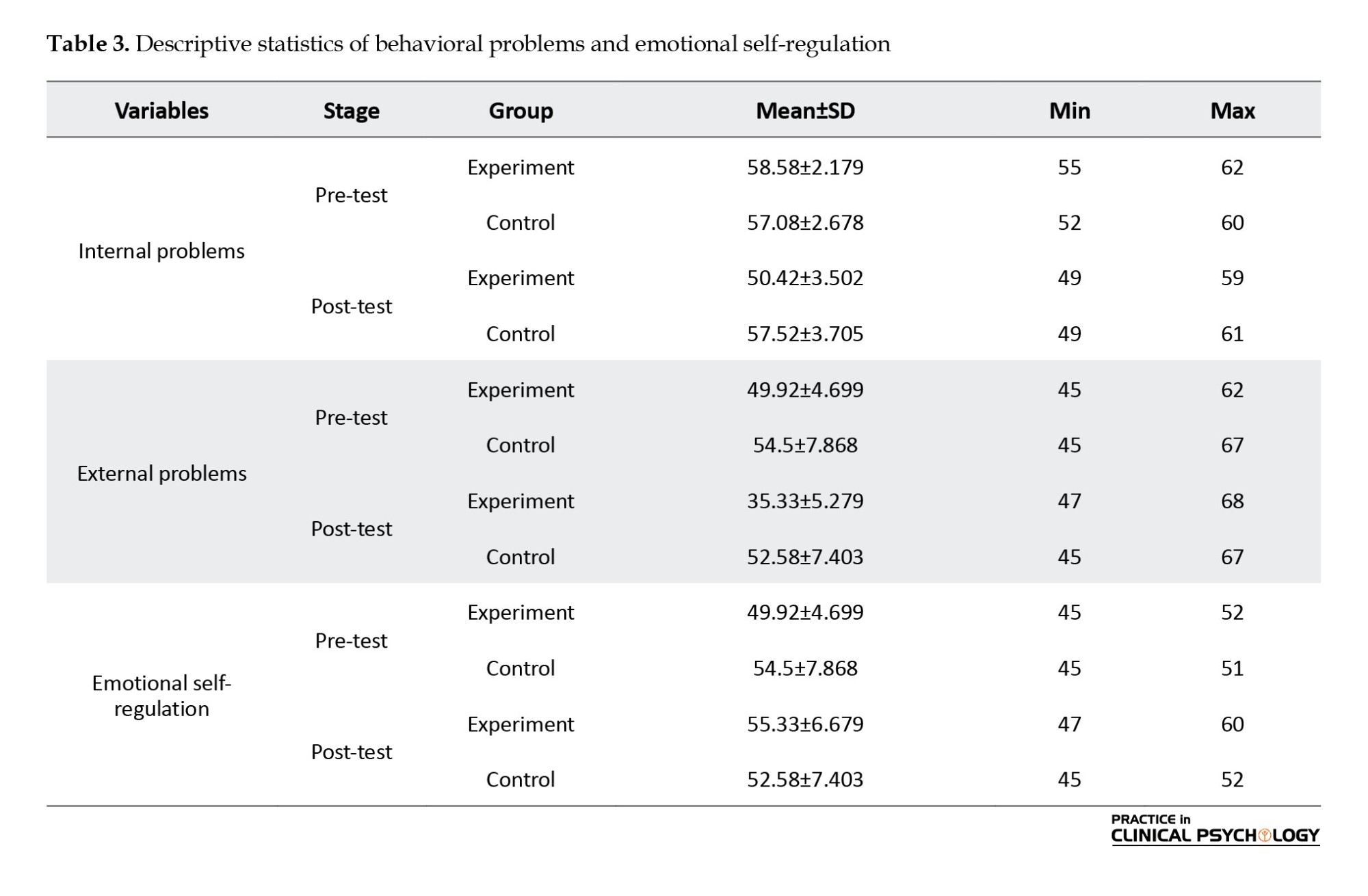
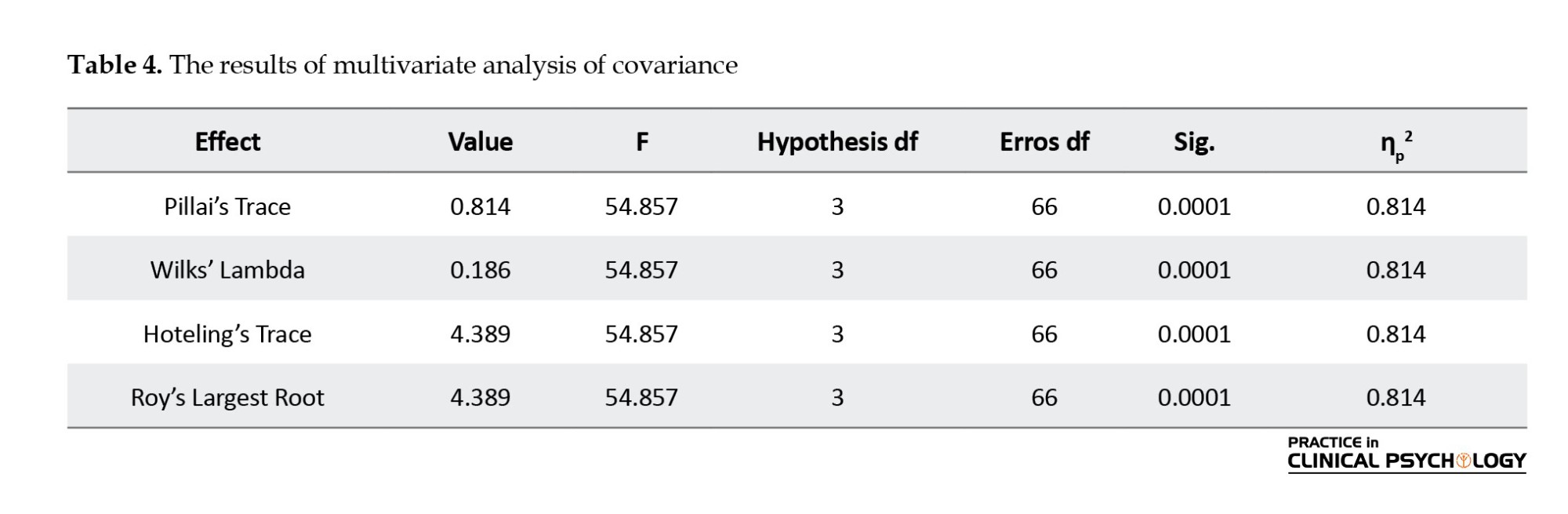
Table 4 presents the results of a MANCOVA conducted to assess the impact of a CR program on three dependent variables. All four tests statistics indicate statistically significant differences between the experimental and control groups (P<0.0001). The large values of Pillai’s Trace, Wilks’ Lambda, Hotelling’s trace, and Roy’s largest root confirm the robustness of the results. The partial eta squared value of 0.814 suggests that the CR program can explain a substantial proportion of the variability in the dependent variables. The results of multivariate analysis of covariance (ANCOVA) were designed to assess the impact of CR programs on three dependent variables, internal problems, external problems, and ESR.
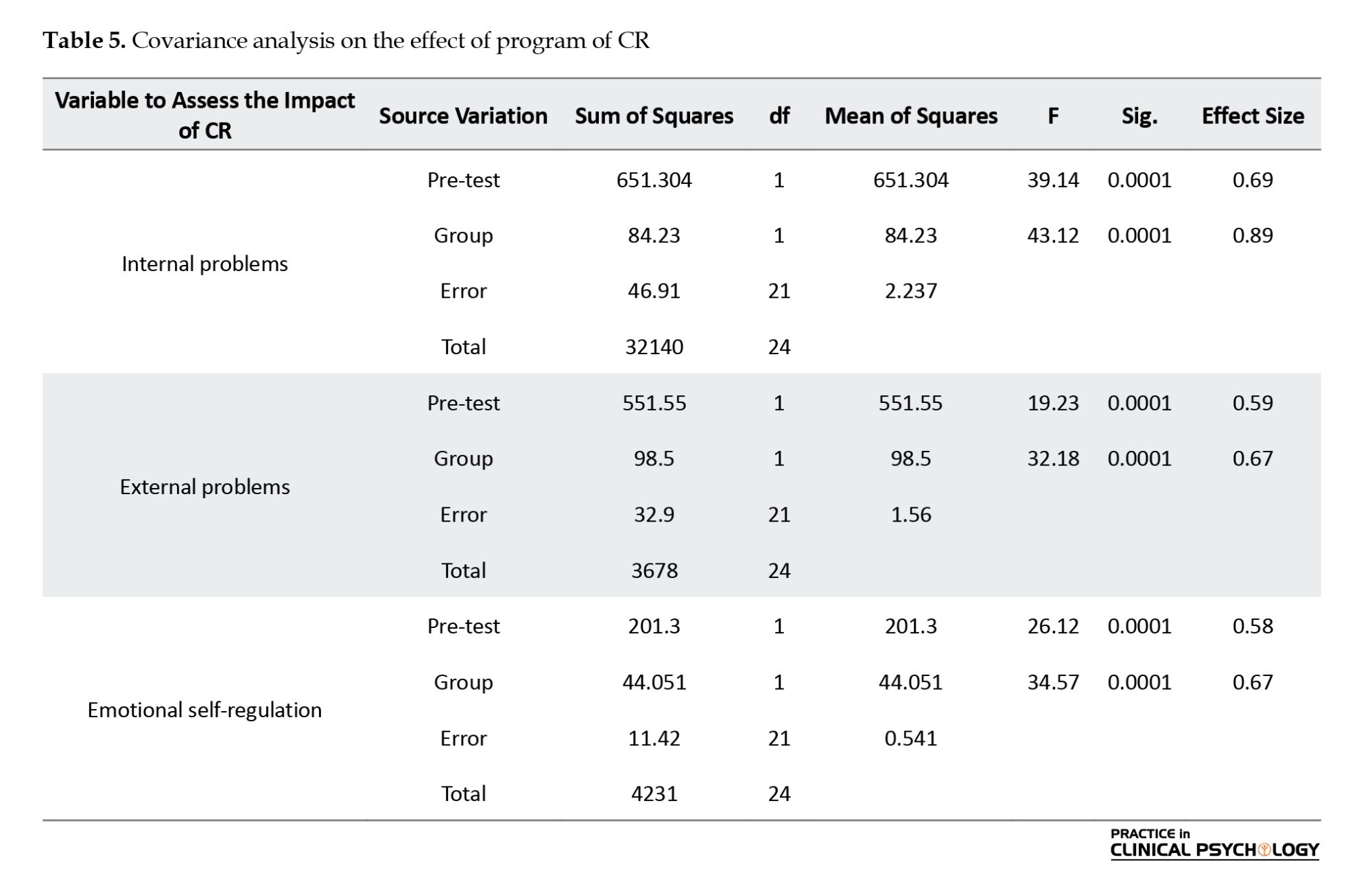
The results of Table 5 showed CR significantly enhances internal problems (P≤0.05, F=43.12, Eta=0.89), external problems (P≤0.05, F=32.18, Eta=0.67), and ESR (P≤0.05, F=44.05, Eta=0.67), as evidenced by the high F and effect sizes across all measured variables.
Discussion
The current research was conducted to investigate the effect of CR programs on the behavioral and emotional self-regulating problems of children with hearing impairment. Hearing impairment is common worldwide, and diagnosing and intervening before six months of age ensures normal language development, regardless of the severity of the hearing loss (Yoshinaga-Itano et al., 2020). This study supports the concept that managing behavioral problems in children with hearing impairment is improved after performing CR therapy. The current study’s results are not consistent with the results of Lawrence et al., (2018), that reported CR has a low effect on improving cognition in adults with hearing impairment. Still, these results are consistent with the results of Bansal, (2014), which reflected cognitive training has a modest positive effect on executive function and working memory skills in adults with cochlear implants (Bansal, 2014). Similarly, some studies showed that teaching CR orally and auditory leads to improved learning, attention, and memory for individuals with hearing impairments (Amani et al., 2017).
In explaining the results of this study, it can be suggested that CR training aids in fostering awareness of emotions and their regulation among children with hearing impairment. Emotion regulation plays a pivotal role in mental well-being and influences an individual’s response to various stimuli (O’Connor et al., 2018). When children with hearing impairment learn to connect with their emotions and talk about them with some strategies like playing with toys, they can manage their emotions, experience less anxiety, and have high self-regulation of emotions. In the context of children’s externalizing behaviors, poor emotion regulation and inattention emerged as significant predictors (Hill et al., 2006). Conversely, providing children with hearing impairment opportunities to engage in group discussions and interactions can enhance their social skills. Consequently, this improvement in social skills may facilitate their emotions management compared to previous proficiency levels (Goldenberg et al., 2016).
Furthermore, children in CR sessions acquire cognitive strategies to regulate their emotions, including cognitive avoidance. Cognitive avoidance involves techniques, such as downplaying the significance of stressors or redirecting focus toward positive thoughts, which can effectively regulate internal stress. Avoidance strategies are negatively associated with depression in children and adolescents (Goldenberg et al., 2016). One objective of CR training is to enhance working memory capacity. A correlation is observed between working memory proficiency and the self-regulation of emotions (Schmeichel et al., 2008). Therefore, when the capacity of working memory of deaf children increases through cognitive training, they can use emotion regulation strategies better than in the past in situations that utilize cognitive resources, such as cognitive evaluation and positive reappraisal.
In elucidating the results of the current study, CR therapy can be an effective intervention for addressing behavioral issues in children with hearing impairment. According to a study by Schorr et al. (2005), CR therapy improves cognitive skills, such as attention, memory, and problem-solving, which are often compromised in children with hearing impairments. These improvements can lead to better self-regulation and reduced impulsivity, ultimately decreasing behavioral problems. Also, CR can improve inhibition and self-control. Although executive function and cognitive control are not synonymous with self-regulation, they represent the top-down components of self-regulation at the cognitive level (Nigg, 2017). Therefore, when children with hearing impairment did the inhibition training, it became easier for them to manage their behaviors. By improving behavior inhibition, the rate of aggression and hyperactivity in children with hearing impairment is reduced. Cognitive training aims to target and improve the cognitive deficits believed to be at the core of ADHD. (Castellanos et al., 2006). The internal behaviors, such as anxiety and depression are reduced in children with hearing impairment in this research. This is consistent with the results of Rahmanian et al. (2018). A crucial relationship exists between anxiety and executive functions (Sohlberg & Mateer, 2001). As children with hearing impairment learn to concentrate their attention on alternative stimuli, they may potentially experience reduced anxiety levels.
In this study, children with hearing impairment learn to pay attention to behaviors related to their emotions. Therefore this training enhances ESR and modifies the behaviors. Cognitive training reduces violence and aggression in children with hearing impairment. The effects of cognitive training may be associated with improvements in problem-solving and increased ability to develop alternative strategies. CR programs are structured educational and cognitive measures that emphasize behavioral and attentional problems and improve remembering daily activities (Bansal, 2014). Since a CR program includes homework and exercises focusing on executive function skills, along with educational guidelines for doing this homework; therefore, it is not surprising that a CR program may help alleviate specific behavioral issues in children with hearing impairments.
This study has several limitations that should be acknowledged before extending its results. One of the significant limitations is that only children with hearing impairments from Yazd City were included in the sample. Consequently, the result cannot be generalized to other regions and nations. In addition, we cannot control the social-cultural differences in children and their families. Finally, we do not have any questions that are adapted for people with hearing impairment. For future studies, it is suggested that computer-based CR for children with hearing impairment be used.
Conclusion
The present study demonstrated that CR interventions effectively reduce behavioral problems and increase hearing impaired children’s ESR. Therefore, planning an educational program of CR is vital in improving children’s behavioral and emotional problems and can be used in schools and rehabilitation centers for children with hearing impairment.
Ethical Considerations
Compliance with ethical guidelines
This study received approval from the Ethics Committee of Science and Culture University, Yazd, Iran (Code: IR.ACECR.JDM.REC.1401.037).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contribute to preparing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank parents of children with hearing impairment and their children for their warm cooperation in the study.
References
Adequate sensory stimuli and typical sensory reception are necessary for the complete development of neural activity (Kral et al., 2016). Hearing impairment is one of the most frequent sensory deficits (Lieu et al., 2020). Sensorineural hearing loss is the most common type of hearing impairment, impacting 1 to 2 out of every 1000 newborns and 1 in 1000 adolescents. Children experiencing hearing impairment encounter challenges in fostering communication skills, comprehending others’ feelings and thoughts, and self-regulation. Consequently, they struggle to form strong bonds with peers, leading to limited social interactions and low emotional management (Morgan et al., 2021). The medical treatment of childhood hearing loss includes hearing aids, cochlear or brainstem implants, enhancement of signal-to-noise ratio in educational environments, speech therapy, and the utilization of sign language (Brennan & Bally, 2007).
Hearing impairment places a child in a challenging position between the hearing and deaf communities, leading to more significant behavioral issues in children with hearing impairment than their hearing peers (Korver et al., 2017).
A relationship exists between internalizing behaviors and hearing impairment in children that may continue even after cochlear implantation. Behavioral issues, such as conduct disorders, hyperactivity, and difficulties with emotional and executive functions in people with hearing impairment may stem from inadequate language development (Bigler et al., 2019). While individuals with hearing impairment are at a higher risk of developing behavioral issues, including elevated aggression, psychopathic traits, oppositional defiant disorder, and other behavioral disorders, some may also experience depression.(Yigider et al., 2020). Individuals with hearing impairment often have a heightened risk of depression, which can potentially lead to suicidal ideation (Adigun, 2017).
Emotional self-regulation (ESR) pertains to comprehending, adapting, and conveying emotions (Domaradzka & Fajkowska, 2018). Individuals with hearing impairment articulate their social and emotional encounters related to hearing loss using terms, such as adverse outcomes, feeling overwhelmed socially, fatigue, bereavement, exclusion, identity influence, emotional distress, frustration, sorrow, anxiety, isolation, and feelings of being burdensome (Bennett et al., 2022). Pensacola et al. reported that participants with hearing loss scored higher on alexithymia and lower for positive relationships. However, no significant differences were observed in emotional regulation between deaf adults and those with typical hearing (Peñacoba et al., 2020). Adults experiencing hearing impairment encounter challenges in recognizing emotions, resulting in lower scores in facial emotion discrimination, cognitive empathy, and tasks involving naming expressions, particularly the expression of fear (Martins et al., 2019). Since a significant and direct correlation is observed between emotional regulation and adaptive environmental behaviors, people with hearing loss show less adaptive behaviors when dealing with the environment because they have problems regulating emotions (Hintermair et al., 2013). On the other hand, one of the crucial components of cognition is emotion regulation (Mahrogi et al., 2021), therefore, if we can improve emotion regulation in hearing-impaired children by improving cognitive components, their behavioral problems may also decrease. Cognitive rehabilitation (CR) therapy significantly reduces cognitive failures and improves emotion regulation (Franco-Martín et al., 2020).
CR aims to identify and tackle individual requirements and objectives, which may involve employing new knowledge or compensatory techniques, such as utilizing memory aids (Bahar‐Fuchs et al., 2013). The meta-analysis results indicate that computer-based CR can be an effective method for cognitive recovery (Nie et al., 2022). Darvishi reported that motored-based CR can improve neuropsychological and orientation in nonverbal learning children (Darvishi et al., 2020). The research results showed that computer-based cognitive training enhances working memory (Oba et al., 2013), executive function, verbal memory, and attention in individuals with cochlear implants (Bansal, 2014). A systematic review study reported that the effect of cognitive training in improving cognition for adults with hearing loss is very low (Lawrence et al., 2018).
Since hearing impairment is linked to higher levels of mental distress, it can impact daily functioning and overall health (Dalton et al., 2003), interventions are required to reduce some behavioral issues in children with hearing impairment to improve psychological functioning. Due to the lack of agreement on the effectiveness of CR on the mental health of children with hearing impairment and the lack of research about the effectiveness of CR on behavioral problems of children with hearing impairment in Iran, this study was conducted to determine the effectiveness of CR programs on behavioral problems and ESR in children with hearing impairment.
Materials and Methods
Study design
The present research was a quasi-experimental study with a pre-test-post-test design and a control group. The study samples included 24 girls with hearing impairments aged 7 to 11 years living in Yazd City, Iran. They were randomly chosen using a convenience sampling method from children with hearing impairment referring to Naghmeh Clinic. A clinic audiologist assessed the level of hearing impairment of these children. Then the children were randomly split into two groups of 12 (intervention and control). The inclusion criteria included an age range from 7 to 11 years, a diagnosis of mild (hearing loss of 20 to 40 decibels) and moderate hearing impairment (hearing loss of 41 to 60 decibels) as assessed by an audiologist, no mental disability based on the children’s Wechsler test (score above 70) and no epilepsy or seizure. The exclusion criteria included cochlear implants, incomplete questionnaires, and non-participation in training sessions. Before beginning the research, the objective and process were presented to all participants. The mothers of the children in the sample group were present to cooperate in completing the children’s questionnaires in the research.
The intervention group underwent 10 sessions of a CR program based on Samuel (2008) and Nazarboland et al. (2019)., CR protocol. In this research, two protocols developed in Iran and abroad have been used to make them more suitable for Iranian children with hearing loss. Experts have checked the validity of this protocol. The CR package is an educational protocol based on Captain’s log cognitive trainer. This protocol helps improve memory, attention, perception, reasoning, planning, and emotional management. Although this protocol can be used with computers, in our research, this protocol was used for children based on computers and play with toys concerning ethical issues. After the end of the study, CR treatment was also performed for the control group.
Table 1 presents the educational content of the sessions. Each meeting lasted 90 minutes (two sessions every week). Since the children had hearing impairment, most of the exercises were based on images and games and emojis to regulate emotions. The control group did not receive the treatment.
Study instruments
Conners’ parent rating scale (CPRS)
The CPRS is a widely recognized tool in research and clinical practice for collecting parents’ observations on behavioral issues in children. The parent form has 48 items that parents fill out. Parents use the Likert scale to fill each item, and the answering spectrum starts with 0 (not true at all, never, or barely) to 3 (entirely true, mostly, almost always). Subscales of Conner’s test include cognitive problems, oppositional, hyperactive-impulsivity, anxiety-shy, perfectionism, social problems, and psychosomatic (Conners et al., 1998). The test reliability was reported between 0.41 to 0.57 for all scales (Gianarris et al., 2001). Factor analysis of this questionnaire in Iran showed four factors, including conduct problems, social problems, anxiety-shy, and psychosomatic problems. External problems are conduct and social problems. Internal problems include anxiety-shy and psychosomatic. In Iran, the validity and reliability of questionnaire for the re-test method was 0.58. Also the Cronbach α method, the coefficient of internal consistency of this questionnaire was 0/73 (Shahaeian et al., 2007). The Cronbach α was 0.75 in this research. Parents completed the questionnaire for their children.
ESR questionnaire (ESRQ)
The ESRQ includes 20 items, each rated on a 5-point Likert scale, where five represents “completely true about me” and one signifies “never true about me.” The possible scores range from 20 to 100. After translation and back-translation, psychology experts, to ensure both validity and content validity, reviewed the questionnaire, which was confirmed. This questionnaire assesses three key components or sub-scales, secrecy, compromise, and tolerance, with 5, 7, and 8 items assigned to each. Cronbach’s α reliability for the sub-scales of secrecy, compromise, and tolerance were calculated at 0.70, 0.68, and 0.50, with an overall reliability of 0.81. Additionally, indicator validity was satisfactory (Hofmann & Kashdan, 2010). In Iran, reliability and validity scores were reported as 0.70, 0.75, and 0.50 for the sub-scales, with an overall reliability of 0.81 (Karashki, 2013). In the present study, Cronbach’s α values for secrecy, compromise, and tolerance were 0.72, 0.7, and 0.69, respectively, and 0.76. For this research, parents filled out the questionnaire on behalf of their children.
Interventional sessions
The experimental group’s participants performed two sessions every week and underwent 10 CR therapy sessions. Each meeting lasted 90 minutes. Since the children had hearing impairment, most of the exercises were based on images and games and emojis to regulate emotions. The control group did not receive the treatment. Table 1 presents the educational content of the sessions.
Results
Twenty-four girls aged between 7 and 11 (mean age=9.17±3.32 years) with hearing impairment participated in the study. Their mean hearing score was 54.65 dB. All participants utilized hearing aids; none underwent cochlear implantation. Table 2 presents the demographic characteristics of the subjects. The study found no significant difference in the speech levels of the children. Only three children over three years old experienced hearing disability and used hearing aids.
Table 3 presents the Mean±SD of the behavioral problems and ESR.
As shown in Table 3, the mean scores of behavioral problems in the intervention group decreased after the treatment and the scores of ESR increased after treatment. We use ANCOVA to search more about these observed differences. Before testing the hypothesis, the Kolmogorov-Smirnov test was utilized to examine the normality of scores for both variables, and the non-significance variables showed that their distribution was normal (P>0.05). According to Levine’s test and the non-significance of all variables, the assumption of the equality of inter-group variances for behavioral problems was also met (P≤005, F=8.2), and self-emotional regulation (P≤0.05, F=10.3). Also, the condition of variance-covariance material was established based on Box’s M test, which was insignificant for all variables (Box’s M=4.17, F=1.12). To evaluate whether there are statistically significant differences between the experimental and control groups, we employ a multivariate analysis of covariance (MANCOVA).
Table 4 presents the results of a MANCOVA conducted to assess the impact of a CR program on three dependent variables. All four tests statistics indicate statistically significant differences between the experimental and control groups (P<0.0001). The large values of Pillai’s Trace, Wilks’ Lambda, Hotelling’s trace, and Roy’s largest root confirm the robustness of the results. The partial eta squared value of 0.814 suggests that the CR program can explain a substantial proportion of the variability in the dependent variables. The results of multivariate analysis of covariance (ANCOVA) were designed to assess the impact of CR programs on three dependent variables, internal problems, external problems, and ESR.
The results of Table 5 showed CR significantly enhances internal problems (P≤0.05, F=43.12, Eta=0.89), external problems (P≤0.05, F=32.18, Eta=0.67), and ESR (P≤0.05, F=44.05, Eta=0.67), as evidenced by the high F and effect sizes across all measured variables.
Discussion
The current research was conducted to investigate the effect of CR programs on the behavioral and emotional self-regulating problems of children with hearing impairment. Hearing impairment is common worldwide, and diagnosing and intervening before six months of age ensures normal language development, regardless of the severity of the hearing loss (Yoshinaga-Itano et al., 2020). This study supports the concept that managing behavioral problems in children with hearing impairment is improved after performing CR therapy. The current study’s results are not consistent with the results of Lawrence et al., (2018), that reported CR has a low effect on improving cognition in adults with hearing impairment. Still, these results are consistent with the results of Bansal, (2014), which reflected cognitive training has a modest positive effect on executive function and working memory skills in adults with cochlear implants (Bansal, 2014). Similarly, some studies showed that teaching CR orally and auditory leads to improved learning, attention, and memory for individuals with hearing impairments (Amani et al., 2017).
In explaining the results of this study, it can be suggested that CR training aids in fostering awareness of emotions and their regulation among children with hearing impairment. Emotion regulation plays a pivotal role in mental well-being and influences an individual’s response to various stimuli (O’Connor et al., 2018). When children with hearing impairment learn to connect with their emotions and talk about them with some strategies like playing with toys, they can manage their emotions, experience less anxiety, and have high self-regulation of emotions. In the context of children’s externalizing behaviors, poor emotion regulation and inattention emerged as significant predictors (Hill et al., 2006). Conversely, providing children with hearing impairment opportunities to engage in group discussions and interactions can enhance their social skills. Consequently, this improvement in social skills may facilitate their emotions management compared to previous proficiency levels (Goldenberg et al., 2016).
Furthermore, children in CR sessions acquire cognitive strategies to regulate their emotions, including cognitive avoidance. Cognitive avoidance involves techniques, such as downplaying the significance of stressors or redirecting focus toward positive thoughts, which can effectively regulate internal stress. Avoidance strategies are negatively associated with depression in children and adolescents (Goldenberg et al., 2016). One objective of CR training is to enhance working memory capacity. A correlation is observed between working memory proficiency and the self-regulation of emotions (Schmeichel et al., 2008). Therefore, when the capacity of working memory of deaf children increases through cognitive training, they can use emotion regulation strategies better than in the past in situations that utilize cognitive resources, such as cognitive evaluation and positive reappraisal.
In elucidating the results of the current study, CR therapy can be an effective intervention for addressing behavioral issues in children with hearing impairment. According to a study by Schorr et al. (2005), CR therapy improves cognitive skills, such as attention, memory, and problem-solving, which are often compromised in children with hearing impairments. These improvements can lead to better self-regulation and reduced impulsivity, ultimately decreasing behavioral problems. Also, CR can improve inhibition and self-control. Although executive function and cognitive control are not synonymous with self-regulation, they represent the top-down components of self-regulation at the cognitive level (Nigg, 2017). Therefore, when children with hearing impairment did the inhibition training, it became easier for them to manage their behaviors. By improving behavior inhibition, the rate of aggression and hyperactivity in children with hearing impairment is reduced. Cognitive training aims to target and improve the cognitive deficits believed to be at the core of ADHD. (Castellanos et al., 2006). The internal behaviors, such as anxiety and depression are reduced in children with hearing impairment in this research. This is consistent with the results of Rahmanian et al. (2018). A crucial relationship exists between anxiety and executive functions (Sohlberg & Mateer, 2001). As children with hearing impairment learn to concentrate their attention on alternative stimuli, they may potentially experience reduced anxiety levels.
In this study, children with hearing impairment learn to pay attention to behaviors related to their emotions. Therefore this training enhances ESR and modifies the behaviors. Cognitive training reduces violence and aggression in children with hearing impairment. The effects of cognitive training may be associated with improvements in problem-solving and increased ability to develop alternative strategies. CR programs are structured educational and cognitive measures that emphasize behavioral and attentional problems and improve remembering daily activities (Bansal, 2014). Since a CR program includes homework and exercises focusing on executive function skills, along with educational guidelines for doing this homework; therefore, it is not surprising that a CR program may help alleviate specific behavioral issues in children with hearing impairments.
This study has several limitations that should be acknowledged before extending its results. One of the significant limitations is that only children with hearing impairments from Yazd City were included in the sample. Consequently, the result cannot be generalized to other regions and nations. In addition, we cannot control the social-cultural differences in children and their families. Finally, we do not have any questions that are adapted for people with hearing impairment. For future studies, it is suggested that computer-based CR for children with hearing impairment be used.
Conclusion
The present study demonstrated that CR interventions effectively reduce behavioral problems and increase hearing impaired children’s ESR. Therefore, planning an educational program of CR is vital in improving children’s behavioral and emotional problems and can be used in schools and rehabilitation centers for children with hearing impairment.
Ethical Considerations
Compliance with ethical guidelines
This study received approval from the Ethics Committee of Science and Culture University, Yazd, Iran (Code: IR.ACECR.JDM.REC.1401.037).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contribute to preparing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank parents of children with hearing impairment and their children for their warm cooperation in the study.
References
Adigun, O. T. (2017). Depression and individuals with hearing loss: A systematic review. Journal of Psychology & Psychotherapy, 7(5), 1-6. [DOI:10.4172/2161-0487.1000323]
Amani, O., Mazaheri, M. A., Nejati, V., & Shamsian, S. (2017). [Effectiveness of cognitive rehabilitation in executive functions (attention and working memory) in adolescents survived from acute lymphoblastic leukemia with a history of chemotherapy: A randomized clinical trial (Persian)]. Journal of Mazandaran University of Medical Sciences, 27(147), 126-138. [Link]
Bahar‐Fuchs, A., Clare, L., & Woods, B. (2013). Cognitive training and cognitive rehabilitation for mild to moderate Alzheimer’s disease and vascular dementia. The Cochrane Database of Systematic Reviews, 2013(6), CD003260. [DOI:10.1002/14651858.CD003260.pub2] [PMID]
Bansal, A. (2014). Evaluating the short-term effects of home-based computerized multi-domain cognitive training in adult cochlear implant users: A prospective randomized intervention study [MA thesis]. Oslo: University of Oslo. [DOI:10.13140/2.1.2365.1523]
Bennett, R. J., Saulsman, L., Eikelboom, R. H., & Olaithe, M. (2022). Coping with the social challenges and emotional distress associated with hearing loss: A qualitative investigation using Leventhal’s self-regulation theory. International Journal of Audiology, 61(5), 353-364. [DOI:10.1080/14992027.2021.1933620] [PMID]
Bigler, D., Burke, K., Laureano, N., Alfonso, K., Jacobs, J., & Bush, M. L. (2019). Assessment and treatment of behavioral disorders in children with hearing loss: A systematic review. Otolaryngology-Head and Neck Surgery, 160(1), 36-48. [DOI:10.1177/0194599818797598] [PMID]
Brennan, M., & Bally, S. J. (2007). Psychosocial adaptations to dual sensory loss in middle and late adulthood. Trends in Amplification, 11(4), 281-300. [DOI:10.1177/1084713807308210] [PMID]
Castellanos, F. X., Sonuga-Barke, E. J., Milham, M. P., & Tannock, R. (2006). Characterizing cognition in ADHD: beyond executive dysfunction. Trends in Cognitive Sciences, 10(3), 117-123. [DOI:10.1016/j.tics.2006.01.011] [PMID]
Conners, C. K., Sitarenios, G., Parker, J. D., & Epstein, J. N. (1998). The revised Conners’ Parent Rating Scale (CPRS-R): factor structure, reliability, and criterion validity. Journal of Abnormal Child Psychology, 26(4), 257-268. [DOI:10.1023/A:1022602400621] [PMID]
Dalton, D. S., Cruickshanks, K. J., Klein, B. E., Klein, R., Wiley, T. L., & Nondahl, D. M. (2003). The impact of hearing loss on quality of life in older adults. The Gerontologist, 43(5), 661-668. [DOI:10.1093/geront/43.5.661] [PMID]
Darvishi, E., Demehri, F., Saedmanesh, M., & Abooyi, A. (2020). Investigating the effectiveness of motor based cognitive rehabilitation on orientation and neuropsychological symptoms in children with non-verbal learning disorder. Journal of Learning Disabilities, 10(1), 70-86. [Link]
Domaradzka, E., & Fajkowska, M. (2018). Cognitive emotion regulation strategies in anxiety and depression understood as types of personality. Frontiers in Psychology, 9, 856. [DOI:10.3389/fpsyg.2018.00856] [PMID]
Gianarris, W. J., Golden, C. J., & Greene, L. (2001). The CONNERS’PARENT rating scales: A critical review of the literature. Clinical Psychology Review, 21(7), 1061-1093. [DOI:10.1016/S0272-7358(00)00085-4] [PMID]
Goldenberg, A., Halperin, E., Van Zomeren, M., & Gross, J. J. (2016). The process model of group-based emotion: Integrating intergroup emotion and emotion regulation perspectives. Personality and social Psychology Review, 20(2), 118-141.[ [DOI:10.1177/1088868315581263] [PMID]
Franco-Martín, M. A., Diaz-Baquero, A. A., Bueno-Aguado, Y., Cid-Bartolomé, M. T., Parra Vidales, E., & Perea Bartolomé, M. V., et al. (2020). Computer-based cognitive rehabilitation program GRADIOR for mild dementia and mild cognitive impairment: New features. BMC Medical Informatics and Decision Making, 20(1), 274. [DOI:10.1186/s12911-020-01293-w] [PMID]
Hill, A. L., Degnan, K. A., Calkins, S. D., & Keane, S. P. (2006). Profiles of externalizing behavior problems for boys and girls across preschool: The roles of emotion regulation and inattention. Developmental Psychology, 42(5), 913. [DOI:10.1037/0012-1649.42.5.913] [PMID]
Hintermair, M. (2013). Executive functions and behavioral problems in deaf and hard-of-hearing students at general and special schools. Journal of Deaf Studies and Deaf Education, 18(3), 344-359. [PMID]
Hofmann, S. G., & Kashdan, T. B. (2010). The affective style questionnaire: Development and psychometric properties. Journal of Psychopathology and Behavioral Assessment, 32(2), 255–263. [DOI:10.1007/s10862-009-9142-4] [PMID]
Karashki, H. (2013). [Evaluating factorial structure of emotional styles in students (Persian)]. Journal of Research in Behavioural Sciences, 11(3), 185-195. [Link]
Kral, A., Kronenberger, W. G., Pisoni, D. B., & O’Donoghue, G. M. (2016). Neurocognitive factors in sensory restoration of early deafness: A connectome model. The Lancet. Neurology, 15(6), 610–621. [DOI:10.1016/S1474-4422(16)00034-X] [PMID]
Lawrence, B. J., Jayakody, D. M. P., Henshaw, H., Ferguson, M. A., Eikelboom, R. H., & Loftus, A. M., et al. (2018). Auditory and cognitive training for cognition in adults with hearing loss: A systematic review and meta-analysis. Trends in Hearing, 22, 2331216518792096. [DOI:10.1177/2331216518792096] [PMID]
Lieu, J. E. C., Kenna, M., Anne, S., & Davidson, L. (2020). Hearing loss in children: A review. JAMA, 324(21), 2195–2205. [DOI:10.1001/jama.2020.17647] [PMID]
Korver, A. M., Smith, R. J., Van Camp, G., Schleiss, M. R., Bitner-Glindzicz, M. A., & Lustig, L. R., et al. (2017). Congenital hearing loss. Nature Reviews. Disease Primers, 3, 16094. [PMID]
Martins, A. T., Faísca, L., Vieira, H., & Gonçalves, G. (2019). Emotional recognition and empathy both in deaf and blind adults. Journal of Deaf Studies and Deaf Education, 24(2), 119–127. [PMID]
Mahrogi, H., Tozandehjani, H., Nejat, H., & Bagherzadeh-gholmakani, Z. (2021). [Comparing the effectiveness of cognitive rehabilitation based on attention amplification and cognitive rehabilitation based on working memory amplification in cognitive emotion regulation and information processing speed of dyslexic students (Persian)]. Neuropsychology, 7(25), 73-92. [DOI:10.30473/clpsy.2020.52835.1544]
Morgan, G., Curtin, M., & Botting, N. (2021). The interplay between early social interaction, language and executive function development in deaf and hearing infants. Infant Behavior & Development, 64, 101591. [DOI:10.1016/j.infbeh.2021.101591] [PMID]
Nazarboland, N., Tahmasi, A., & Nejati, V. (2019). [Effectiveness of cognitive rehabilitation based on “ARAM” program in improving executive functions of selective attention and inhibitory control in elderly people with mild cognitive impairment (Persian)]. Journal of Cognitive Psychology, 7(3), 40-59. [Link]
Nie, P., Liu, F., Lin, S., Guo, J., Chen, X., Chen, S., & Yu, L ., et al. (2022). The effects of computer-assisted cognitive rehabilitation on cognitive impairment after stroke: A systematic review and meta-analysis. Journal of Clinical Nursing, 31(9-10), 1136-1148. [DOI:10.1111/jocn.16030]
Nigg, J. T. (2017). Annual research review: On the relations among self‐regulation, self‐control, executive functioning, effortful control, cognitive control, impulsivity, risk‐taking, and inhibition for developmental psychopathology. Journal of Child Psychology and Psychiatry, 58(4), 361-383. [DOI:10.1111/jcpp.12675] [PMID]
O’Connor, C. A., Dyson, J., Cowdell, F., & Watson, R. (2018).Do universal school‐based mental health promotion programmes improve the mental health and emotional wellbeing of young people? A literature review. Journal of Clinical Nursing, 27(3-4), e412-e426. [PMID]
Oba, S. I., Galvin, J. J., 3rd, & Fu, Q. J. (2013). Minimal effects of visual memory training on the auditory performance of adult cochlear implant users. Journal of Rehabilitation Research and Development, 50(1), 99-110. [PMID]
Peñacoba, C., Garvi, D., Gómez, L., & Álvarez, A. (2020). Emotional functioning, positive relationships, and language use in deaf adults. Journal of Deaf Studies and Deaf Education, 25(1), 22-32. [DOI:10.1093/deafed/enz034] [PMID]
Rahmanian, M., Mohtarami, S., & Dehestani, M. (2018). [The effect of cognitive rehabilitation training on improving anxiety symptoms in children (Persian)]. Journal of Child Mental Health, 5(1), 48-58. [Link]
Samuel, R. (2008). Cognitive rehabilitation for reversible and progressive brain injury. Indian Journal of Psychiatry, 50(4), 282-284. [DOI:10.4103/0019-5545.44752] [PMID]
Schmeichel, B. J., Volokhov, R. N., & Demaree, H. A. (2008). Working memory capacity and the self-regulation of emotional expression and experience. Journal of Personality and Social Psychology, 95(6), 1526-1540. [DOI:10.1037/a0013345] [PMID]
Shahaeian, A., Shahim, S., Bashash, L., & Yousefi, F. (2007). [Standardization, factor analysis and reliability of the conners parents rating scales for 6 to 11 years old children Shiraz. Journal of Educational Psychology Studies, 3(3), 97-120. [Link]
Sohlberg, M. M., & Mateer, C. A. (2001). Improving attention and managing attentional problems: Adapting rehabilitation techniques to adults with ADD. Annals of the New York Academy of Sciences, 931(1), 359-375. [DOI:10.1111/j.1749-6632.2001.tb05790.x]
Schorr, E. A., Fox, N. A., van Wassenhove, V., & Knudsen, E. I. (2005). Auditory-visual fusion in speech perception in children with cochlear implants. Proceedings of the National Academy of Sciences of the United States of America, 102(51), 18748–18750. [DOI:10.1073/pnas.0508862102] [PMID]
Yigider, A. P., Yilmaz, S., Ulusoy, H., Kara, T., Kufeciler, L., & Kaya, K. H. (2020). Emotional and behavioral problems in children and adolescents with hearing loss and their effects on quality of life. International Journal of Pediatric Otorhinolaryngology, 137, 110245. [DOI:10.1016/j.ijporl.2020.110245] [PMID]
Type of Study: Original Research Article |
Subject:
Rehabilitation
Received: 2024/08/27 | Accepted: 2024/11/11 | Published: 2025/01/1
Received: 2024/08/27 | Accepted: 2024/11/11 | Published: 2025/01/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
