

Volume 7, Issue 4 (Autumn 2019)
PCP 2019, 7(4): 245-253 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammad-Aminzadeh D, Abasi A, Asmari-Bardezard Y, Kazemian S, Younesi S J. Comparing Emotion Regulation Strategies and Adjustment Between Students With Physical Disability and Healthy Students. PCP 2019; 7 (4) :245-253
URL: http://jpcp.uswr.ac.ir/article-1-652-en.html
URL: http://jpcp.uswr.ac.ir/article-1-652-en.html
Dana Mohammad-Aminzadeh1 

 , Amir Abasi * 1, Yousef Asmari-Bardezard2 , Somaye Kazemian3 , Seyed Jalal Younesi3
, Amir Abasi * 1, Yousef Asmari-Bardezard2 , Somaye Kazemian3 , Seyed Jalal Younesi3
, Amir Abasi * 1, Yousef Asmari-Bardezard2 , Somaye Kazemian3 , Seyed Jalal Younesi3
1- Department of Counseling, Faculty of Psychology and Education, Allameh Tabataba’i University, Tehran, Iran.
2- Department of Clinical Psychology, the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Counseling, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Clinical Psychology, the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Counseling, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Keywords: Emotion regulation strategies, Adjustment, Students with a physical disability, Normal students
Full-Text [PDF 676 kb]
(2193 Downloads)
| Abstract (HTML) (3425 Views)

Both groups were matched according to their educational level, similarly, and demographic characteristics. The number of middle-school students in both groups was 38. The mean age of the group with disabilities was 13.61 years, and in the healthy group, it was 13.20 years. Furthermore, the number of high-school students in both was 62; the mean age of the group with disabilities was 16.49 years and it was 15.89 years in the healthy group.
To analyze the acquired data, Pearson’s correlation analysis and MANCOVA were applied. Before using MANCOVA, to comply with its assumptions was used Levene’s test and Box test; the condition of homogeneity of variance matrices of variance/covariance was respected. These test results were not significant for any of the variables. As a result of the use of parametric tests was allowed. Significance levels of all tests allowed the use of MANCOVA.
The descriptive analysis results of the study groups (mean±SD) are presented in Table 1.
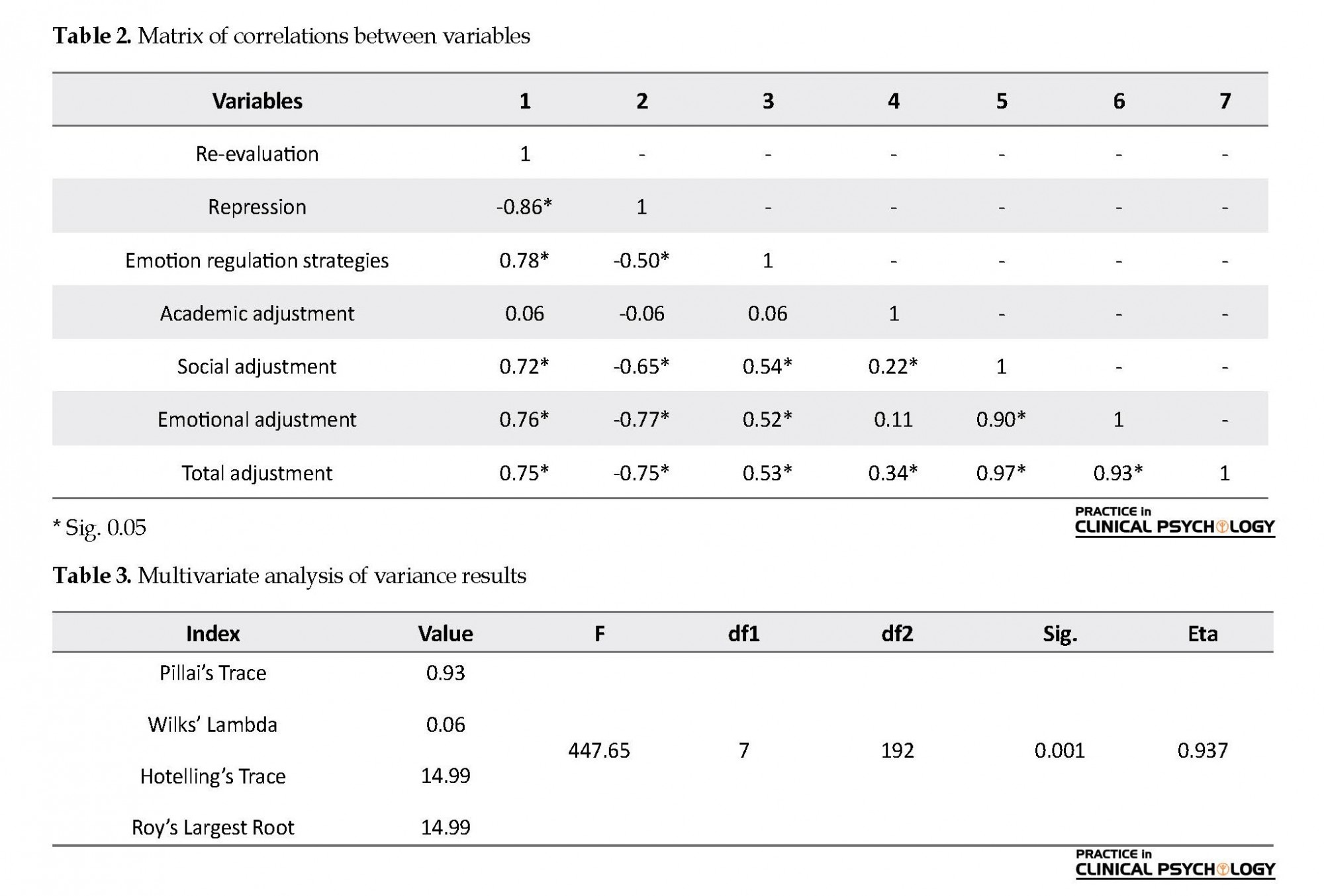
As per Table 2, re-evaluation, as a subscale of emotion regulation strategies, had a positive and significant relationship with adaptation in three educational, social, and emotional areas. Moreover, repression, as another subscale of emotion regulation strategies, had a negative relationship with adjustment in different educational, social, and emotional aspects.
According to Table 3, the effect of the group on the linear combination of dependent variables was significant. Thus, it indicates that the two study groups were significantly different in a combination of dependent variables (repression, re-evaluation, and adjustment) in Pillai’s trace, Wilks’ Lambda, Hotelling’s Trace, and Roy’s Largest Root with the estimates of an effect size equal to 0.93.
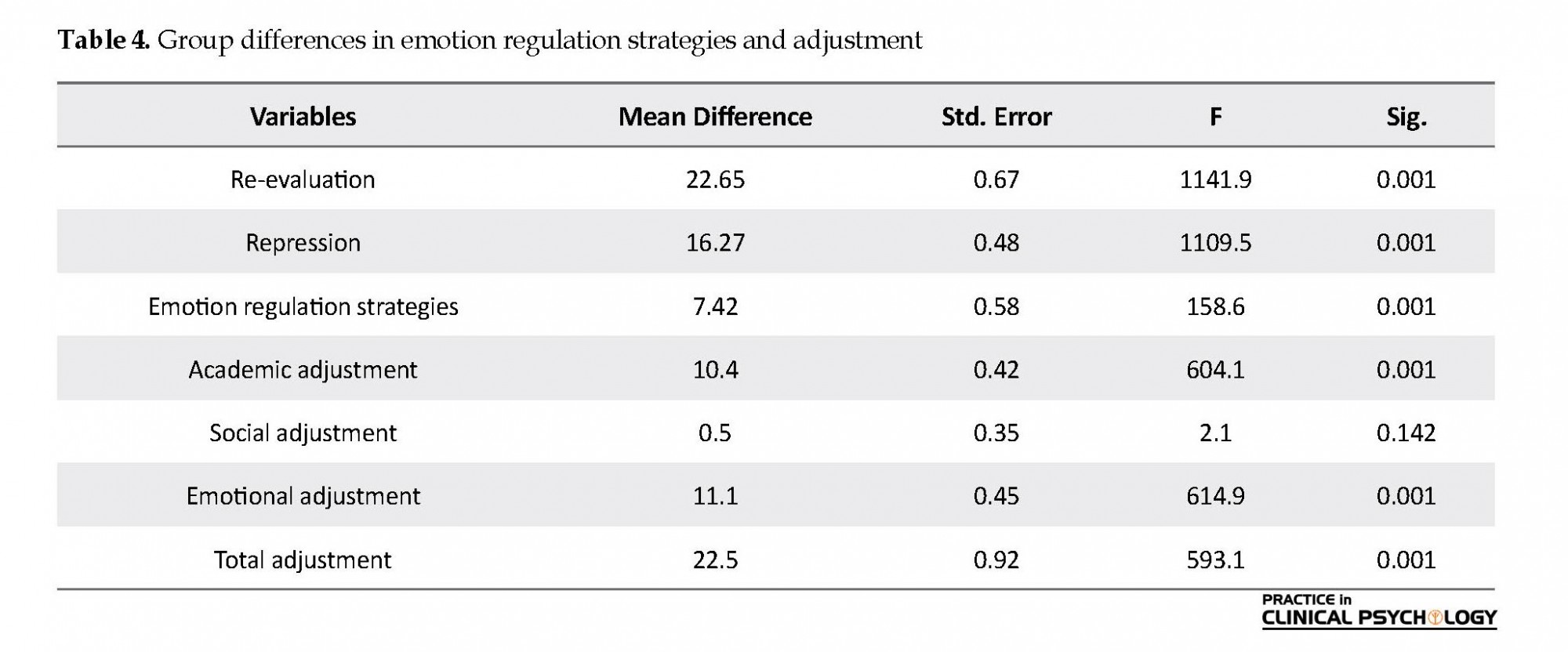
According to Table 4, for each dependent variable, data analysis (using Bonferroni alpha of 0.017 and the degrees of freedom 1, 198) suggested that education, as a dimension of adjustment was not significantly different between the two groups.
4. Discussion
The present study examined social adjustment and the use of emotion regulation strategies among students with physical/mobility disabilities and healthy students. According to the study findings, there was a positive and significant relationship between social adjustment and reappraisal (r=0.72) and a significant negative relationship between suppression and social adjustment (r=-0.65); these findings indicated that emotional reappraisal, as an emotion regulation strategy, improved social adjustment; however, emotional suppression decreased social adjustment. There was also a significant difference between the two groups regarding the use of emotion regulation strategies (suppression and reappraisal); these findings indicate that compared to healthy students, those with physical/mobility disabilities were less capable of managing or regulating their emotional responses and coping with stressful or unpleasant life events. There was no previous study precisely similar to the present one. However, Garnefski and Kraaij argued that emotion regulation strategies were associated with psychological distress and significantly predicted subsequent adjustment (Garnefski & Kraaij, 2006). Mennin et al. (2007) also reported that those who were not able to efficiently manage their emotions against daily life events indicated more diagnostic symptoms of internalizing disorders, like depression and anxiety.
This population has emotional problems, mental health issues, misinterpretations, focus on the negative aspects of life, and feel the lack of control over the internal and external world (which may be related to their developmental impairments). Thus, students with physical/mobility disabilities tend to use negative emotion regulation strategies in the face of stressful or unpleasant events; in contrast, healthy students, in such events, tend to use adaptive emotion regulation strategies, such as making positive reappraisals, considering adverse events as unimportant or less unpleasant than other events, and having a feeling of control over the internal and external world. Therefore, the second group is less vulnerable to emotional problems. This suggests that students less capable of managing their emotions in the face of daily life events, experience more psychological distress. Such distress may lead to depression and anxiety; contrarily, effective emotion regulation is related to healthier relationships, better academic performance, and better physical health.
Another study indicated a significant difference between the scores of students with physical/mobility disabilities and healthy students in two subscales of social adjustment; the emotional and social adjustment subscales. However, no significant difference was found between the two groups in the academic adjustment subscale. This finding is in line with those of Sharma (Sharma, 2004), wiener (Wiener, 2004), Sideritis (Sideridis, 2007; Auerbach, Gross-Tsur, Manor, & Shalev, 2008; Freilich & Shechtman, 2010), indicating that disabled children and adolescents have higher rates of social and emotional problems, compared to their healthy counterparts.
The study finding indicating decreased social adjustment in students with physical/mobility disabilities could be explained by the fact that, like physical development, social development is a continuous process; i.e. it is gradually achieved during different life stages through g various experiences. Furthermore, it is among the most important signs of desirable mental health status in adolescents. In other words, an individual is considered to have reasonable adjustment only when being able to have a healthy relationship with their social environment; otherwise, a proper adjustment cannot be achieved by the person. However, research indicates that, due to facing numerous problems in life as well as poor interpersonal skills, adolescents with disabilities often have poor mental health (Sideridis, 2007), experience higher social rejection and loneliness (Estell et al., 2008), and are less popular than their healthy peers. Additionally, because of their developmental problems, students with physical/mobility disabilities tend to develop impairments in their performance and adjustment. This matter results from experiences, such as their peers’ success, love failure, and losing motivation for life. When adolescents are unable to successfully overcome developmental challenges, they experience psychological distress and considerable impairments in the emotional and social aspects of their lives. In addition, students with physical/mobility disabilities perceive themselves as different from others and tend to evaluate their appearance negatively. Therefore, they are more prone to experience social problems and ignorance by others; as a result, they may demonstrate a poor adjustment.
It the present study, no significant difference was observed in academic adjustment between the study groups. No previous finding consistent with this result was detected; however, in contrast to this finding, in a study by Zahed, Rajabi, & Omidi (2012) on social, emotional, academic, and self-regulating learning, a significant difference was found between students with and without learning disabilities (“a comparison of social, emotional and educational adjustment and self-regulated learning in students with and without learning disabilities”, 2012). This finding can also be explained using the inferiority complex (Adler’s theory). Adler stated that actual mental or physical inferiority could be a source of inferiority feelings. He believed that physical impairment could affect personality and motivate individuals to overcome their impairment or disability. Compensation has a vital role in the feelings of inferiority; it is often used by those with a physical disability to cover disability and impairment, to create a new balance in the organism. Therefore, the lack of difference between physical disability and academic achievement could be attributed to the use of compensation by adolescents with disabilities to cope with their impairments and shortcomings.
The present study was only conducted on students with physical disabilities; thus, cautions should be considered in generalizing the obtained outcomes to other rehabilitation communities. Moreover, the study data were achieved based on self-report (questionnaire); therefore, the collected results may be biased. As a result, qualitative methods are suggested for better investigation of future research structures.
Future studies are suggested to examine the study variables among female students as well as students with other disabilities, such as visual and auditory impairments. Accordingly, their results can be used to improve the use of adaptive emotion regulation strategies in students with disabilities and help them achieve the optimum level of adjustment in different domains.
Compared to healthy students, their counterparts with physical/mobility disabilities are more likely to use negative emotion regulation strategies, especially suppression; however, healthy students tend to use more positive emotion regulation strategies, especially reappraisal. Therefore, students with physical disabilities benefit from lower emotional and social adjustment, compared to their healthy peers.
Ethical Considerations
Compliance with ethical guidelines
A written informed consent was obtained from the participants prior to the study. They were informed of the study objectives and methods. Participation in the study did not impose any costs on the participants.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Methodology: Dana Mohammad-aminzadeh, Yousef Asmari; Investigation: Seyed Jalal Younesi; Writing-original draft: Dana Mohammad-aminzadeh, Somaye Kazemian, Amir Abasi Writing-review & editing: Seyed Jalal Younesi, somaye Kazemian; Resources: Dana Mohammad-aminzadeh, Amir Abasi Supervision: Seyed Jalal Younesi.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
We would like to express our sincere thanks to the study participants and the schools’ personnel for their cooperation and support.
References
Ahmad, T., Ishfaq, K., & Naeem, S. B. (2013). Impact of physically disability of children on their families; a study in Children Hospital & Institute of Child Health Multan, Pakistan. International Journal of Medicine and Applied Health, 1(2), 46-51.
Auerbach, J. G., Gross-Tsur, V., Manor, O., & Shalev, R. S. (2008). Emotional and behavioral characteristics over a six-year period in youths with persistent and nonpersistent dyscalculia. Journal of Learning Disabilities, 41(3), 263-73. [DOI:10.1177/0022219408315637] [PMID]
Aurora, U. (2014). Study for determining laterality in children with motor disabilities in adapted physical activities. Procedia - Social and Behavioral Sciences, 117, 646-52. [DOI:10.1016/j.sbspro.2014.02.276]
Babapour Kheiroddin, J., & Ahmadi, E. (2013). [A comparison of emotion regulation strategies and mindfulness in students with and without obsessive believes (Persian)]. Journal of Modern Psychological Researches, 7(28), 23-40.
Baurain, C., Nader-Grosbois, N., & Dionne, C. (2013). Socio-emotional regulation in children with intellectual disability and typically developing children, and teachers’ perceptions of their social adjustment. Research in Developmental Disabilities, 34(9), 2774-87. [DOI:10.1016/j.ridd.2013.03.022] [PMID]
Berking, M., Wupperman, P., Reichardt, A., Pejic, T., Dippel, A., & Znoj, H. (2008). Emotion-regulation skills as a treatment target in psychotherapy. Behaviour Research and Therapy, 46(11), 1230-7. [DOI:10.1016/j.brat.2008.08.005] [PMID]
Brown, R. L., & Turner, R. J. (2012). Physical limitation and anger stress exposure and assessing the role of psychosocial resources. Society and Mental Health, 2(2), 69-84. [DOI:10.1177/2156869312444441]
Estell, D. B., Jones, M. H., Pearl, R., Van Acker, R., Farmer, T. W., & Rodkin, P. C. (2008). Peer groups, popularity, and social preference trajectories of social functioning among students with and without learning disabilities. Journal of Learning Disabilities, 41(1), 5-14. [DOI:10.1177/0022219407310993] [PMID]
Estévez López, E., Emler, N. P., Cava, M. J., & Inglés Saura, C. J. (2014). Psychosocial adjustment in aggressive popular and aggressive rejected adolescents at school. Psychosocial Intervention, 23(1), 57-67. [DOI:10.5093/in2014a6]
Fiasse, C., & Nader-Grosbois, N. (2012). Perceived social acceptance, theory of mind and social adjustment in children with intellectual disabilities. Research in Developmental Disabilities, 33(6), 1871-80. [DOI:10.1016/j.ridd.2012.05.017] [PMID]
Freilich, R., & Shechtman, Z. (2010). The contribution of art therapy to the social, emotional, and academic adjustment of children with learning disabilities. The Arts in Psychotherapy, 37(2), 97-105. [DOI:10.1016/j.aip.2010.02.003]
Garnefski, N., & Kraaij, V. (2006). Cognitive Emotion Regulation Questionnaire-development of a short 18-item version (CERQ-short). Personality and Individual Differences, 41(6), 1045-53. [DOI:10.1016/j.paid.2006.04.010]
Gross, J. J., & Jazaieri, H. (2014). Emotion, emotion regulation, and psychopathology an affective science perspective. Clinical Psychological Science, 2(4), 387-401. [DOI:10.1177/2167702614536164]
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348-62. [DOI:10.1037/0022-3514.85.2.348] [PMID]
Halperin, E. (2014). Emotion, emotion regulation, and conflict resolution. Emotion Review, 6(1), 68-76. [DOI:10.1177/1754073913491844]
Hsiao, M. N., Tseng, W. L., Huang, H. Y., & Gau, S. S. (2013). Effects of autistic traits on social and school adjustment in children and adolescents: The moderating roles of age and gender. Research in Developmental Disabilities, 34(1), 254-65. [DOI:10.1016/j.ridd.2012.08.001] [PMID]
Kingston, J., Chadwick, P., Meron, D., & Skinner, T. C. (2007). A pilot randomized control trial investigating the effect of mindfulness practice on pain tolerance, psychological well-being, and physiological activity. Journal of Psychosomatic Research, 62(3), 297-300. [DOI:10.1016/j.jpsychores.2006.10.007] [PMID]
Lucas-Carrasco, R., Eser, E., Hao, Y., McPherson, K. M., Green, A., Kullmann, L., & WHOQOL-DIS Group. (2011). The Quality of Care and Support (QOCS) for people with disability scale: Development and psychometric properties. Research in Developmental Disabilities, 32(3), 1212-25. [DOI:10.1016/j.ridd.2010.12.030] [PMID]
Mennin, D. S., Holaway, R. M., Fresco, D. M., Moore, M. T., & Heimberg, R. G. (2007). Delineating components of emotion and its dysregulation in anxiety and mood psychopathology. Behavior Therapy, 38(3), 284-302. [DOI:10.1016/j.beth.2006.09.001] [PMID]
Mithen, J., Aitken, Z., Ziersch, A., & Kavanagh, A. M. (2015). Inequalities in social capital and health between people with and without disabilities. Social Science & Medicine, 126, 26-35. [DOI:10.1016/j.socscimed.2014.12.009] [PMID]
Nader-Grosbois, N., Houssa, M., & Mazzone, S. (2013). How could theory of mind contribute to the differentiation of social adjustment profiles of children with externalizing behavior disorders and children with intellectual disabilities? Research in Developmental Disabilities, 34(9), 2642-60. [DOI:10.1016/j.ridd.2013.05.010] [PMID]
Nosek, M. A., Hughes, R. B., Swedlund, N., Taylor, H. B., & Swank, P. (2003). Self-esteem and women with disabilities. Social Science & Medicine, 56(8), 1737-47. [DOI:10.1016/S0277-9536(02)00169-7]
Rahmati, B., Adibrad, N., & Tahmasian, K., & Saleh Sedghpour, B. (2010). The effectiveness of life skill training on social adjustment in children. Procedia - Social and Behavioral Sciences, 5, 870-4. [DOI:10.1016/j.sbspro.2010.07.201]
Salehi, M., Kharaz Tavakol, H., Shabani, M., & Ziaei, T. (2015). The relationship between self-esteem and sexual self-concept in people with physical-motor disabilities. Iranian Red Crescent Medical Journal, 17(1), e25359. [DOI:10.5812/ircmj.25359] [PMID] [PMCID]
Sharma, G. (2004). A comparative study of the personality characteristics of primary-school students with learning disabilities and their nonlearning disabled peers. Learning Disability Quarterly, 27(3), 127-40. [DOI:10.2307/1593664]
Sideridis, G. D. (2007). International approaches to learning disabilities: More alike or more different? Learning Disabilities Research & Practice, 22(3), 210-5. [DOI:10.1111/j.1540-5826.2007.00249.x]
Sinha, A., & Singh, R. (2005). Manual for adjustment inventory for school students. Agra: National psychological corporation.
Trani, J. F., & Bakhshi, P. (2008). Challenges for assessing disability prevalence: The case of Afghanistan. Alter, 2(1), 44-64. [DOI:10.1016/j.alter.2007.10.003]
Tull, M. T., Stipelman, B. A., Salters-Pedneault, K., & Gratz, K. L. (2009). An examination of recent non-clinical panic attacks, panic disorder, anxiety sensitivity, and emotion regulation difficulties in the prediction of generalized anxiety disorder in an analogue sample. Journal of Anxiety Disorders, 23(2), 275-82. [DOI:10.1016/j.janxdis.2008.08.002] [PMID]
Varsamis, P., & Agaliotis, I. (2015). Relationships between gross- and fine motor functions, cognitive abilities, and self-regulatory aspects of students with physical disabilities. Research in Developmental Disabilities, 47, 430-40. [DOI:10.1016/j.ridd.2015.10.009] [PMID]
Wiener, J. (2004). Do peer relationships foster behavioral adjustment in children with learning disabilities? Learning Disability Quarterly, 27(1), 21-30. [DOI:10.2307/1593629]
World Health Organization. (2011). World report on disability. Geneva: World Health Organization.
Zahed, A., Rajabi, S., & Omidi, M. (2012). [A comparison of social, emotional and educational adjustment and self-regulated learning in students with and without learning disabilities (Persian)]. Journal of Learning Disabilities, 1(2), 43-62.
Full-Text: (1681 Views)
1. Introduction
Disability, as an impairment, limits an individual’s one or more major life activities (Brown & Turner, 2012). Moreover, it is often accompanied by reduced self-esteem (Nosek, Hughes, Swedlund, Taylor, & Swank, 2003; Salehi, Tavakol, Shabani, & Ziaei, 2015), psychological distress (Trani & Bakhshi, 2008).Disability has been used by the World Health Organization (WHO) in the International Classification of Functioning, Disability and Health (ICF) as an umbrella term for impairments, functional limitations, and participation limitations (Lucas-Carrasco et al., 2011). It is resulted in physical impairments (Aurora, 2014) and deprived independent participation in personal and social activities (Salehi et al., 2015). Physical disability, as part of a broad range of disabilities, involves failure to use one limb or part of it for at least 6 months (Bahrampour, Ghamari, & Amiri Majd, 2014). According to the WHO, nearly 1 billion people throughout the world have some disability (World Health Organization 2011). Additionally, more than one-third of them live in developing countries (Bahrampour et al., 2014).
Disability in every life aspect leads to the impaired natural and harmonious development of the person (Aurora, 2014), psychological and behavioral problems (Trani & Bakhshi, 2008; Varsamis & Agaliotis, 2015), and reduced self-esteem and interpersonal relationships (Salehi et al., 2015). Due to their impairments, students with physical/mobility disabilities are less capable to empathy with others (Ahmad, Ishfaq, & Naeem, 2013), are less likely to be accepted by their peers (Estévez, Emler, Cava, & Inglés, 2014), and have less access to social support, compared to their healthy peers (Mithen, Aitken, Ziersch, & Kavanagh, 2015). Besides, during adolescence, feeling different from others, due to having a chronic illness or disability, may negatively affect social performance and adjustment (Hsiao, Tseng, Huang, & Gau, 2013).
Adjustment is defined as the ability to adapt, compromise, collaborate, and cope with oneself, the environment, and others. In other words, adjustment refers to a set of cognitive and behavioral strategies used to cope with stressful situations. Social adjustment, as a criterion of mental health (Rahmati, Adibrad, Tahmasian & Tahmasian, 2010), refers to the adjustment of individuals to their social environment (Nader-Grosbois, Houssa, & Mazzone, 2013). Furthermore, it enables them to perceive and predict other’s behaviors, control their behaviors, and adjust their social interactions (Baurain, Nader-Grosbois, & Dionne, 2013). Overall, social adjustment is based on the necessity that an individual’s needs and desires have to be adjusted to those of the group they live in (Rahmati et al., 2010). Social adjustment is especially necessary during adolescence, i.e. due to increased interaction with peers and reduced dependence on parents (Fiasse & Nader-Grosbois, 2012). Besides, proper social adjustment during adolescence is the basis of excellent social performance, facilitates social roles, and improves life satisfaction (Baurain et al., 2013). Social maladjustment not only leads to problems in the domains mentioned above, but also may result in impaired social interactions, a tendency toward socially and morally deviant behaviors, and the deterioration of cultural values of individuals (Rahmati et al., 2010). Emotional adjustment is defined as good mental health, personal life satisfaction, and the coordination of emotions, activities, and thoughts. In other words, emotional adjustment reflects the mechanisms by which one becomes emotionally stable. Social and emotional competencies are the determinants of affecting academic adjustment.
Various definitions have been suggested for emotion regulation; however, different theories agree that emotion regulation includes skills related to emotional awareness, evaluating emotions, modulating emotions, and the adaptive use of emotions (Berking et al., 2008). Emotion regulation could also refer to emotion management through which people can influence their emotions, and determine what, when, and how they are experienced and expressed by them (Gross & Jazaieri, 2014). Emotion management is aimed at adjusting emotional responses using some techniques and strategies (Halperin, 2013). Emotion regulation strategies are defined as actions representing manners of coping with stressful situations or unpleasant events (Garnefski & Kraaij, 2006). Research on emotion regulation d that those who are unable to properly manage their emotions demonstrate more internalizing disorders (Mennin, Holaway, Fresco, Moore, & Heimberg, 2007). In addition, there is a positive and significant relationship between reappraisal, as an emotion regulation strategy, and successful performance in social interactions (Tull, Stipelman, Salters-Pedneault, & Gratz, 2009).
Emotions are essential in mental health and thriving social life performance (Gross & Jazaieri, 2014). Furthermore, it is associated with most mental and emotional disorders, including depression, anxiety, and interpersonal sensitivity (Kingston, Chadwick, Meron, & Skinner, 2007). Moreover, social adjustment significantly affects students’ mental health (Rahmati et al., 2010). Thus, the present study examined social adjustment and the use of emotion regulation strategies among students with a physical disability and healthy students.
2. methods
This was a causal-comparative study. The statistical population included all students with a physical disability and healthy middle- and high-school students of Tehran City, Iran (2016 academic year). The study sample consisted of 200 students (100 students with physical disabilities and 100 healthy students). The sample size was selected based on the limited number of students with physical disabilities in Tehran. Accordingly, 2, 4, and 16 regions (where special schools for students with physical disabilities are located) were purposefully selected. Then, by referring to the mentioned schools, the research questionnaires were presented; the research purpose and data confidentiality were explained to the students. In total, 100 students with physical disabilities completed the questionnaires; therefore, 100 healthy students were randomly selected. The study students were matched on educational level (middle- and high-school). Besides, prior similar studies that have been conducted on people with disabilities in Iran have selected a sample size of between 50 and 100 subjects.
To conduct this research, after receiving the necessary permissions from the research unit of Allameh Tabatabai University, we referred to the Ministry of Education in Tehran. Out of the 22 regions in Tehran, with a purposive sampling method, regions two, 4, and 16 that have schools for students with physical disabilities were selected as research regions. In the areas mentioned above, schools for students with physical disabilities were selected as samples. In addition, in the same areas, a sample of healthy students from regular schools was also selected for data comparison.
The inclusion criteria included students with a physical disability; having average IQ (IQ range: 90-110, based on the school counseling records); no history of psychiatric hospitalization (based on the subjects’ reports); willingness to participate in the study (via an interview in which they were marked); and no concomitant treatment. The exclusion criterion was the reluctance to continue participating in the research.
To observe the ethical considerations, the following points were met: a written informed consent form was obtained from the study participants before the study onset; the study participants were initially informed about the subject and method of the study, and participation in the study imposed no financial burden on the study subjects. The below tools were used to collect the required data:
Emotion Regulation Questionnaire (ERQ)
This 10-item questionnaire was developed by Gross and John (Gross & John, 2003). It has 2 subscales, including emotional suppression and emotional reappraisal. Among the 10 items of the ERQ, 4 items assess emotional suppression, and 6 items assess emotional reappraisal. The items are rated on a Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Total obtainable scores range from 10 to 70. Gross and John (2003), reported test-retest reliability estimates of .84 and .67 for the reappraisal and suppression subscales, respectively. In the present study, Cronbach’s alphas coefficients of 0.73 and 0.61 were obtained for the reappraisal and suppression subscales, respectively. In Iran, the Cronbach’s alpha coefficients for re-evaluation and repression were calculated as 0.83 and 0.79, respectively (Babapour & Ahmadi, 2013).
Adjustment Inventory for School Students (AISS)
This inventory was developed by Sinha and Singh (1993) to differentiate high school-students with proper adjustments from those with reduced adjustments on three adjustment domains (emotional, social, and academic). It has 60 items and 3 subscales (social adjustment, emotional adjustment, and academic adjustment). AISS items that indicate poor adjustment are scored zero, and otherwise 1. The AISS was conducted in a sample comprised of 1950 randomly-selected high-school students in grades 1, 2, and 3 (1200 boys and 750 girls); the achieved results indicated no significant difference with the normal distribution. Additionally, using split-half, test-retest, and Kuder–Richardson methods, reliability estimates of .95, .93, and .94 were found for this inventory. In the present study, a Cronbach’s alpha coefficient of 0.79 was calculated for the AISS (Sinha & Singh, 2005). furthermore, Zahed, Rajabi, & Omidi (2012) reported the Cronbach’s and Kuder-Richardson coefficients of 0.82 and 0.89 for this questionnaire, respectively.
3. Results
SPSS was used to analyze the collected data. Mean±SD values were calculated for each group (physically-disabled and healthy students) (Table 1). The correlation matrix between the research variables was calculated as well (Table 2). Then, using Multivariate Analysis of Variance (MANOVA), the two groups were compared (Tables 3 & 4).
Disability, as an impairment, limits an individual’s one or more major life activities (Brown & Turner, 2012). Moreover, it is often accompanied by reduced self-esteem (Nosek, Hughes, Swedlund, Taylor, & Swank, 2003; Salehi, Tavakol, Shabani, & Ziaei, 2015), psychological distress (Trani & Bakhshi, 2008).Disability has been used by the World Health Organization (WHO) in the International Classification of Functioning, Disability and Health (ICF) as an umbrella term for impairments, functional limitations, and participation limitations (Lucas-Carrasco et al., 2011). It is resulted in physical impairments (Aurora, 2014) and deprived independent participation in personal and social activities (Salehi et al., 2015). Physical disability, as part of a broad range of disabilities, involves failure to use one limb or part of it for at least 6 months (Bahrampour, Ghamari, & Amiri Majd, 2014). According to the WHO, nearly 1 billion people throughout the world have some disability (World Health Organization 2011). Additionally, more than one-third of them live in developing countries (Bahrampour et al., 2014).
Disability in every life aspect leads to the impaired natural and harmonious development of the person (Aurora, 2014), psychological and behavioral problems (Trani & Bakhshi, 2008; Varsamis & Agaliotis, 2015), and reduced self-esteem and interpersonal relationships (Salehi et al., 2015). Due to their impairments, students with physical/mobility disabilities are less capable to empathy with others (Ahmad, Ishfaq, & Naeem, 2013), are less likely to be accepted by their peers (Estévez, Emler, Cava, & Inglés, 2014), and have less access to social support, compared to their healthy peers (Mithen, Aitken, Ziersch, & Kavanagh, 2015). Besides, during adolescence, feeling different from others, due to having a chronic illness or disability, may negatively affect social performance and adjustment (Hsiao, Tseng, Huang, & Gau, 2013).
Adjustment is defined as the ability to adapt, compromise, collaborate, and cope with oneself, the environment, and others. In other words, adjustment refers to a set of cognitive and behavioral strategies used to cope with stressful situations. Social adjustment, as a criterion of mental health (Rahmati, Adibrad, Tahmasian & Tahmasian, 2010), refers to the adjustment of individuals to their social environment (Nader-Grosbois, Houssa, & Mazzone, 2013). Furthermore, it enables them to perceive and predict other’s behaviors, control their behaviors, and adjust their social interactions (Baurain, Nader-Grosbois, & Dionne, 2013). Overall, social adjustment is based on the necessity that an individual’s needs and desires have to be adjusted to those of the group they live in (Rahmati et al., 2010). Social adjustment is especially necessary during adolescence, i.e. due to increased interaction with peers and reduced dependence on parents (Fiasse & Nader-Grosbois, 2012). Besides, proper social adjustment during adolescence is the basis of excellent social performance, facilitates social roles, and improves life satisfaction (Baurain et al., 2013). Social maladjustment not only leads to problems in the domains mentioned above, but also may result in impaired social interactions, a tendency toward socially and morally deviant behaviors, and the deterioration of cultural values of individuals (Rahmati et al., 2010). Emotional adjustment is defined as good mental health, personal life satisfaction, and the coordination of emotions, activities, and thoughts. In other words, emotional adjustment reflects the mechanisms by which one becomes emotionally stable. Social and emotional competencies are the determinants of affecting academic adjustment.
Various definitions have been suggested for emotion regulation; however, different theories agree that emotion regulation includes skills related to emotional awareness, evaluating emotions, modulating emotions, and the adaptive use of emotions (Berking et al., 2008). Emotion regulation could also refer to emotion management through which people can influence their emotions, and determine what, when, and how they are experienced and expressed by them (Gross & Jazaieri, 2014). Emotion management is aimed at adjusting emotional responses using some techniques and strategies (Halperin, 2013). Emotion regulation strategies are defined as actions representing manners of coping with stressful situations or unpleasant events (Garnefski & Kraaij, 2006). Research on emotion regulation d that those who are unable to properly manage their emotions demonstrate more internalizing disorders (Mennin, Holaway, Fresco, Moore, & Heimberg, 2007). In addition, there is a positive and significant relationship between reappraisal, as an emotion regulation strategy, and successful performance in social interactions (Tull, Stipelman, Salters-Pedneault, & Gratz, 2009).
Emotions are essential in mental health and thriving social life performance (Gross & Jazaieri, 2014). Furthermore, it is associated with most mental and emotional disorders, including depression, anxiety, and interpersonal sensitivity (Kingston, Chadwick, Meron, & Skinner, 2007). Moreover, social adjustment significantly affects students’ mental health (Rahmati et al., 2010). Thus, the present study examined social adjustment and the use of emotion regulation strategies among students with a physical disability and healthy students.
2. methods
This was a causal-comparative study. The statistical population included all students with a physical disability and healthy middle- and high-school students of Tehran City, Iran (2016 academic year). The study sample consisted of 200 students (100 students with physical disabilities and 100 healthy students). The sample size was selected based on the limited number of students with physical disabilities in Tehran. Accordingly, 2, 4, and 16 regions (where special schools for students with physical disabilities are located) were purposefully selected. Then, by referring to the mentioned schools, the research questionnaires were presented; the research purpose and data confidentiality were explained to the students. In total, 100 students with physical disabilities completed the questionnaires; therefore, 100 healthy students were randomly selected. The study students were matched on educational level (middle- and high-school). Besides, prior similar studies that have been conducted on people with disabilities in Iran have selected a sample size of between 50 and 100 subjects.
To conduct this research, after receiving the necessary permissions from the research unit of Allameh Tabatabai University, we referred to the Ministry of Education in Tehran. Out of the 22 regions in Tehran, with a purposive sampling method, regions two, 4, and 16 that have schools for students with physical disabilities were selected as research regions. In the areas mentioned above, schools for students with physical disabilities were selected as samples. In addition, in the same areas, a sample of healthy students from regular schools was also selected for data comparison.
The inclusion criteria included students with a physical disability; having average IQ (IQ range: 90-110, based on the school counseling records); no history of psychiatric hospitalization (based on the subjects’ reports); willingness to participate in the study (via an interview in which they were marked); and no concomitant treatment. The exclusion criterion was the reluctance to continue participating in the research.
To observe the ethical considerations, the following points were met: a written informed consent form was obtained from the study participants before the study onset; the study participants were initially informed about the subject and method of the study, and participation in the study imposed no financial burden on the study subjects. The below tools were used to collect the required data:
Emotion Regulation Questionnaire (ERQ)
This 10-item questionnaire was developed by Gross and John (Gross & John, 2003). It has 2 subscales, including emotional suppression and emotional reappraisal. Among the 10 items of the ERQ, 4 items assess emotional suppression, and 6 items assess emotional reappraisal. The items are rated on a Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Total obtainable scores range from 10 to 70. Gross and John (2003), reported test-retest reliability estimates of .84 and .67 for the reappraisal and suppression subscales, respectively. In the present study, Cronbach’s alphas coefficients of 0.73 and 0.61 were obtained for the reappraisal and suppression subscales, respectively. In Iran, the Cronbach’s alpha coefficients for re-evaluation and repression were calculated as 0.83 and 0.79, respectively (Babapour & Ahmadi, 2013).
Adjustment Inventory for School Students (AISS)
This inventory was developed by Sinha and Singh (1993) to differentiate high school-students with proper adjustments from those with reduced adjustments on three adjustment domains (emotional, social, and academic). It has 60 items and 3 subscales (social adjustment, emotional adjustment, and academic adjustment). AISS items that indicate poor adjustment are scored zero, and otherwise 1. The AISS was conducted in a sample comprised of 1950 randomly-selected high-school students in grades 1, 2, and 3 (1200 boys and 750 girls); the achieved results indicated no significant difference with the normal distribution. Additionally, using split-half, test-retest, and Kuder–Richardson methods, reliability estimates of .95, .93, and .94 were found for this inventory. In the present study, a Cronbach’s alpha coefficient of 0.79 was calculated for the AISS (Sinha & Singh, 2005). furthermore, Zahed, Rajabi, & Omidi (2012) reported the Cronbach’s and Kuder-Richardson coefficients of 0.82 and 0.89 for this questionnaire, respectively.
3. Results
SPSS was used to analyze the collected data. Mean±SD values were calculated for each group (physically-disabled and healthy students) (Table 1). The correlation matrix between the research variables was calculated as well (Table 2). Then, using Multivariate Analysis of Variance (MANOVA), the two groups were compared (Tables 3 & 4).
Both groups were matched according to their educational level, similarly, and demographic characteristics. The number of middle-school students in both groups was 38. The mean age of the group with disabilities was 13.61 years, and in the healthy group, it was 13.20 years. Furthermore, the number of high-school students in both was 62; the mean age of the group with disabilities was 16.49 years and it was 15.89 years in the healthy group.
To analyze the acquired data, Pearson’s correlation analysis and MANCOVA were applied. Before using MANCOVA, to comply with its assumptions was used Levene’s test and Box test; the condition of homogeneity of variance matrices of variance/covariance was respected. These test results were not significant for any of the variables. As a result of the use of parametric tests was allowed. Significance levels of all tests allowed the use of MANCOVA.
The descriptive analysis results of the study groups (mean±SD) are presented in Table 1.
As per Table 2, re-evaluation, as a subscale of emotion regulation strategies, had a positive and significant relationship with adaptation in three educational, social, and emotional areas. Moreover, repression, as another subscale of emotion regulation strategies, had a negative relationship with adjustment in different educational, social, and emotional aspects.
According to Table 3, the effect of the group on the linear combination of dependent variables was significant. Thus, it indicates that the two study groups were significantly different in a combination of dependent variables (repression, re-evaluation, and adjustment) in Pillai’s trace, Wilks’ Lambda, Hotelling’s Trace, and Roy’s Largest Root with the estimates of an effect size equal to 0.93.
According to Table 4, for each dependent variable, data analysis (using Bonferroni alpha of 0.017 and the degrees of freedom 1, 198) suggested that education, as a dimension of adjustment was not significantly different between the two groups.
4. Discussion
The present study examined social adjustment and the use of emotion regulation strategies among students with physical/mobility disabilities and healthy students. According to the study findings, there was a positive and significant relationship between social adjustment and reappraisal (r=0.72) and a significant negative relationship between suppression and social adjustment (r=-0.65); these findings indicated that emotional reappraisal, as an emotion regulation strategy, improved social adjustment; however, emotional suppression decreased social adjustment. There was also a significant difference between the two groups regarding the use of emotion regulation strategies (suppression and reappraisal); these findings indicate that compared to healthy students, those with physical/mobility disabilities were less capable of managing or regulating their emotional responses and coping with stressful or unpleasant life events. There was no previous study precisely similar to the present one. However, Garnefski and Kraaij argued that emotion regulation strategies were associated with psychological distress and significantly predicted subsequent adjustment (Garnefski & Kraaij, 2006). Mennin et al. (2007) also reported that those who were not able to efficiently manage their emotions against daily life events indicated more diagnostic symptoms of internalizing disorders, like depression and anxiety.
This population has emotional problems, mental health issues, misinterpretations, focus on the negative aspects of life, and feel the lack of control over the internal and external world (which may be related to their developmental impairments). Thus, students with physical/mobility disabilities tend to use negative emotion regulation strategies in the face of stressful or unpleasant events; in contrast, healthy students, in such events, tend to use adaptive emotion regulation strategies, such as making positive reappraisals, considering adverse events as unimportant or less unpleasant than other events, and having a feeling of control over the internal and external world. Therefore, the second group is less vulnerable to emotional problems. This suggests that students less capable of managing their emotions in the face of daily life events, experience more psychological distress. Such distress may lead to depression and anxiety; contrarily, effective emotion regulation is related to healthier relationships, better academic performance, and better physical health.
Another study indicated a significant difference between the scores of students with physical/mobility disabilities and healthy students in two subscales of social adjustment; the emotional and social adjustment subscales. However, no significant difference was found between the two groups in the academic adjustment subscale. This finding is in line with those of Sharma (Sharma, 2004), wiener (Wiener, 2004), Sideritis (Sideridis, 2007; Auerbach, Gross-Tsur, Manor, & Shalev, 2008; Freilich & Shechtman, 2010), indicating that disabled children and adolescents have higher rates of social and emotional problems, compared to their healthy counterparts.
The study finding indicating decreased social adjustment in students with physical/mobility disabilities could be explained by the fact that, like physical development, social development is a continuous process; i.e. it is gradually achieved during different life stages through g various experiences. Furthermore, it is among the most important signs of desirable mental health status in adolescents. In other words, an individual is considered to have reasonable adjustment only when being able to have a healthy relationship with their social environment; otherwise, a proper adjustment cannot be achieved by the person. However, research indicates that, due to facing numerous problems in life as well as poor interpersonal skills, adolescents with disabilities often have poor mental health (Sideridis, 2007), experience higher social rejection and loneliness (Estell et al., 2008), and are less popular than their healthy peers. Additionally, because of their developmental problems, students with physical/mobility disabilities tend to develop impairments in their performance and adjustment. This matter results from experiences, such as their peers’ success, love failure, and losing motivation for life. When adolescents are unable to successfully overcome developmental challenges, they experience psychological distress and considerable impairments in the emotional and social aspects of their lives. In addition, students with physical/mobility disabilities perceive themselves as different from others and tend to evaluate their appearance negatively. Therefore, they are more prone to experience social problems and ignorance by others; as a result, they may demonstrate a poor adjustment.
It the present study, no significant difference was observed in academic adjustment between the study groups. No previous finding consistent with this result was detected; however, in contrast to this finding, in a study by Zahed, Rajabi, & Omidi (2012) on social, emotional, academic, and self-regulating learning, a significant difference was found between students with and without learning disabilities (“a comparison of social, emotional and educational adjustment and self-regulated learning in students with and without learning disabilities”, 2012). This finding can also be explained using the inferiority complex (Adler’s theory). Adler stated that actual mental or physical inferiority could be a source of inferiority feelings. He believed that physical impairment could affect personality and motivate individuals to overcome their impairment or disability. Compensation has a vital role in the feelings of inferiority; it is often used by those with a physical disability to cover disability and impairment, to create a new balance in the organism. Therefore, the lack of difference between physical disability and academic achievement could be attributed to the use of compensation by adolescents with disabilities to cope with their impairments and shortcomings.
The present study was only conducted on students with physical disabilities; thus, cautions should be considered in generalizing the obtained outcomes to other rehabilitation communities. Moreover, the study data were achieved based on self-report (questionnaire); therefore, the collected results may be biased. As a result, qualitative methods are suggested for better investigation of future research structures.
Future studies are suggested to examine the study variables among female students as well as students with other disabilities, such as visual and auditory impairments. Accordingly, their results can be used to improve the use of adaptive emotion regulation strategies in students with disabilities and help them achieve the optimum level of adjustment in different domains.
Compared to healthy students, their counterparts with physical/mobility disabilities are more likely to use negative emotion regulation strategies, especially suppression; however, healthy students tend to use more positive emotion regulation strategies, especially reappraisal. Therefore, students with physical disabilities benefit from lower emotional and social adjustment, compared to their healthy peers.
Ethical Considerations
Compliance with ethical guidelines
A written informed consent was obtained from the participants prior to the study. They were informed of the study objectives and methods. Participation in the study did not impose any costs on the participants.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Methodology: Dana Mohammad-aminzadeh, Yousef Asmari; Investigation: Seyed Jalal Younesi; Writing-original draft: Dana Mohammad-aminzadeh, Somaye Kazemian, Amir Abasi Writing-review & editing: Seyed Jalal Younesi, somaye Kazemian; Resources: Dana Mohammad-aminzadeh, Amir Abasi Supervision: Seyed Jalal Younesi.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
We would like to express our sincere thanks to the study participants and the schools’ personnel for their cooperation and support.
References
Ahmad, T., Ishfaq, K., & Naeem, S. B. (2013). Impact of physically disability of children on their families; a study in Children Hospital & Institute of Child Health Multan, Pakistan. International Journal of Medicine and Applied Health, 1(2), 46-51.
Auerbach, J. G., Gross-Tsur, V., Manor, O., & Shalev, R. S. (2008). Emotional and behavioral characteristics over a six-year period in youths with persistent and nonpersistent dyscalculia. Journal of Learning Disabilities, 41(3), 263-73. [DOI:10.1177/0022219408315637] [PMID]
Aurora, U. (2014). Study for determining laterality in children with motor disabilities in adapted physical activities. Procedia - Social and Behavioral Sciences, 117, 646-52. [DOI:10.1016/j.sbspro.2014.02.276]
Babapour Kheiroddin, J., & Ahmadi, E. (2013). [A comparison of emotion regulation strategies and mindfulness in students with and without obsessive believes (Persian)]. Journal of Modern Psychological Researches, 7(28), 23-40.
Baurain, C., Nader-Grosbois, N., & Dionne, C. (2013). Socio-emotional regulation in children with intellectual disability and typically developing children, and teachers’ perceptions of their social adjustment. Research in Developmental Disabilities, 34(9), 2774-87. [DOI:10.1016/j.ridd.2013.03.022] [PMID]
Berking, M., Wupperman, P., Reichardt, A., Pejic, T., Dippel, A., & Znoj, H. (2008). Emotion-regulation skills as a treatment target in psychotherapy. Behaviour Research and Therapy, 46(11), 1230-7. [DOI:10.1016/j.brat.2008.08.005] [PMID]
Brown, R. L., & Turner, R. J. (2012). Physical limitation and anger stress exposure and assessing the role of psychosocial resources. Society and Mental Health, 2(2), 69-84. [DOI:10.1177/2156869312444441]
Estell, D. B., Jones, M. H., Pearl, R., Van Acker, R., Farmer, T. W., & Rodkin, P. C. (2008). Peer groups, popularity, and social preference trajectories of social functioning among students with and without learning disabilities. Journal of Learning Disabilities, 41(1), 5-14. [DOI:10.1177/0022219407310993] [PMID]
Estévez López, E., Emler, N. P., Cava, M. J., & Inglés Saura, C. J. (2014). Psychosocial adjustment in aggressive popular and aggressive rejected adolescents at school. Psychosocial Intervention, 23(1), 57-67. [DOI:10.5093/in2014a6]
Fiasse, C., & Nader-Grosbois, N. (2012). Perceived social acceptance, theory of mind and social adjustment in children with intellectual disabilities. Research in Developmental Disabilities, 33(6), 1871-80. [DOI:10.1016/j.ridd.2012.05.017] [PMID]
Freilich, R., & Shechtman, Z. (2010). The contribution of art therapy to the social, emotional, and academic adjustment of children with learning disabilities. The Arts in Psychotherapy, 37(2), 97-105. [DOI:10.1016/j.aip.2010.02.003]
Garnefski, N., & Kraaij, V. (2006). Cognitive Emotion Regulation Questionnaire-development of a short 18-item version (CERQ-short). Personality and Individual Differences, 41(6), 1045-53. [DOI:10.1016/j.paid.2006.04.010]
Gross, J. J., & Jazaieri, H. (2014). Emotion, emotion regulation, and psychopathology an affective science perspective. Clinical Psychological Science, 2(4), 387-401. [DOI:10.1177/2167702614536164]
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348-62. [DOI:10.1037/0022-3514.85.2.348] [PMID]
Halperin, E. (2014). Emotion, emotion regulation, and conflict resolution. Emotion Review, 6(1), 68-76. [DOI:10.1177/1754073913491844]
Hsiao, M. N., Tseng, W. L., Huang, H. Y., & Gau, S. S. (2013). Effects of autistic traits on social and school adjustment in children and adolescents: The moderating roles of age and gender. Research in Developmental Disabilities, 34(1), 254-65. [DOI:10.1016/j.ridd.2012.08.001] [PMID]
Kingston, J., Chadwick, P., Meron, D., & Skinner, T. C. (2007). A pilot randomized control trial investigating the effect of mindfulness practice on pain tolerance, psychological well-being, and physiological activity. Journal of Psychosomatic Research, 62(3), 297-300. [DOI:10.1016/j.jpsychores.2006.10.007] [PMID]
Lucas-Carrasco, R., Eser, E., Hao, Y., McPherson, K. M., Green, A., Kullmann, L., & WHOQOL-DIS Group. (2011). The Quality of Care and Support (QOCS) for people with disability scale: Development and psychometric properties. Research in Developmental Disabilities, 32(3), 1212-25. [DOI:10.1016/j.ridd.2010.12.030] [PMID]
Mennin, D. S., Holaway, R. M., Fresco, D. M., Moore, M. T., & Heimberg, R. G. (2007). Delineating components of emotion and its dysregulation in anxiety and mood psychopathology. Behavior Therapy, 38(3), 284-302. [DOI:10.1016/j.beth.2006.09.001] [PMID]
Mithen, J., Aitken, Z., Ziersch, A., & Kavanagh, A. M. (2015). Inequalities in social capital and health between people with and without disabilities. Social Science & Medicine, 126, 26-35. [DOI:10.1016/j.socscimed.2014.12.009] [PMID]
Nader-Grosbois, N., Houssa, M., & Mazzone, S. (2013). How could theory of mind contribute to the differentiation of social adjustment profiles of children with externalizing behavior disorders and children with intellectual disabilities? Research in Developmental Disabilities, 34(9), 2642-60. [DOI:10.1016/j.ridd.2013.05.010] [PMID]
Nosek, M. A., Hughes, R. B., Swedlund, N., Taylor, H. B., & Swank, P. (2003). Self-esteem and women with disabilities. Social Science & Medicine, 56(8), 1737-47. [DOI:10.1016/S0277-9536(02)00169-7]
Rahmati, B., Adibrad, N., & Tahmasian, K., & Saleh Sedghpour, B. (2010). The effectiveness of life skill training on social adjustment in children. Procedia - Social and Behavioral Sciences, 5, 870-4. [DOI:10.1016/j.sbspro.2010.07.201]
Salehi, M., Kharaz Tavakol, H., Shabani, M., & Ziaei, T. (2015). The relationship between self-esteem and sexual self-concept in people with physical-motor disabilities. Iranian Red Crescent Medical Journal, 17(1), e25359. [DOI:10.5812/ircmj.25359] [PMID] [PMCID]
Sharma, G. (2004). A comparative study of the personality characteristics of primary-school students with learning disabilities and their nonlearning disabled peers. Learning Disability Quarterly, 27(3), 127-40. [DOI:10.2307/1593664]
Sideridis, G. D. (2007). International approaches to learning disabilities: More alike or more different? Learning Disabilities Research & Practice, 22(3), 210-5. [DOI:10.1111/j.1540-5826.2007.00249.x]
Sinha, A., & Singh, R. (2005). Manual for adjustment inventory for school students. Agra: National psychological corporation.
Trani, J. F., & Bakhshi, P. (2008). Challenges for assessing disability prevalence: The case of Afghanistan. Alter, 2(1), 44-64. [DOI:10.1016/j.alter.2007.10.003]
Tull, M. T., Stipelman, B. A., Salters-Pedneault, K., & Gratz, K. L. (2009). An examination of recent non-clinical panic attacks, panic disorder, anxiety sensitivity, and emotion regulation difficulties in the prediction of generalized anxiety disorder in an analogue sample. Journal of Anxiety Disorders, 23(2), 275-82. [DOI:10.1016/j.janxdis.2008.08.002] [PMID]
Varsamis, P., & Agaliotis, I. (2015). Relationships between gross- and fine motor functions, cognitive abilities, and self-regulatory aspects of students with physical disabilities. Research in Developmental Disabilities, 47, 430-40. [DOI:10.1016/j.ridd.2015.10.009] [PMID]
Wiener, J. (2004). Do peer relationships foster behavioral adjustment in children with learning disabilities? Learning Disability Quarterly, 27(1), 21-30. [DOI:10.2307/1593629]
World Health Organization. (2011). World report on disability. Geneva: World Health Organization.
Zahed, A., Rajabi, S., & Omidi, M. (2012). [A comparison of social, emotional and educational adjustment and self-regulated learning in students with and without learning disabilities (Persian)]. Journal of Learning Disabilities, 1(2), 43-62.
Type of Study: Research |
Subject:
Rehabilitation
Received: 2019/01/10 | Accepted: 2019/07/7 | Published: 2019/10/1
Received: 2019/01/10 | Accepted: 2019/07/7 | Published: 2019/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
