

Volume 12, Issue 4 (Autumn 2024)
PCP 2024, 12(4): 323-334 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zanganeh Gheshlaghi M, Salehi M, Jafari Roshan M. The Mediating Role of Health Anxiety in Explaining Personality Dimensions and Death Anxiety in the Elderly. PCP 2024; 12 (4) :323-334
URL: http://jpcp.uswr.ac.ir/article-1-955-en.html
URL: http://jpcp.uswr.ac.ir/article-1-955-en.html



1- Department of Psychology, Faculty of Psychology and Social Sciences, Central Tehran Branch, Islamic Azad University, Tehran, Iran.
2- Department of Clinical Health Psychology, Faculty of Psychology and Social Sciences, Central Tehran Branch, Islamic Azad University, Tehran, Iran. ,mah.salehi@iauctb.ac.ir
2- Department of Clinical Health Psychology, Faculty of Psychology and Social Sciences, Central Tehran Branch, Islamic Azad University, Tehran, Iran. ,
Full-Text [PDF 705 kb]
(976 Downloads)
| Abstract (HTML) (2584 Views)
Full-Text: (791 Views)
Introduction
he elderly is one of the most challenging stages of life and a complex set of physical, psychological, and social changes that elderly people face and it is considered a heavy burden for their psychosocial functioning and mental health (Bahar et al., 2022). One of the common psychological problems in old age is anxiety because this period is full of all kinds of feelings of deficiencies and inabilities. Studies show that the elderly are exposed to more anxiety due to reduced self-confidence, lack of activity and movement, loss of friends and relatives, reduced material and physical independence, and chronic diseases. Perhaps the most common anxiety is death anxiety (DA) (Jangi Jahantigh et al., 2022).
Health anxiety (HA) can also be more common in this age group due to the physical vulnerability of the elderly and their awareness of this issue (Safari et al., 2022). HA is a psychological experience characterized by a perceived threat to one’s health that produces physical and emotional symptoms of anxiety. In experiencing HA, a person perceives feelings and physical changes as symptoms of illness. Although normal levels of HA have a protective effect and lead to beneficial health and health-related behaviors, high levels of anxiety are problematic and harmful to mental health (Safari et al., 2022). Anxiety plays a role in reducing physical health, life satisfaction, and quality of life (QoL) of the elderly. Elderly people who experience symptoms of anxiety are more likely to show impairments in different areas of cognitive functioning compared to the elderly who have less anxiety (Majdara et al., 2015). HA or self-diagnosis is common but understudies due to the spread of negative life experiences, including problems and diseases caused by aging and the death of family and relatives (El-Gabalawy et al., 2013). HA is an individual’s mental preoccupation with false beliefs or a serious, dangerous disease growing and it is a disorder that puts a significant burden on health services (Axelsson & Hedman-Lagerlöf, 2022). Thielsch et al. (2015) have proposed the metacognition and intolerance of uncertainty and worry. According to the metacognitive model, anxiety continues until the person recognizes that they can effectively deal with the anticipated danger, but uncertainty about their health and longevity in the elderly increases anxiety and related cognitive and physical symptoms (Davey & Wells, 2008).
Glasser (2019) emphasizes the choice theory on the personality dimensions (PDs), conscientiousness, and responsibility in the individual to achieve the meaning of life. A person should identify the behavior that he/she is trying to correct, pay all his/her attention to it, and not make any excuses to deny his/her responsibility. A conscientious person can make better choices by re-evaluating his/her desires and behaviors to achieve satisfaction from life, and ultimately achieve a more flexible, meaningful, and enjoyable life. Ashton et al. (2014) proposed HEXACO PDs. This model assumes that PDs can be summarized in six dimensions, honesty-humility, emotionality, extraversion, agreeableness, conscientiousness, and openness to experience (Lee & Ashton, 2018). Based on Glaser’s choice theory, since humans can make conscious choices, exercise their will, and consider the future, therefore, according to this view, every elderly person is responsible for their health, and it seems that HEXACO conscientiousness should be involved in this matter (Glasser, 2019). In this regard, in the study of Gonzatti et al., the elderly obtained the highest scores in the dimension of conscientiousness and responsibility compared to other age groups (Gonzatti et al., 2018).
Based on what has been said, the current research aims to answer this question: Does a causal model of DA in the elderly who lived in nursing homes based on PDs with the mediation of HA and the moderating role of gender fit the collected data?
Materials and Methods
The present research was conducted by correlation method and using path analysis. The statistical population of the research included all the elderly who lived in private nursing homes in Tehran City in the summer and autumn of 2023, of which, 340 people were selected by the convenience sampling method. In the current research, the method of “ the number of cases (N) to the number of estimated parameters (q), N:q” was used to determine the sample size. Based on the N:q rule, the sample-size-to-parameters ratio of 5:1 results in a small sample size, a ratio of 10:1 is a suitable sample size, and a ratio of 20:1 is an optimal sample size (Myers et al., 2016). Based on this method, in the present study, the sample size was determined to be 10 times the number of available parameters (21 parameters) and equal to 340 people.
Inclusion and exclusion criteria
The inclusion criteria included 65 to 75 years old, reading and writing education, not being abandoned, not being unsupervised or poorly supervised, and being a widow. The exclusion criteria included simultaneous use of psychiatric drugs and receiving psychotherapy interventions, suffering from acute chronic physical diseases including acute diabetes, high blood pressure, and serious cardiovascular diseases.
Procedures
Templer DA scale (DAS)
Templer DAS (1970) includes 15 items that measure an individual’s attitudes toward death-related topics. Subjects specify their answers to each question with yes or no options. The scores of this scale range from 0 and 15, where a high score indicates an intense fear of death (Thanatophobia) (Templer, 1970). The studies conducted on the validity and reliability of the DAS scale show that this scale has acceptable validity. In the origin section, the test re-test reliability (i.e. intraclass correlation) of the DAS scale is 0.83 and its concurrent validity is reported based on the correlation with the overt anxiety scale of 0.27 and the depression scale of 0.4. Rajabi and Naderi Nobandegani (2020) investigated the reliability and validity of the DAS scale in Iran and reported the internal consistency coefficient as 0.73 and the correlation of the DAS scale with the overt anxiety scale as 0.34 as an index of convergent validity of the instrument.
Short HA inventory (SHAI)
The SHAI (Salkovskis et al., 2002), includes 18 items that are scored on a 4-point Likert scale from 0 to 3. The minimum and maximum score of SHAI is equal to 0 and 54, respectively. A higher score in this tool means a higher level of HA. In the research of Salkovskis et al., (2002) Cronbach’s α coefficient for this tool was reported as 0.89. Nargesi et al. (2017) reported the correlation of this tool with the “Ahvaz self-diagnosis test”=0.75 and Cronbach’s α coefficient for this tool=0.87.
The HEXACO personality inventory
The HEXACO personality inventory-revised (HEXACO-PI-R) (Lee & Ashton, 2018) contains 100 items that measure 6 PDs, including honesty-humility, emotionality, extraversion, agreeableness, conscientiousness, and openness to experience in a 5-point Likert scale from completely disagree=1 to completely agree=5. Karimi and Minaei (2016) obtained Cronbach’s α coefficients in the range of 0.74 to 0.62 for this instrument. They reported the correlation of this tool with the NEO personality inventory-revised as an index of convergent validity of the tool.
Results
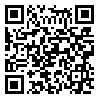
A total of 340 elderly people (185 women and 155 men) participated in the present study with the Mean±SD age of age group for women and men equal to 66.24 and 3.19, respectively. Table 1 presents the Mean±SD of PDs (honesty-humility, emotionality, extraversion, agreeableness, conscientiousness, and openness to experience), HA, and DA.
Univariate normal distribution
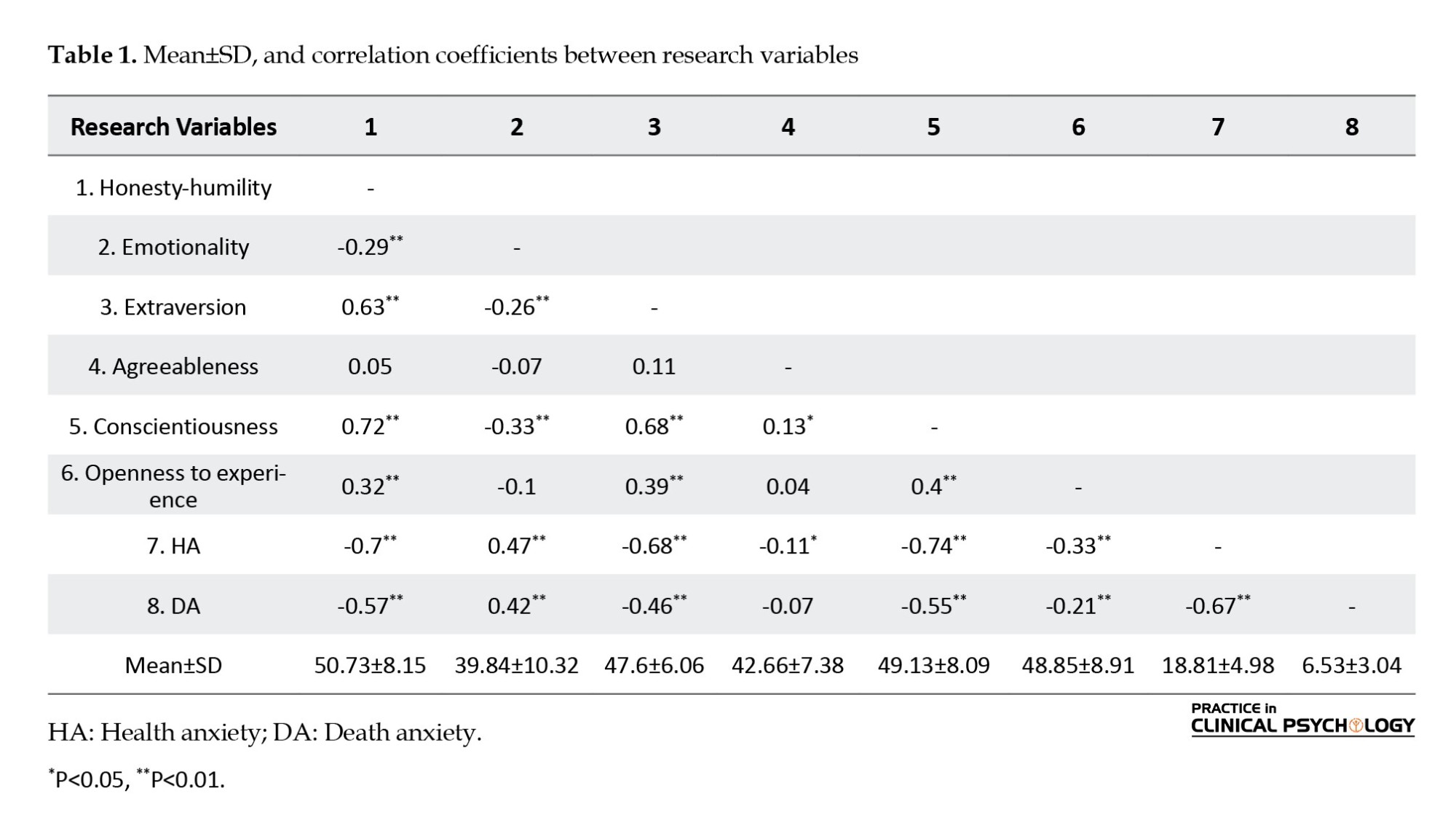
Table 1 presents the correlation coefficients between the variables, based on which, the direction of the correlation between the variables was consistent with the expectations and the theories of the research field. In this research, to evaluate the assumption of univariate normal distribution, Kurtosis, and skewness of the variables and to evaluate the assumption of collinearity of values, variance inflation factor (VIF) and tolerance coefficient were investigated. (Table 2).
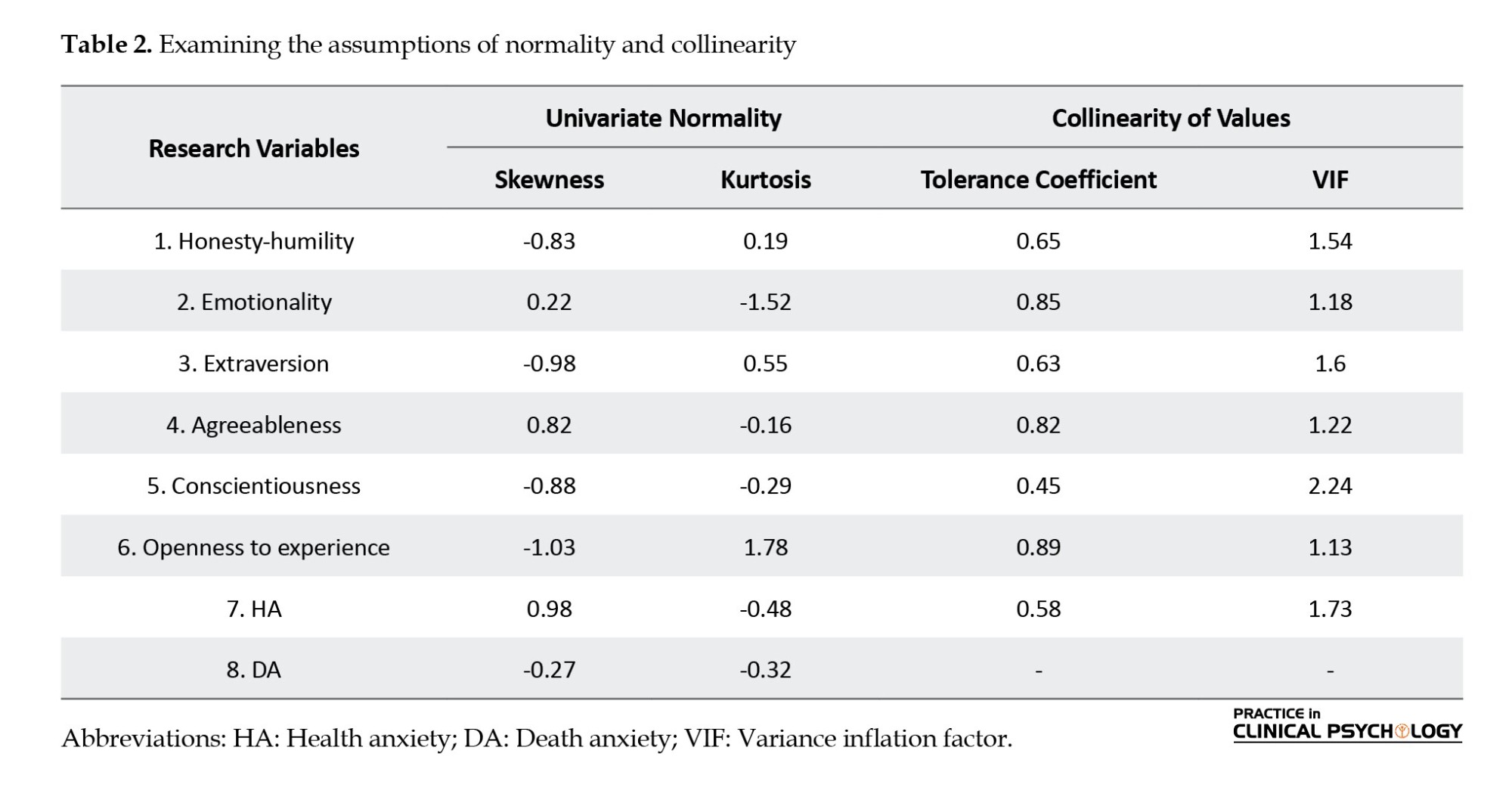
Table 2 shows that the Kurtosis and skewness values of all components are in the range of ±2. This result indicates that the assumption of univariate normal distribution among the data is valid (Kline, 2023). Also, as shown in Table 2, the assumption of collinearity was valid among the data of the current research. Because the tolerance coefficient values of predictor variables were larger than 0.1 and the VIF values of each of them were smaller than 10. According to Myers et al., (2016), the tolerance coefficient is less than 0.1 and the value of the VIF is higher than 10, indicating that the assumption of collinearity is not established.
Multivariate normal distribution (MND)
In this research, to evaluate the establishment or non-establishment of the assumption of MND, the information analysis related to “the Mahalanobis distance” was used. The values of Skewness and Kurtosis were obtained as 0.93 and 1.18, respectively. Therefore, the value of both indices was in the range of ±2, confirming the assumption of MND among the data. Finally, to evaluate the homogeneity of variances, the scatter diagram of the standardized residuals of the errors was examined and the evaluations showed that the assumption is also valid among the data.
Model specification
In the research model, it was assumed that PDs are mediated by HA and DA. In this research, the path analysis (PA) method was used to analyze the data. To do this, version 24 of AMOS software and the maximum likelihood estimation method were used.
Because 8 indicators were found in the research model, therefore its known elements were (v[v+1]/2=36), and on the other hand, the number of unknown elements was also 36, and as a result, its degrees of freedom (df) was equal to zero (0=36-36). Models in which the df is equal to zero are called just-identified. In just-identified models, the estimation parameters and fitness indices are assumed to be complete and not estimated (Weston & Gore, 2006).
The evaluation of the path coefficient (PC) in the initial model showed that the PC of none of the two factors of agreeableness and openness to experience with the two variables of HA and DA is not significant. For this reason, two factors were left out in the modification of the model. In addition, the direct PC between emotionality and DA on the one hand and the direct PC between the humility factor and DA on the other hand were not statistically significant. Therefore, these two paths were removed from the model. After modifying the model, the fit of the model was again evaluated with the collected data. Table 3 presents the fit indices of the model after modification.
Table 3 shows that after modifying the model, the fit indices obtained from the PA support the acceptable fit of the model with the compiled data. Table 4 presents the PC in the research model.
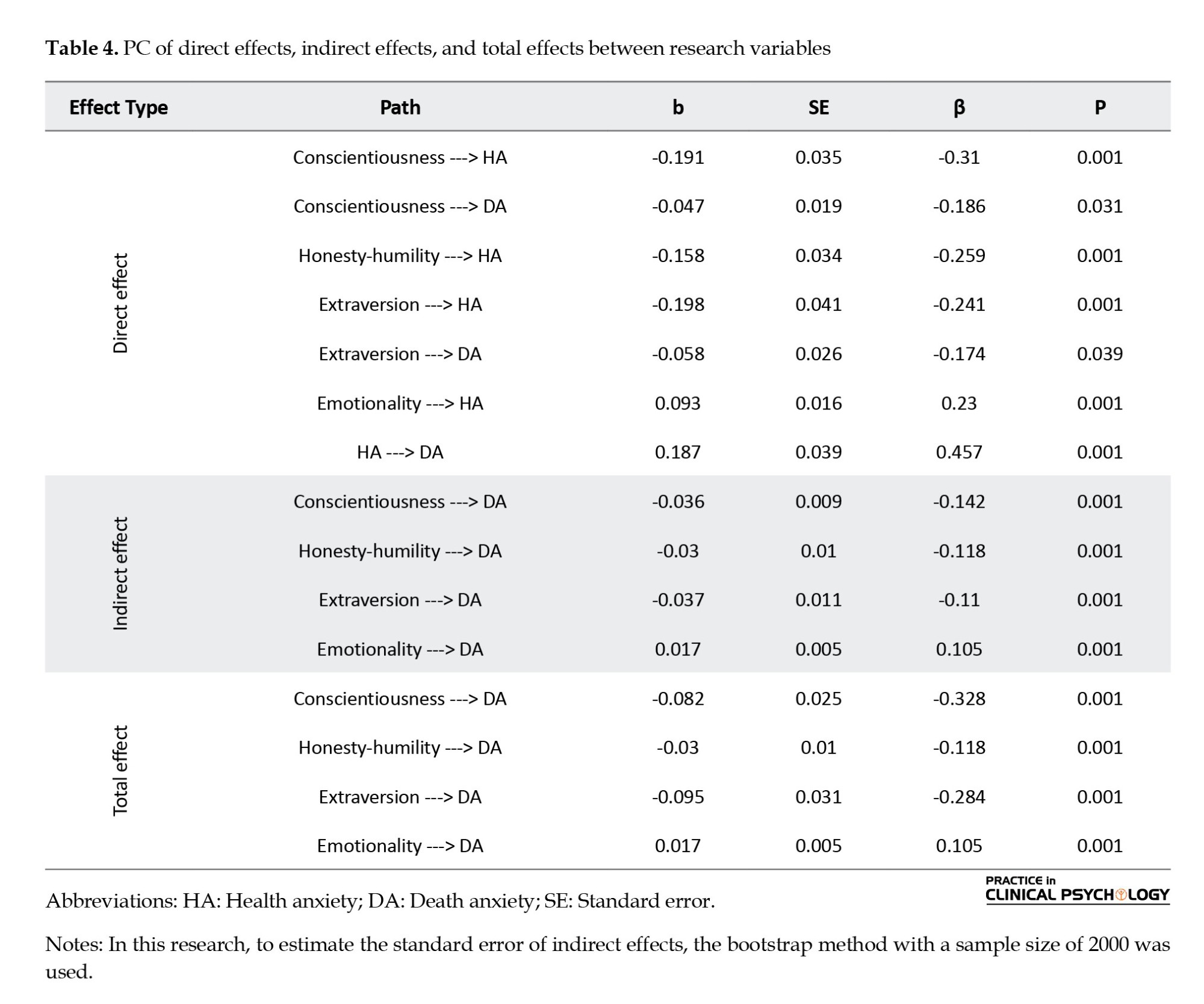
According to the model presented in Figure 1, in addition to removing the two factors of agreeableness and openness to experience, the direct PC between emotionality and DA, as well as the direct PC between the honesty factor and DA due to lack of significance, were removed during the model modification. Table 4 shows that the PC (direct and indirect PC) between PDs extraversion (β=-0.284, P=0.001) and conscientiousness (P=0.001, β=-0.328) is negative and significant with DA. Also, the PC between HA and DA (P=0.001, β=0.457) is positive and significant. The indirect PC between PD extraversion (P=0.001, β=0.110), conscientiousness (P=0.142, β=0.001) and humility (P=0.001, β118 β=-0) with DA was negative and significant. While the indirect PC between PD emotionality (P=0.001, β=0.105) and DA was positive and significant. Based on this, it can be concluded that HA among the elderly mediates the relationship between the three PDs of extroversion, humility, and conscientiousness with DA negatively and the relationship between PD emotionality and DA positively and significantly.
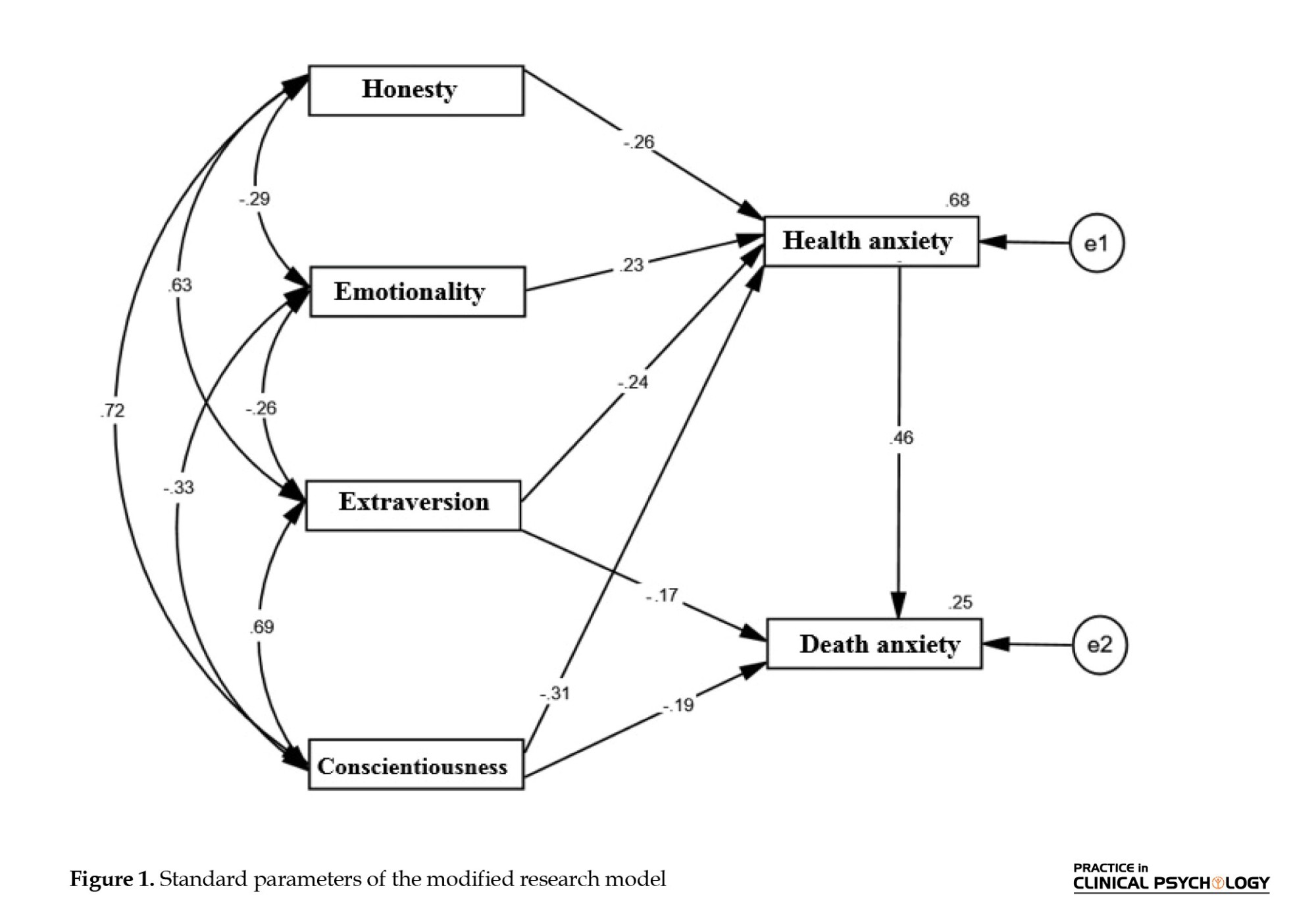
Figure 1 shows the standard parameters in the research model. As shown, the sum of squared multiple correlation (R2) for DA was equal to 0.25. This shows that the PD factors of humility, extroversion, conscientiousness, and emotionality together with HA explain 25% of the variance of DA in the elderly.
Discussion
First hypothesis: PDs are related to DA in the elderly living in nursing homes.
The results of statistical analysis showed that the PC between the PD factors of extroversion, conscientiousness, and humility with DA was negative and the PC between the PD factor of emotionality with DA was positive and significant. Therefore, in the test of the first hypothesis, it was concluded that among the PD factors, emotionality is positively related, and the PD factors of extroversion, conscientiousness, and humility are negatively and significantly related to the HA of the elderly living in nursing homes.
These results are consistent with the results of other researchers (Kardis et al., 2022; Veisi et al., 2023; Mock, 2021; Moulaei et al., 2023; Noroziyan and Peyadekoohsar, 2022; Rafezi, 2022; Tabe Bordbar et al., 2018; Khayat et al., 2018).
According to Kardis et al., (2022), a significant negative relationship is observed between extraversion and DA. While confirming the relationship between PDs and DA, Veisi et al., (2023) showed that DA plays a mediating role in the relationship between PDs and psychological well-being in people with coronavirus. Noroziyan and Peyadekoohsar, (2022) showed that neuroticism and conscientiousness have a significant positive and negative relationship with DA, respectively. According to Rafezi, (2022), a positive relationship is observed between neuroticism and DA, and a negative and significant relationship between PDs of extroversion, flexibility, and conscientiousness and DA. Tabe Bordbar et al., (2018) showed that neuroticism/negative emotionality positively and significantly, and extroversion and responsibility negatively and significantly can predict DA in the elderly. Khayat et al., (2018) observed a negative and direct relationship between agreeableness and life satisfaction with DA. Also, neuroticism and conscientiousness had a direct and positive relationship with DA.
The results of the current research, consistent with the results of Kardis et al., (2022) and Rafezi, (2022), showed a significant negative relationship between extroversion and DA. Extroversion may facilitate coping with DA. Because extroverted people often use the support of friends and family in difficult times, and therefore, having a strong support network, they may feel less alone and hopeless when facing life’s challenges. Also, extroverts are usually good at communicating with others and may feel more comfortable and relaxed when facing difficult issues, such as death by talking and sharing their experiences and feelings. This highlights the great importance of extroversion in shaping the quality of social relationships, especially in the elderly living in nursing homes; because research shows that the feeling of loneliness is significantly higher in the elderly living in nursing homes compared to elderly people living in families (Heidari et al., 2016). Therefore, it seems that extraversion can act as a shield against DA by increasing relationships and social support. On the other hand, while confirming the negative relationship between DA and extroversion, Norouzian and Peiadeh Kohsar (2022) indicated that extroversion facilitates the use of adaptive coping strategies, such as seeking social support, positive thinking, and problem-oriented strategies, thereby reducing depression and DA. Extroversion increases the feeling of power and mastery over life by increasing social support and thus can reduce DA in the elderly. This explanation is consistent with the results of Krause (2012). They showed that strong spiritual support moderated the relationship between stress and anxiety only among highly extroverted participants.
The results of the present study showed a positive relationship between PD emotionality and DA. Emotionality, as one of the PDs, refers to a person’s willingness to experience and express strong and intense emotions. People with high emotionality usually strongly and easily react to various developments and events and show their positive or negative emotions openly. The elderly with high emotionality may tend to react immediately and strongly to news or thoughts of death. This characteristic may increase their anxiety and stress due to the observation of illness and death of peers living in nursing homes. Also, these people may experience some form of depression or severe anxiety about the topic of death. In addition, individuals with high emotionality may experience extreme changes in emotional and affective states, which may reduce their ability to cope with DA. Individuals with negative emotional PDs may be prone to negative thinking and attitudes, despair, excessive worry, and excessive distress. These attitudes and feelings may exacerbate DA. People with higher negative emotionality, when faced with negative emotions such as fear and anger, go through a longer return period to reach a normal state, which can interfere with their ability to deal with emotions and regulate them. Therefore, people with emotional PDs may have more difficulty in using effective ways to deal with DA. This result is consistent with Mock, (2021), which identified negative emotionality as a predictor of DA and aging anxiety.
The results of the present study showed that humility has a negative relationship with DA, which is consistent with the results of Kesebir (2014). Thus, higher levels of humility predict lower levels of DA. Humility is characterized by a willingness to accept oneself and live without comforting illusions. As a result, humble individuals appraise death-related thoughts as less threatening and are less likely to exhibit potentially destructive behavior patterns. Individuals high in humility do not engage in selfish moral detachment following reminders of mortality, while individuals low in humility do. A possible explanation is that people with humility PDs, having a better shield against the fear of death, can interpret and interpret death-related thoughts differently, in the sense that death-related thoughts for people with humility PDs lead them to find the meaning of life and the way of life inspires. As a result, death makes them want to live up to values and behave in morally appropriate ways. These results suggest that a calm self, characterized by humility, acts as a shield against DA. Higher humility during reminders of death preserves self-control in individuals. People with humility PDs have a less intrusive “self” that is secure in their reality in the sense that the “self” doesn’t bother them as much as possible. Hence, threats to the self, including the possibility of death, are less of a concern for people with humility PDs. They are less reactive and do not resort to adverse defenses to ward off threats. In addition, humility requires a willingness to see the larger context and a careful and non-defensive assessment of one’s place in it. It makes sense that people with humility PDs are more at peace with accepting the nature of existence, including the finiteness of life. Given this set of related reasons, humility appears to protect against DA and prevent destructive ways of dealing with one’s death. Humility requires seeing and accepting the truth about yourself. In its most basic sense, it means knowing your strengths and weaknesses and coming to terms with your shortcomings. As a result, humility itself is largely protected from the need for distortions and defensive responses to self-threats. However, at a deeper level, humility also requires a careful judgment of one’s place in the larger context of existence. Therefore, the person with humility PDs is probably more aware of this existential reality of life and death and existence. For people with humility PDs, this makes death a lesser tragedy and potentially a source of clarity and guidance on how to live (Kesebir, 2014).
Second hypothesis: HA is related to DA in the elderly living in nursing homes.
The results of the second hypothesis test showed that HA has a positive and significant relationship with DA in the elderly living in nursing homes. This result is consistent with the results of other researchers (Söğütlü & Göktaş, 2021; Ghiasi et al., 2021; Birgit et al., 2018) who found a positive relationship between DA and HA between cancer patients and their caregivers, patients with COVID-19, and the elderly and.... Based on the results of Söğütlü & Göktaş, (2021), exposure to one’s illness and that of others, as well as experiencing the loss of loved ones, is associated with increased HA and DA.
The elderly experience a lot of worries about their health and physical functions due to the reduction of body immunity and physical vulnerability; sometimes, these thoughts and concerns cause people to consider simple physical symptoms as serious diseases, suffer from HA or even self-diagnosis disorder (Asadi et al., 2023) and increase their DA (Haroon et al., 2018). Experiencing unfamiliar physical symptoms, performing medical tests, or contracting a physical disease in the elderly or other elderly in the nursing home can lead to mental preoccupation and false beliefs about having a progressive disease. This situation increases the elderly’s misinterpretation of physical symptoms. Some other elderly people believe that health means that a person does not have any symptoms or even a small illness, and they consider every symptom as an illness. Sometimes this situation causes them to seek to ensure their health too much or to focus excessively on their bodily sensations (Lebel et al., 2020); As a result, HA increases and complicates their physical symptoms, such as increased heart rate, increased breathing rate, chest pain, increased breathing, digestive problems, feeling hot, fatigue, and in some cases, muscle pain (American Psychiatric Association, 2020).
Ambiguity intolerance as a behavioral, cognitive, and negative emotional response to uncertainty increases bias in information processing and disrupts threat assessment and coping skills (Dugas et al., 2004). In other words, elderly people with low ambiguity tolerance, when faced with ambiguous situations, such as numerous physical symptoms that indicate a decline in their health status, overestimate the possibility of negative consequences, such as lifelong disability and death, and their negative beliefs about ambiguity tolerance cause ambiguous information can be interpreted as threatening. As a result, ambiguous information, such as a simple increase in blood pressure or a common digestive problem is interpreted as catastrophic and negative, which increases DA in them. These explanations are consistent with the results of other studies indicating that ambiguity tolerance affects patients’ pain experience through increased worry, inconsistent cognitions, and inconsistent emotion regulation methods, such as catastrophizing (López-Martínez et al., 2022).
Therefore, emotion regulation strategies can also be considered as one of the crucial factors affecting the DA and health of the elderly. When ambiguity is high (such as in a situation related to an ambiguous health condition, its outcome, or disease prognosis), older adults with higher ambiguity intolerance are more likely to be biased in information processing, processing the situation negatively and emphasizing On the negative points of the consequences and presenting a catastrophic interpretation of the situation, they experience more negative emotions, such as anxiety and stress, and further, with the use of incompatible emotion regulation strategies (self-blame and other-blame, catastrophizing, rumination), DA increases in them. A negative orientation towards illness and death increases anxiety (HA and DA). Also, pessimism about the abilities of themselves and caregivers to solve physical problems increases the feeling of failure in the elderly and they view the consequences of physical problems with a more negative view; this hurts their problem-solving process and while increasing HA, it also increases DA.
Elderly people with higher HA may use maladaptive coping strategies and maladaptive emotion regulation strategies, reducing the likelihood of treatment compliance. Non-compliance with treatment makes their health condition more complicated and while increasing HA, it can also increase DA. This explanation is consistent with the results of Ghassempour et al. (2022), who showed that emotion regulation methods have a direct effect on treatment adherence.
Third hypothesis: HA in the elderly living in nursing homes mediates the relationship between PDs and DA.
The results of the third hypothesis test showed that HA in the elderly living in nursing homes mediates the relationship between PDs emotionality factor and DA positively and the relationship between extroversion, humility, and conscientiousness factors and DA negatively and significantly. No research investigates the mediating role of HA in the relationship between PDs and DA. However other researchers have examined the relationships between PDs and constructs close to HA and DA, and their results are consistent with the results of the current research. For example, Ghiasi et al., (2021) showed that personality is an essential factor in predicting the quality of life-related to health and DA. Nikčević et al. (2021) also showed that HA plays a mediating role in the relationship between PDs and anxiety and depression.
Emotionality by increasing reactivity to thoughts or news related to illness and death, followed by increased vulnerability to negative emotions and hyperawareness of physical and emotional symptoms can increase types of anxiety, such as HA and DA in the elderly. The findings of other researchers also support this finding. For example, Mock, (2021) has shown that negative emotionality predicts DA and aging anxiety. Ghiasi et al., (2021) found that neuroticism was a predictor of quality of life-related to health and DA. Neuroticism, along with features, such as the tendency to experience mental distress and negative mood, anxiety, depression, anger-hostility, and vulnerability to stress, increases people’s vulnerability to experiencing negative emotions, HA and DA. While extraversion has an inverse relationship with DA by increasing health-related QoL scores. In explaining these results, it can be said that extreme changes in emotional states can reduce the ability of the elderly to deal with HA and DA. A reciprocal relationship is observed between emotionality and coping that affects HA and DA. These results are consistent with the cognitive-behavioral model of HA. Specifically, high emotionality may increase health concerns or DA, leading to the use of behavioral strategies for coping with anxiety aimed at reducing anxiety in the short term (e.g. avoidance or reassurance seeking). As Amani and Ghodrati (2023) have shown, emotion-oriented coping strategies mediate the relationship between emotionality and HA. Further (based on the theory of panic management), although the use of “adjacent” defenses can remove thoughts and concerns related to death from the conscious level, their remaining in the unconscious level is still considered a threat to the mental health of the elderly, and if they do not find a way to solve this threat, their DA will increase and can lead to the collapse of the mental structure.
The mediating role of HA in the relationship between extroversion, humility, and conscientiousness with DA can be explained based on the crucial and moderating role of social support. People with extraversion and conscientiousness PDs have stronger social connections that facilitate them to receive social support. Social support reduces perceived stress and leads to an increase in positive affect and a decrease in anxiety and depression. Establishing positive communication strengthens the cardiovascular, neuroendocrine, and immune systems. Individuals with healthy social support are less likely to experience cognitive decline associated with aging (Bai et al., 2020). Increased relationships and social support can act as a shield against DA. Therefore, receiving more social support in elderly people with extraversion and conscientiousness PDs may moderate the effect of HA on DA by increasing mental and physical health. Also, the mediating role of HA in the relationship between humility and DA in elderly people can be influenced by the mechanisms of social support and spirituality based on the research results of Krause (2020). Krause (found that elderly people who go to church are more likely to receive spiritual support from church members, more spiritual support is associated with having a closer relationship with God. The elderly with a closer relationship with God have more humility, and over time, they value their health more. Therefore, in the results of the current research, the mediating role of HA in the relationship between humility and DA in elderly people can be explained as follows: Since humility is one of the correlates of agreeableness and conscientiousness, the elderly with higher humility, while establishing better relationships with others, get higher social and spiritual support, and more conscientiously observe health-related behaviors. As a result, they have higher mental and physical health. On the other hand, they accept their own and others’ strengths and weaknesses better, and by accepting their situation, their HA and DA are reduced.
In this regard, considering the role of HA in predicting DA, it is suggested to implement psychotherapy interventions to prevent and manage the HA of the elderly in the health center. Therefore, health anxiety mediates the relationship between personality dimensions and death anxiety. The research model was different in terms of fit with the data of two groups of women and men.
Conclusion
Multiple psychological mechanisms can predict death anxiety in the elderly. HA mediates the relationship between PDs and DA. The research model was different in terms of fit with the data of two groups of women and men.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran Central Branch, Islamic Azad University, Tehran, Iran (Code: IR.IAU.CTB.REC.1402.172).
Funding
This study was extracted from the PhD dissertation of Mahjoubeh Zanganeh Gheshlaghi, approved by the Department of Psychology, Faculty of Psychology and Educational Sciences, Tehran Central Branch, Islamic Azad University, Tehran, Iran.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Thanks for the support and cooperation of the seniors who cooperated with the writing team.
References
he elderly is one of the most challenging stages of life and a complex set of physical, psychological, and social changes that elderly people face and it is considered a heavy burden for their psychosocial functioning and mental health (Bahar et al., 2022). One of the common psychological problems in old age is anxiety because this period is full of all kinds of feelings of deficiencies and inabilities. Studies show that the elderly are exposed to more anxiety due to reduced self-confidence, lack of activity and movement, loss of friends and relatives, reduced material and physical independence, and chronic diseases. Perhaps the most common anxiety is death anxiety (DA) (Jangi Jahantigh et al., 2022).
Health anxiety (HA) can also be more common in this age group due to the physical vulnerability of the elderly and their awareness of this issue (Safari et al., 2022). HA is a psychological experience characterized by a perceived threat to one’s health that produces physical and emotional symptoms of anxiety. In experiencing HA, a person perceives feelings and physical changes as symptoms of illness. Although normal levels of HA have a protective effect and lead to beneficial health and health-related behaviors, high levels of anxiety are problematic and harmful to mental health (Safari et al., 2022). Anxiety plays a role in reducing physical health, life satisfaction, and quality of life (QoL) of the elderly. Elderly people who experience symptoms of anxiety are more likely to show impairments in different areas of cognitive functioning compared to the elderly who have less anxiety (Majdara et al., 2015). HA or self-diagnosis is common but understudies due to the spread of negative life experiences, including problems and diseases caused by aging and the death of family and relatives (El-Gabalawy et al., 2013). HA is an individual’s mental preoccupation with false beliefs or a serious, dangerous disease growing and it is a disorder that puts a significant burden on health services (Axelsson & Hedman-Lagerlöf, 2022). Thielsch et al. (2015) have proposed the metacognition and intolerance of uncertainty and worry. According to the metacognitive model, anxiety continues until the person recognizes that they can effectively deal with the anticipated danger, but uncertainty about their health and longevity in the elderly increases anxiety and related cognitive and physical symptoms (Davey & Wells, 2008).
Glasser (2019) emphasizes the choice theory on the personality dimensions (PDs), conscientiousness, and responsibility in the individual to achieve the meaning of life. A person should identify the behavior that he/she is trying to correct, pay all his/her attention to it, and not make any excuses to deny his/her responsibility. A conscientious person can make better choices by re-evaluating his/her desires and behaviors to achieve satisfaction from life, and ultimately achieve a more flexible, meaningful, and enjoyable life. Ashton et al. (2014) proposed HEXACO PDs. This model assumes that PDs can be summarized in six dimensions, honesty-humility, emotionality, extraversion, agreeableness, conscientiousness, and openness to experience (Lee & Ashton, 2018). Based on Glaser’s choice theory, since humans can make conscious choices, exercise their will, and consider the future, therefore, according to this view, every elderly person is responsible for their health, and it seems that HEXACO conscientiousness should be involved in this matter (Glasser, 2019). In this regard, in the study of Gonzatti et al., the elderly obtained the highest scores in the dimension of conscientiousness and responsibility compared to other age groups (Gonzatti et al., 2018).
Based on what has been said, the current research aims to answer this question: Does a causal model of DA in the elderly who lived in nursing homes based on PDs with the mediation of HA and the moderating role of gender fit the collected data?
Materials and Methods
The present research was conducted by correlation method and using path analysis. The statistical population of the research included all the elderly who lived in private nursing homes in Tehran City in the summer and autumn of 2023, of which, 340 people were selected by the convenience sampling method. In the current research, the method of “ the number of cases (N) to the number of estimated parameters (q), N:q” was used to determine the sample size. Based on the N:q rule, the sample-size-to-parameters ratio of 5:1 results in a small sample size, a ratio of 10:1 is a suitable sample size, and a ratio of 20:1 is an optimal sample size (Myers et al., 2016). Based on this method, in the present study, the sample size was determined to be 10 times the number of available parameters (21 parameters) and equal to 340 people.
Inclusion and exclusion criteria
The inclusion criteria included 65 to 75 years old, reading and writing education, not being abandoned, not being unsupervised or poorly supervised, and being a widow. The exclusion criteria included simultaneous use of psychiatric drugs and receiving psychotherapy interventions, suffering from acute chronic physical diseases including acute diabetes, high blood pressure, and serious cardiovascular diseases.
Procedures
Templer DA scale (DAS)
Templer DAS (1970) includes 15 items that measure an individual’s attitudes toward death-related topics. Subjects specify their answers to each question with yes or no options. The scores of this scale range from 0 and 15, where a high score indicates an intense fear of death (Thanatophobia) (Templer, 1970). The studies conducted on the validity and reliability of the DAS scale show that this scale has acceptable validity. In the origin section, the test re-test reliability (i.e. intraclass correlation) of the DAS scale is 0.83 and its concurrent validity is reported based on the correlation with the overt anxiety scale of 0.27 and the depression scale of 0.4. Rajabi and Naderi Nobandegani (2020) investigated the reliability and validity of the DAS scale in Iran and reported the internal consistency coefficient as 0.73 and the correlation of the DAS scale with the overt anxiety scale as 0.34 as an index of convergent validity of the instrument.
Short HA inventory (SHAI)
The SHAI (Salkovskis et al., 2002), includes 18 items that are scored on a 4-point Likert scale from 0 to 3. The minimum and maximum score of SHAI is equal to 0 and 54, respectively. A higher score in this tool means a higher level of HA. In the research of Salkovskis et al., (2002) Cronbach’s α coefficient for this tool was reported as 0.89. Nargesi et al. (2017) reported the correlation of this tool with the “Ahvaz self-diagnosis test”=0.75 and Cronbach’s α coefficient for this tool=0.87.
The HEXACO personality inventory
The HEXACO personality inventory-revised (HEXACO-PI-R) (Lee & Ashton, 2018) contains 100 items that measure 6 PDs, including honesty-humility, emotionality, extraversion, agreeableness, conscientiousness, and openness to experience in a 5-point Likert scale from completely disagree=1 to completely agree=5. Karimi and Minaei (2016) obtained Cronbach’s α coefficients in the range of 0.74 to 0.62 for this instrument. They reported the correlation of this tool with the NEO personality inventory-revised as an index of convergent validity of the tool.
Results
A total of 340 elderly people (185 women and 155 men) participated in the present study with the Mean±SD age of age group for women and men equal to 66.24 and 3.19, respectively. Table 1 presents the Mean±SD of PDs (honesty-humility, emotionality, extraversion, agreeableness, conscientiousness, and openness to experience), HA, and DA.
Univariate normal distribution
Table 1 presents the correlation coefficients between the variables, based on which, the direction of the correlation between the variables was consistent with the expectations and the theories of the research field. In this research, to evaluate the assumption of univariate normal distribution, Kurtosis, and skewness of the variables and to evaluate the assumption of collinearity of values, variance inflation factor (VIF) and tolerance coefficient were investigated. (Table 2).
Table 2 shows that the Kurtosis and skewness values of all components are in the range of ±2. This result indicates that the assumption of univariate normal distribution among the data is valid (Kline, 2023). Also, as shown in Table 2, the assumption of collinearity was valid among the data of the current research. Because the tolerance coefficient values of predictor variables were larger than 0.1 and the VIF values of each of them were smaller than 10. According to Myers et al., (2016), the tolerance coefficient is less than 0.1 and the value of the VIF is higher than 10, indicating that the assumption of collinearity is not established.
Multivariate normal distribution (MND)
In this research, to evaluate the establishment or non-establishment of the assumption of MND, the information analysis related to “the Mahalanobis distance” was used. The values of Skewness and Kurtosis were obtained as 0.93 and 1.18, respectively. Therefore, the value of both indices was in the range of ±2, confirming the assumption of MND among the data. Finally, to evaluate the homogeneity of variances, the scatter diagram of the standardized residuals of the errors was examined and the evaluations showed that the assumption is also valid among the data.
Model specification
In the research model, it was assumed that PDs are mediated by HA and DA. In this research, the path analysis (PA) method was used to analyze the data. To do this, version 24 of AMOS software and the maximum likelihood estimation method were used.
Because 8 indicators were found in the research model, therefore its known elements were (v[v+1]/2=36), and on the other hand, the number of unknown elements was also 36, and as a result, its degrees of freedom (df) was equal to zero (0=36-36). Models in which the df is equal to zero are called just-identified. In just-identified models, the estimation parameters and fitness indices are assumed to be complete and not estimated (Weston & Gore, 2006).
The evaluation of the path coefficient (PC) in the initial model showed that the PC of none of the two factors of agreeableness and openness to experience with the two variables of HA and DA is not significant. For this reason, two factors were left out in the modification of the model. In addition, the direct PC between emotionality and DA on the one hand and the direct PC between the humility factor and DA on the other hand were not statistically significant. Therefore, these two paths were removed from the model. After modifying the model, the fit of the model was again evaluated with the collected data. Table 3 presents the fit indices of the model after modification.
Table 3 shows that after modifying the model, the fit indices obtained from the PA support the acceptable fit of the model with the compiled data. Table 4 presents the PC in the research model.
According to the model presented in Figure 1, in addition to removing the two factors of agreeableness and openness to experience, the direct PC between emotionality and DA, as well as the direct PC between the honesty factor and DA due to lack of significance, were removed during the model modification. Table 4 shows that the PC (direct and indirect PC) between PDs extraversion (β=-0.284, P=0.001) and conscientiousness (P=0.001, β=-0.328) is negative and significant with DA. Also, the PC between HA and DA (P=0.001, β=0.457) is positive and significant. The indirect PC between PD extraversion (P=0.001, β=0.110), conscientiousness (P=0.142, β=0.001) and humility (P=0.001, β118 β=-0) with DA was negative and significant. While the indirect PC between PD emotionality (P=0.001, β=0.105) and DA was positive and significant. Based on this, it can be concluded that HA among the elderly mediates the relationship between the three PDs of extroversion, humility, and conscientiousness with DA negatively and the relationship between PD emotionality and DA positively and significantly.
Figure 1 shows the standard parameters in the research model. As shown, the sum of squared multiple correlation (R2) for DA was equal to 0.25. This shows that the PD factors of humility, extroversion, conscientiousness, and emotionality together with HA explain 25% of the variance of DA in the elderly.
Discussion
First hypothesis: PDs are related to DA in the elderly living in nursing homes.
The results of statistical analysis showed that the PC between the PD factors of extroversion, conscientiousness, and humility with DA was negative and the PC between the PD factor of emotionality with DA was positive and significant. Therefore, in the test of the first hypothesis, it was concluded that among the PD factors, emotionality is positively related, and the PD factors of extroversion, conscientiousness, and humility are negatively and significantly related to the HA of the elderly living in nursing homes.
These results are consistent with the results of other researchers (Kardis et al., 2022; Veisi et al., 2023; Mock, 2021; Moulaei et al., 2023; Noroziyan and Peyadekoohsar, 2022; Rafezi, 2022; Tabe Bordbar et al., 2018; Khayat et al., 2018).
According to Kardis et al., (2022), a significant negative relationship is observed between extraversion and DA. While confirming the relationship between PDs and DA, Veisi et al., (2023) showed that DA plays a mediating role in the relationship between PDs and psychological well-being in people with coronavirus. Noroziyan and Peyadekoohsar, (2022) showed that neuroticism and conscientiousness have a significant positive and negative relationship with DA, respectively. According to Rafezi, (2022), a positive relationship is observed between neuroticism and DA, and a negative and significant relationship between PDs of extroversion, flexibility, and conscientiousness and DA. Tabe Bordbar et al., (2018) showed that neuroticism/negative emotionality positively and significantly, and extroversion and responsibility negatively and significantly can predict DA in the elderly. Khayat et al., (2018) observed a negative and direct relationship between agreeableness and life satisfaction with DA. Also, neuroticism and conscientiousness had a direct and positive relationship with DA.
The results of the current research, consistent with the results of Kardis et al., (2022) and Rafezi, (2022), showed a significant negative relationship between extroversion and DA. Extroversion may facilitate coping with DA. Because extroverted people often use the support of friends and family in difficult times, and therefore, having a strong support network, they may feel less alone and hopeless when facing life’s challenges. Also, extroverts are usually good at communicating with others and may feel more comfortable and relaxed when facing difficult issues, such as death by talking and sharing their experiences and feelings. This highlights the great importance of extroversion in shaping the quality of social relationships, especially in the elderly living in nursing homes; because research shows that the feeling of loneliness is significantly higher in the elderly living in nursing homes compared to elderly people living in families (Heidari et al., 2016). Therefore, it seems that extraversion can act as a shield against DA by increasing relationships and social support. On the other hand, while confirming the negative relationship between DA and extroversion, Norouzian and Peiadeh Kohsar (2022) indicated that extroversion facilitates the use of adaptive coping strategies, such as seeking social support, positive thinking, and problem-oriented strategies, thereby reducing depression and DA. Extroversion increases the feeling of power and mastery over life by increasing social support and thus can reduce DA in the elderly. This explanation is consistent with the results of Krause (2012). They showed that strong spiritual support moderated the relationship between stress and anxiety only among highly extroverted participants.
The results of the present study showed a positive relationship between PD emotionality and DA. Emotionality, as one of the PDs, refers to a person’s willingness to experience and express strong and intense emotions. People with high emotionality usually strongly and easily react to various developments and events and show their positive or negative emotions openly. The elderly with high emotionality may tend to react immediately and strongly to news or thoughts of death. This characteristic may increase their anxiety and stress due to the observation of illness and death of peers living in nursing homes. Also, these people may experience some form of depression or severe anxiety about the topic of death. In addition, individuals with high emotionality may experience extreme changes in emotional and affective states, which may reduce their ability to cope with DA. Individuals with negative emotional PDs may be prone to negative thinking and attitudes, despair, excessive worry, and excessive distress. These attitudes and feelings may exacerbate DA. People with higher negative emotionality, when faced with negative emotions such as fear and anger, go through a longer return period to reach a normal state, which can interfere with their ability to deal with emotions and regulate them. Therefore, people with emotional PDs may have more difficulty in using effective ways to deal with DA. This result is consistent with Mock, (2021), which identified negative emotionality as a predictor of DA and aging anxiety.
The results of the present study showed that humility has a negative relationship with DA, which is consistent with the results of Kesebir (2014). Thus, higher levels of humility predict lower levels of DA. Humility is characterized by a willingness to accept oneself and live without comforting illusions. As a result, humble individuals appraise death-related thoughts as less threatening and are less likely to exhibit potentially destructive behavior patterns. Individuals high in humility do not engage in selfish moral detachment following reminders of mortality, while individuals low in humility do. A possible explanation is that people with humility PDs, having a better shield against the fear of death, can interpret and interpret death-related thoughts differently, in the sense that death-related thoughts for people with humility PDs lead them to find the meaning of life and the way of life inspires. As a result, death makes them want to live up to values and behave in morally appropriate ways. These results suggest that a calm self, characterized by humility, acts as a shield against DA. Higher humility during reminders of death preserves self-control in individuals. People with humility PDs have a less intrusive “self” that is secure in their reality in the sense that the “self” doesn’t bother them as much as possible. Hence, threats to the self, including the possibility of death, are less of a concern for people with humility PDs. They are less reactive and do not resort to adverse defenses to ward off threats. In addition, humility requires a willingness to see the larger context and a careful and non-defensive assessment of one’s place in it. It makes sense that people with humility PDs are more at peace with accepting the nature of existence, including the finiteness of life. Given this set of related reasons, humility appears to protect against DA and prevent destructive ways of dealing with one’s death. Humility requires seeing and accepting the truth about yourself. In its most basic sense, it means knowing your strengths and weaknesses and coming to terms with your shortcomings. As a result, humility itself is largely protected from the need for distortions and defensive responses to self-threats. However, at a deeper level, humility also requires a careful judgment of one’s place in the larger context of existence. Therefore, the person with humility PDs is probably more aware of this existential reality of life and death and existence. For people with humility PDs, this makes death a lesser tragedy and potentially a source of clarity and guidance on how to live (Kesebir, 2014).
Second hypothesis: HA is related to DA in the elderly living in nursing homes.
The results of the second hypothesis test showed that HA has a positive and significant relationship with DA in the elderly living in nursing homes. This result is consistent with the results of other researchers (Söğütlü & Göktaş, 2021; Ghiasi et al., 2021; Birgit et al., 2018) who found a positive relationship between DA and HA between cancer patients and their caregivers, patients with COVID-19, and the elderly and.... Based on the results of Söğütlü & Göktaş, (2021), exposure to one’s illness and that of others, as well as experiencing the loss of loved ones, is associated with increased HA and DA.
The elderly experience a lot of worries about their health and physical functions due to the reduction of body immunity and physical vulnerability; sometimes, these thoughts and concerns cause people to consider simple physical symptoms as serious diseases, suffer from HA or even self-diagnosis disorder (Asadi et al., 2023) and increase their DA (Haroon et al., 2018). Experiencing unfamiliar physical symptoms, performing medical tests, or contracting a physical disease in the elderly or other elderly in the nursing home can lead to mental preoccupation and false beliefs about having a progressive disease. This situation increases the elderly’s misinterpretation of physical symptoms. Some other elderly people believe that health means that a person does not have any symptoms or even a small illness, and they consider every symptom as an illness. Sometimes this situation causes them to seek to ensure their health too much or to focus excessively on their bodily sensations (Lebel et al., 2020); As a result, HA increases and complicates their physical symptoms, such as increased heart rate, increased breathing rate, chest pain, increased breathing, digestive problems, feeling hot, fatigue, and in some cases, muscle pain (American Psychiatric Association, 2020).
Ambiguity intolerance as a behavioral, cognitive, and negative emotional response to uncertainty increases bias in information processing and disrupts threat assessment and coping skills (Dugas et al., 2004). In other words, elderly people with low ambiguity tolerance, when faced with ambiguous situations, such as numerous physical symptoms that indicate a decline in their health status, overestimate the possibility of negative consequences, such as lifelong disability and death, and their negative beliefs about ambiguity tolerance cause ambiguous information can be interpreted as threatening. As a result, ambiguous information, such as a simple increase in blood pressure or a common digestive problem is interpreted as catastrophic and negative, which increases DA in them. These explanations are consistent with the results of other studies indicating that ambiguity tolerance affects patients’ pain experience through increased worry, inconsistent cognitions, and inconsistent emotion regulation methods, such as catastrophizing (López-Martínez et al., 2022).
Therefore, emotion regulation strategies can also be considered as one of the crucial factors affecting the DA and health of the elderly. When ambiguity is high (such as in a situation related to an ambiguous health condition, its outcome, or disease prognosis), older adults with higher ambiguity intolerance are more likely to be biased in information processing, processing the situation negatively and emphasizing On the negative points of the consequences and presenting a catastrophic interpretation of the situation, they experience more negative emotions, such as anxiety and stress, and further, with the use of incompatible emotion regulation strategies (self-blame and other-blame, catastrophizing, rumination), DA increases in them. A negative orientation towards illness and death increases anxiety (HA and DA). Also, pessimism about the abilities of themselves and caregivers to solve physical problems increases the feeling of failure in the elderly and they view the consequences of physical problems with a more negative view; this hurts their problem-solving process and while increasing HA, it also increases DA.
Elderly people with higher HA may use maladaptive coping strategies and maladaptive emotion regulation strategies, reducing the likelihood of treatment compliance. Non-compliance with treatment makes their health condition more complicated and while increasing HA, it can also increase DA. This explanation is consistent with the results of Ghassempour et al. (2022), who showed that emotion regulation methods have a direct effect on treatment adherence.
Third hypothesis: HA in the elderly living in nursing homes mediates the relationship between PDs and DA.
The results of the third hypothesis test showed that HA in the elderly living in nursing homes mediates the relationship between PDs emotionality factor and DA positively and the relationship between extroversion, humility, and conscientiousness factors and DA negatively and significantly. No research investigates the mediating role of HA in the relationship between PDs and DA. However other researchers have examined the relationships between PDs and constructs close to HA and DA, and their results are consistent with the results of the current research. For example, Ghiasi et al., (2021) showed that personality is an essential factor in predicting the quality of life-related to health and DA. Nikčević et al. (2021) also showed that HA plays a mediating role in the relationship between PDs and anxiety and depression.
Emotionality by increasing reactivity to thoughts or news related to illness and death, followed by increased vulnerability to negative emotions and hyperawareness of physical and emotional symptoms can increase types of anxiety, such as HA and DA in the elderly. The findings of other researchers also support this finding. For example, Mock, (2021) has shown that negative emotionality predicts DA and aging anxiety. Ghiasi et al., (2021) found that neuroticism was a predictor of quality of life-related to health and DA. Neuroticism, along with features, such as the tendency to experience mental distress and negative mood, anxiety, depression, anger-hostility, and vulnerability to stress, increases people’s vulnerability to experiencing negative emotions, HA and DA. While extraversion has an inverse relationship with DA by increasing health-related QoL scores. In explaining these results, it can be said that extreme changes in emotional states can reduce the ability of the elderly to deal with HA and DA. A reciprocal relationship is observed between emotionality and coping that affects HA and DA. These results are consistent with the cognitive-behavioral model of HA. Specifically, high emotionality may increase health concerns or DA, leading to the use of behavioral strategies for coping with anxiety aimed at reducing anxiety in the short term (e.g. avoidance or reassurance seeking). As Amani and Ghodrati (2023) have shown, emotion-oriented coping strategies mediate the relationship between emotionality and HA. Further (based on the theory of panic management), although the use of “adjacent” defenses can remove thoughts and concerns related to death from the conscious level, their remaining in the unconscious level is still considered a threat to the mental health of the elderly, and if they do not find a way to solve this threat, their DA will increase and can lead to the collapse of the mental structure.
The mediating role of HA in the relationship between extroversion, humility, and conscientiousness with DA can be explained based on the crucial and moderating role of social support. People with extraversion and conscientiousness PDs have stronger social connections that facilitate them to receive social support. Social support reduces perceived stress and leads to an increase in positive affect and a decrease in anxiety and depression. Establishing positive communication strengthens the cardiovascular, neuroendocrine, and immune systems. Individuals with healthy social support are less likely to experience cognitive decline associated with aging (Bai et al., 2020). Increased relationships and social support can act as a shield against DA. Therefore, receiving more social support in elderly people with extraversion and conscientiousness PDs may moderate the effect of HA on DA by increasing mental and physical health. Also, the mediating role of HA in the relationship between humility and DA in elderly people can be influenced by the mechanisms of social support and spirituality based on the research results of Krause (2020). Krause (found that elderly people who go to church are more likely to receive spiritual support from church members, more spiritual support is associated with having a closer relationship with God. The elderly with a closer relationship with God have more humility, and over time, they value their health more. Therefore, in the results of the current research, the mediating role of HA in the relationship between humility and DA in elderly people can be explained as follows: Since humility is one of the correlates of agreeableness and conscientiousness, the elderly with higher humility, while establishing better relationships with others, get higher social and spiritual support, and more conscientiously observe health-related behaviors. As a result, they have higher mental and physical health. On the other hand, they accept their own and others’ strengths and weaknesses better, and by accepting their situation, their HA and DA are reduced.
In this regard, considering the role of HA in predicting DA, it is suggested to implement psychotherapy interventions to prevent and manage the HA of the elderly in the health center. Therefore, health anxiety mediates the relationship between personality dimensions and death anxiety. The research model was different in terms of fit with the data of two groups of women and men.
Conclusion
Multiple psychological mechanisms can predict death anxiety in the elderly. HA mediates the relationship between PDs and DA. The research model was different in terms of fit with the data of two groups of women and men.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Tehran Central Branch, Islamic Azad University, Tehran, Iran (Code: IR.IAU.CTB.REC.1402.172).
Funding
This study was extracted from the PhD dissertation of Mahjoubeh Zanganeh Gheshlaghi, approved by the Department of Psychology, Faculty of Psychology and Educational Sciences, Tehran Central Branch, Islamic Azad University, Tehran, Iran.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Thanks for the support and cooperation of the seniors who cooperated with the writing team.
References
Amani, M., & Ghodrati, S. (2023). The mediating role of coping strategies in the relationship between personality traits and perceived stress with health anxiety during the COVID-19 pandemic. Journal of Fundamentals of Mental Health, 25(3), 1-9. [Link]
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders.Washington, DC:American Psychiatric Association. [Link]
Asadi, L., Seyrafi, M., & Ahadi, M. (2023). [The effectiveness of existential therapy on health anxiety, loneliness, and death anxiety in the elderly (Persian)]. Medical Journal of Mashhad University of Medical Sciences, 66(1). [DOI:10.22038/mjms.2022.66447.3919]
Ashton, M. C., Lee, K., & de Vries, R. E. (2014). The HEXACO Honesty-Humility, Agreeableness, and Emotionality factors: a review of research and theory. Personality and social psychology review: an official journal of the Society for Personality and Social Psychology, Inc., 18(2), 139-152. [DOI:10.1177/1088868314523838]
Axelsson, E., & Hedman-Lagerlöf, E. (2022). Health anxiety. Comprehensive Clinical Psychology, 422-439. [DOI:10.1016/b978-0-12-818697-8.00231-4]
Bahar, A., Shahriary, M., & Fazlali, M. (2021). Effectiveness of logotherapy on death anxiety, hope, depression, and proper use of glucose control drugs in diabetic patients with depression. International Journal of Preventive Medicine, 12, 6. [DOI:10.4103/ijpvm.IJPVM_553_18] [PMID]
Bai, Y., Bian, F., Zhang, L., & Cao, Y. (2020). The impact of social support on the health of the rural elderly in China. International Journal of Environmental Research and Public Health, 17(6), 2004. [DOI:10.3390/ijerph17062004]
Aan de Stegge, B. M., Tak, L. M., Rosmalen, J. G. M., & Oude Voshaar, R. C. (2018). Death anxiety and its association with hypochondriasis and medically unexplained symptoms: A systematic review. Journal of Psychosomatic Research, 115, 58-65. [DOI:10.1016/j.jpsychores.2018.10.002] [PMID]
Davey, G. C., & Wells, A. (2008). Worry and its psychological disorders: Theory, assessment and treatment. New York: John Wiley & Sons Ltd. [Link]
Dugas, M. J., Schwartz, A., & Francis, K. (2004). Brief report: Intolerance of uncertainty, worry, and depression. Cognitive Therapy and Research, 28(6), 835-842. [DOI:10.1007/s10608-004-0669-0]
El-Gabalawy, R., Mackenzie, C. S., Thibodeau, M. A., Asmundson, G. J., & Sareen, J. (2013). Health anxiety disorders in older adults: Conceptualizing complex conditions in late life. Clinical Psychology Review, 33(8), 1096-1105. [DOI:10.1016/j.cpr.2013.08.010] [PMID]
Ghassempour, H., Darzi Azadboni, M., Mirzaian, B., Sangani, A., & Shakerian, S. (2022). [Modeling of early maladaptive schemas on adherence to treatment with the mediating role of cognitive emotion regulation and resilience in coronary heart patients (Persian)]. Journal of Nursing Education, 11(4), 13-24. [Link]
Ghiasi, Z., Alidadi, A., Payandeh, A., Emami, A., & Lotfinia, S. (2021). Health-related quality of life and death anxiety among hemodialysis patients. Zahedan Journal of Research in Medical Sciences, 23(2), e98400. [DOI:10.5812/zjrms.98400]
Glasser, W. (2019). A choice theory psychology guide to happiness: How to make yourself happy. William Glasser Institute. [Link]
Gonzatti, V., Cunha, A. M., Bastos, A. G., de Lima Argimon, I. I., Tatay, C. M., & Irigaray, T. Q.(2018). Personality factors in adults and the elderly: A comparative study. Avaliaçao Psicologica: Interamerican Journal of Psychological Assessment, 16(3), 256-260. [Link]
Heidari, M., Ghodusi Borujeni, M., & Naseh, L. (2016). [Comparison of self-efficacy and loneliness between community-dwelling & institutionalized older people (Persian)]. Salmand: Iranian Journal of Ageing, 11(1),142-151. [DOI:10.21859/sija-1101142]
Haroon, W., Khawaja, A. O., & Ghayas, S. (2018). Ego integrity, physical health status and death anxiety in older adults. Journal of Behavioural Sciences, 28(1), 18-32. [Link]
Jangi Jahantigh, L., Latifi, Z., & Soltanizadeh, M. (2022). [Effect of self-healing training on death anxiety and sleep quality of older women living in nursing homes (Persian)]. Salmand: Iranian Journal of Ageing, 17(3), 380-397. [DOI:10.32598/sija.2022.3319.1]
Kardes, V. C., Fidan, F., & Yiğit, M. (2022). Evaluation of the relationship between death anxiety and personality traits in hospitalized patients with covid-19. Ankara Medical Journal, 22(4), 485-498. [DOI:10.5505/amj.2022.15679]
Karimi, H., & Minaei, A. (2016).[ Psychometric characteristics and factor structure of Hexaco personality questionnaire and comparison of its relationship with five main personality factors among female and male students in Tehran (Persian)]. Psychometry, 6(22), 43-58. [Link]
Kesebir, P. (2014). A quiet ego quiets death anxiety: Humility as an existential anxiety buffer. Journal of Personality and Social Psychology, 106(4), 610–623. [DOI:10.1037/a0035814] [PMID]
Khayat, K., Tajeri, B., Pashang, S., & Malihiolzakereini, S. (2018). [Mediating role of life satisfaction in relationship between personality factors and death anxiety in the elderly (Persian)]. Journal of Research in Behavioural Sciences, 16(2), 189-197. [Link]
Kline, R. B. (2023). Principles and practice of structural equation modeling. New York: Guilford Publications. [Link]
Krause, N. (2012). Religious involvement, humility, and change in self-rated health over time. Journal of Psychology and Theology, 40(3), 199-210. [DOI:10.1177/009164711204000303]
Krause, N., Pargament, K. I., & Ironson, G. (2020). Assessing the relationships among spiritual social support, stress, and anxiety: Does extraversion also play a role in the coping process? Current Psychology, 39, 307-314. [DOI:10.1007/s12144-017-9764-8]
Lee, K., & Ashton, M. C. (2018). Psychometric properties of the HEXACO-100. Assessment, 25(5), 543-556. [DOI:10.1177/1073191116659134] [PMID]
Lebel, S., Mutsaers, B., Tomei, C., Leclair, C. S., Jones, G., & Petricone-Westwood, D., et al. (2020). Health anxiety and illness-related fears across diverse chronic illnesses: A systematic review on conceptualization, measurement, prevalence, course, and correlates. Plos One, 15(7), e0234124. [DOI:10.1371/journal.pone.0234124] [PMID]
López-Martínez, A. E., Ramírez-Maestre, C., Serrano-Ibáñez, E. R., Ruiz-Párraga, G. T., & Esteve, R. (2022). Intolerance of uncertainty moderates the relationship between catastrophizing, anxiety, and perceived pain in people with chronic nononcological pain. Pain Medicine, 23(10), 1793-1799. [DOI:10.1093/pm/pnac030] [PMID]
Majdara,, E., Bigdeli,, I., Najafi,, M., & Rashn,, S. (2016). [Direct and indirect impact of effects on anxiety and depression in elderly: The mediating role of difficulty in emotion regulation (Persian)]. Journal of Clinical Psychology, 8(2), 89-98. [DOI:10.22075/jcp.2017.2239]
Mock, C. E. (2021). Negative affectivity, emotional complexity and age as they relate to death and aging anxiety [PhD dissertation]. Edwardsville: Southern Illinois University. [Link]
Moulaei, K., Haghdoost, A. A., Bahaadinbeigy, K., & Dinari, F. (2023). The effect of the holy Quran recitation and listening on anxiety, stress, and depression: A scoping review on outcomes. Health Science Reports, 6(12), e1751. [DOI:10.1002/hsr2.1751] [PMID]
Myers, N. D., Celimli, S., Martin, J. J., & Hancock, G. R. (2016). Sample size determination and power estimation in structural equation modeling. In: N. An introduction to intermediate and advanced statistical analyses for sport and exercise scientists (pp. 267-284). [Link]
Nargesi, F., Izadi, F., Kariminejad, K., & Rezaii Sharif, A. (2017). [The investigation of the reliability and validity of the Persian version of the Health anxiety questionnaire in students of Lorestan University of Medical Sciences (Persian)]. Quarterly of Educational Measurement, 8(27), 147-160. [DOI:10.22054/jem.2017.19621.1495]
Nikčević, A. V., Marino, C., Kolubinski, D. C., Leach, D., & Spada, M. M. (2021). Modeling the contribution of the Big Five personality traits, health anxiety, and COVID-19 psychological distress to generalized anxiety and depressive symptoms during the COVID-19 pandemic. Journal of Affective Disorders, 279, 578-584. [DOI:10.1016/j.jad.2020.10.053]
Noroziyan, K., & Peyadekoohsar, A. (2022). [Prediction of death anxiety based on personality traits and god-image in patients with covid-19 (Persian)]. Journal of Research in Behavioural Sciences, 20(2), 204-219. [DOI:10.52547/rbs.20.2.204]
Rafezi, Z. (2022). [Predicting elderly death anxiety based on personality traits: The mediating role of forgiveness (Persian)]. Mental Health and Culture, 1(1), 15-31. [Link]
Rajabi, G., & Naderi Nobandegani, Z. (2020). Reliability and validity of the Persian version of reasons for death fear scale. Practice in Clinical Psychology, 8(1), 9-16. [DOI:10.32598/jpcp.8.1.9]
Safari, H., Bahrainian, S., & Ghanifar, M. H. (2022). [Health anxiety and related factors to it in recovered hospitalized elderly patients with Covid-19 (Persian)]. The Journals of Gerontology, 7(3), 45-55. [DOI:10.22034/JOGE.7.3.45]
Salkovskis, P. M., Rimes, K. A., Warwick, H. M., & Clark, D. M. (2002). The health anxiety inventory: Development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychological Medicine, 32(5), 843–853.[DOI:10.1017/S0033291702005822] [PMID]
Söğütlü, L., & Göktaş, S. Ş. (2021). The effect of COVID-19 pandemic on health anxiety, death anxiety and somatic symptoms in university students. Journal of Contemporary Medicine, 11(3), 323-329. [DOI:10.16899/jcm.878671]
Tabe bordbar, F., Esmaeili, M., & Asadi, R. (2019). [The prediction of death anxiety in the elderly based on personality types and mental health (Persian)]. Aging Psychology, 5(3), 239-249. [DOI:10.22126/jap.2019.4788.1374]
Templer, D. I. (1970). The construction and validation of a death anxiety scale. The Journal of General Psychology, 82(2), 165-177. [Link]"
Thielsch, C., Andor, T., & Ehring, T. (2015). Metacognition, intolerance of uncertainty and worry: An investigation in adolescents. Personality and Individual Differences, 74, 94- 98. [DOI:https://doi.org/10.1016/j.paid.2014.10.004]
Veisi, R., Kakabarai, K., Chehri, A., & Arefi, M. (2023). The role of death anxiety as a mediator in the relationship between personality types and psychological well-being in coronavirus disease-2019 patients. Journal of Education and Health Promotion, 12(1), 104. [DOI:10.4103/jehp.jehp_195_22] [PMID]
Type of Study: Original Research Article |
Subject:
Psychometric
Received: 2024/10/5 | Accepted: 2024/10/15 | Published: 2024/10/1
Received: 2024/10/5 | Accepted: 2024/10/15 | Published: 2024/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
