

Volume 11, Issue 4 (Autumn 2023)
PCP 2023, 11(4): 341-348 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghamari Kivi H, Jamshiddoust Miyanroudi F, Mousavi S, Ghavibazou E. Role of Types of Inner Speech in the Prediction of Symptoms of Anxiety, Depression, Somatization, and Distress in the Normal Population. PCP 2023; 11 (4) :341-348
URL: http://jpcp.uswr.ac.ir/article-1-878-en.html
URL: http://jpcp.uswr.ac.ir/article-1-878-en.html



1- Department of Counseling, Faculty of Educational Sciences and Psychology, Mohaghegh Ardabili University, Ardabil, Iran.
2- Department of Psychology, Faculty of Educational Sciences and Psychology, Mohaghegh Ardabili University, Ardabil, Iran. ,f.jamshiddoust@student.uma.ac.ir
3- Department of Psychology, Payame Noor University, Tehran, Iran.
4- Department of Counseling, Faculty of Education and Psychology, Alzahra University of Tehran, Tehran, Iran.
2- Department of Psychology, Faculty of Educational Sciences and Psychology, Mohaghegh Ardabili University, Ardabil, Iran. ,
3- Department of Psychology, Payame Noor University, Tehran, Iran.
4- Department of Counseling, Faculty of Education and Psychology, Alzahra University of Tehran, Tehran, Iran.
Full-Text [PDF 492 kb]
(3290 Downloads)
| Abstract (HTML) (3131 Views)
Full-Text: (1279 Views)
1. Introduction
Using inner speech is a cognitive strategy that can influence thoughts, feelings, and behaviors (Walter et al., 2019). Self-talk or internal discussions are ways in which a person communicates with himself. It is a natural cognitive process. Using inner speech may increase when faced with obstacles or challenges. People can either speak to themselves or use inner speech. This is referred to as inner speaking. Self-talk can be positive or negative. Van Raalte et al. (2016) distinguish between automatic, spontaneous, and often emotionally motivated self-talk, on the one hand, and directed and consciously motivated self-talk, on the other (Van Raalte et al., 2016). Cognitive-behavioral models emphasize the link between inner speech and the development of emotional disorders (Beck, 1972). This relationship is mainly considered from two different but complementary perspectives. One approach focuses on assessing the influence of positive and negative valence of thoughts on psychological maladjustment (Beck, 1972).
The second issue revolves around the hypothesis of cognitive content specificity and attempts to determine whether each affective disorder (i.e. depression and anxiety) is characterized by the perception of different contents (Beck, 1972). Self-talk is an internal dialogue. It is influenced by each individual’s subconscious and reveals his thoughts, beliefs, questions, and ideas. Self-talk can be negative or positive. It can be encouraging and painful. Most individuals’ self-talk depends on their personality. If people are optimistic, their self-talk may be more upbeat. The opposite is often true if people tend to be pessimistic.
Positive thinking and optimism can be effective stress management tools (Carroll, 2022). Having a more positive outlook on life can provide you with some health benefits. In the study conducted by Fritsch et al., the intensity of felt emotions and the intensity of external emotional reactions were lower when players reported only self-talk about their goals rather than spontaneous self-talk. These results support the relevance of dual-process self-talk. These results suggest that spontaneity is crucial for players to understand their emotions, but goal-directed self-talk is helpful in emotion regulation (Fritsch et al., 2022).
Research shows that how people talk to themselves during self-talk affects how they feel. For example, according to the source, using non-first-person pronouns, such as “you” and your name, instead of first-person pronouns, such as “I,” helps people adjust their thinking, their emotions, and behavior under social pressure. A 2019 study supports this theory, showing that using second-person pronouns in positive self-talk improves time and performance in endurance sports (Shadinger, 2020). Research, employing a variety of designs, has shown that self-talk strategies help athletes engage in positive self-talk and, in turn, reduce levels of competition-related anxiety (Walter et al., 2019). Additionally, a structural model that included pre-competitive anxiety provided further evidence of the association between self-talk and competitive anxiety. Finally, some methodological implications will be discussed (Marshall et al., 2016). Hatzigeorgiadis et al examined the effects of motivational self-talk on self-efficacy and performance. Research results suggest that enhancing self-efficacy may be a mechanism to explain the facilitative effects of self-talk on performance (Hatzigeorgiadis et al., 2008; Latinjak et al., 2016). Previous studies have shown its positive effects on anxiety, behavioral control under fearful conditions, and self-efficacy (Sadri Damirchi, 2020). Recently, in research conducted by Alderson-Day et al., it was discovered that inner speech can be studied using a precise method. The new scale called the varieties of inner speech questionnaire–revised (VISQ-R) includes both positive and negative self-talk. This research has shown that evaluative states are related to feelings of anxiety and depression and more evaluative states are associated with more negative self-esteem. However, motivational and regulatory self-talk is more related to the new positivity factor (Alderson-Day et al., 2017). Research in the field of sport psychology is more concerned with strong self-talk and presents aspects of self-regulatory and goal-directed behavior. However, the phenomenon of self-talk and its relationship with psychological trauma are less studied. This study shows that we can do research in this area, for example, people who are capable of positive/moderated self-talk will have a positive impact on their performance by practicing strategies instead of critical evaluation/self-talk (Davis et al., 2013). Positive/moderated self-talk has been shown to play a crucial role in creativity and visualization (Alderson et al., 2017).
According to Shi et al., reinforcing self-talk was not effective in overcoming anxiety. Speech anxiety seems to be primarily caused by frequent self-criticism (Shi, et al., 2017). McCarthy-Jones and Fernyhough showed that the factors “evaluative/motivational self-talk” and “presence of another person’s voice during self-talk” were positively related to anxiety (McCarthy & Fernyhough, 2011). The tendency toward auditory hallucinations was also positively correlated with conversational inner speech. In a recent study conducted by Alderson-Day et al. in a sample of healthy subjects, the VISQ factor “evaluative/motivational self-talk” was associated with lower self-esteem and more frequent dissociative experiences. Using structural equation modeling, they found that dissociation mediated between specific components of inner speech (evaluators and others participating in inner speech) and dispositions leading to auditory hallucinations (Alderson-Day, 2014). According to this literature review, the present study was conducted to investigate the role of self-talk styles in predicting symptoms of anxiety, depression, sleepiness, and distress in the general population in Iran. Because the signs of these problems are also present in normal people and can be easily studied.
2. Materials and Methods
Participants
The research method was a descriptive correlation type. The statistical population of the study included all 10 000 students from the University of Mohaghegh Ardabili in Iran in the academic year of 2019-2020. The sample size was calculated via Morgan’s table. To detect the optimum sample size, we considered a confidence level of 80% and a margin of error of 5%; therefore, the smallest sample size was calculated to be 378.
Inclusion criteria
The inclusion criteria included the existence of positive or negative self-talk in the subject, experiencing symptoms of anxiety, depression, physicalization, and distress, being a student in any field and level of study in the university, the consent of the person to complete the questionnaires, students at the University of Mohaghegh Ardabili interested in cooperation with more than 18 years of age.
Exclusion criteria
The exclusion criteria included the absence of clear self-talk in the subject, the existence of a specific mental disorder, and the absence of the subject’s request to implement the questionnaire.
Study procedure
To implement the study, all students were referred to the Sepand Counseling Center and interviewed at the Counseling Center of the University of Mohaghegh Ardabili in the first six months of 2019-2020. The population of this study was all those who were referred to the Sepand Counseling Center and students who were willing to complete the questionnaires. Additionally, all inclusion and exclusion criteria were considered in the early screening stages, and no sample loss was observed after the final selection. Furthermore, students completed the VISQ and the four-dimensional symptom questionnaire (4DSQ), including four symptom scales. Most sample participants were at the University of Mohaghegh Ardabili. Finally, a total of 372 of the 378 respondents completed the questionnaires, while 5 questionnaires were discarded due to incompletion. The researchers have followed all the current Iranian laws and regulations. In this study, ethical issues, such as informed consent, privacy, confidentiality, and anonymity were considered. According to the regulation of compliance with ethical standards, the consent form for free participation in the research was completed by all examinees.
Research tools
Varieties of inner speech questionnaire (VISQ)
Varieties of inner speech questionnaire–revised (VISQ-R) phenomenological properties of inner speech were assessed using the 35-item VISQ-R (Hurlburt, 1997). In addition to the original 18 items on dialogue, evaluation, succinctness, and the presence of others in self-talk, the expanded version includes new items on literal and metaphorical use of language, and how to define the speaker’s position and address as well as regulations on language usage, different moods, and positive moods /regulations. Responses were made on a seven-item frequency scale, in which respondents rated the frequency of experiencing the inner speech experience from “never” (1) to “always” (7). Exploratory factor analysis indicated a five-factor structure consisting of the three previous subscales (dialogue, succinctness, and others talking to themselves), an evaluative/critical factor, a positive/active factor, and a new regulation (Alderson-Day et al., 2018). The result of calculating Cronbach’s α coefficient in this study is 0.899.
The four-dimensional symptom questionnaire (4DSQ)
The four-dimensional symptom questionnaire (4DSQ) includes four symptom scales, distress (16 items), depression (6 items), anxiety (12 items), and lethargy (16 items) (Terluin, 2006). 4DSQ uses a 7-day time reference. Questions are answered on a 5-point frequency scale, from “not at all” to “very often or constantly.” To calculate the total score, responses were coded on a 3-point scale: “Never” (0 points), “sometimes” (1 point), “often,” “often,” and “very often or continuously” (2 points). By grouping the reaction categories “often,” “regularly,” and “very often or continuously,” we placed more weight on the number of symptoms experienced than on their perceived frequency. The 4DSQ is a self-report questionnaire consisting of 50 items divided into four scales. These items are formulated as questions similar to those that may be asked in daily primary care practice. The distress scale contains 16 items and has a score range of 0–32, the depression scale contains 6 items and has a range of 0–12, the anxiety scale contains 12 items and has a range of 0–24, and the somatization scale contains 16 items and has a range of 0–32 (Terluin et al., 2016). This questionnaire is based on the symptoms of mental patients. The internal correlation for the four scales is from 0.35 to 0.71. The result of calculating Cronbach’s α coefficient in the current study is equal to 0.95.
Data analysis
The research method is descriptive and correlational, using the statistical method of multivariate analysis of variance. Data were analyzed using-SPSS software, version 23. Descriptive statistics (Mean±SD, percentage, and frequency) and inferential statistics (Pearson correlation method) were used. Additionally, in this study, stepwise multivariate regression analysis to determine depression, including self-talk by others, explained 18% of the variance in depression.
3. Results
The demographic characteristics of the participants showed that 0.8% of the participants were diploma students, 83.1% were undergraduate students, 14% were postgraduate students, and 2.2% were doctoral students. The marital status of the subjects participating in the project was as follows, out of 212 women (57%) and 160 men (43%), 270 people (72.6%) were single and 102 people (27.4%) were married. Table 1 presents a positive correlation between types of inner speech with various symptoms of disorders, and as expected only a very slight and sometimes negative correlation between positive-regulatory inner speech and other disorders. Therefore, the highest correlated of correlation is between others’ inner speech and anxiety. Stepwise regression analysis was used to investigate the following questions.

In stepwise multivariate regression analysis for anxiety, inner speech (others) was entered first, which explained 20% of anxiety variance (F(1, 370)=45.95, P<0.001). After that, inner speech (positive-regulatory) was entered, which explained another 2% (F(1, 369)=10.98, P<0.001). Finally, inner speech (evaluation-critical) was entered, which explained the remaining 2% (F(1, 368)=41.12, P<0.001). Higher anxiety was correlated with inner speech (higher others, lower positive-regulatory, and higher evaluative/critical inner speech). In the stepwise multivariate regression analysis for depression, inner speech (others) was entered first, which explained 17% of the variance of depression (F(1, 370)=60.76, P<0.001). After that, inner speech (positive-regulatory) was entered, which explained another 2% (F(1, 369)=51.9, P<0.002). Finally, the inner speech (evaluation-critical) was included, which explained the remaining 5% (F(1, 368)=55.24, P<0.001). Higher depression was correlated with inner speech (others and higher critical evaluation and lower positive-regulatory). In the stepwise multivariate regression analysis for somatization, inner speech (others) were entered first, which explained 16% of the variance of somatization (F(1, 370)=90.72, P<0.001). After that, inner speech (dialogic) was entered, which explained another 1% (F(1, 369)=34.7, P<0.007). Finally, inner speech (evaluation-critical) was entered, which explained the remaining 9% (F(1, 368)=4.10, P<0.04). Higher somatization was correlated with higher inner speech (others, conversational, and evaluative-critical). In the stepwise multivariate regression analysis for distress, first, the self-evaluation-critical inner speech was entered, which explained 21% of the variance of distress (F(1, 370)=48.101, P<0.001). After that, inner speech (others) was entered, which explained another 5% (F(1, 369)=27.78, P<0.001). Finally, inner speech (positive-regulatory) was entered, which explained the remaining 3% (F(1, 368)=20.20, P<0.001). Higher distress was correlated with inner speech (higher evaluative-critical and others and lower positive-regulatory, Table 1).
According to Table 2, to more accurately determine the components of inner speech in people with symptoms of anxiety, depression, somatization, and distress, by standardizing the scores and converting them to Z scores, scores of 0-1 were selected, and typical people had disorders.

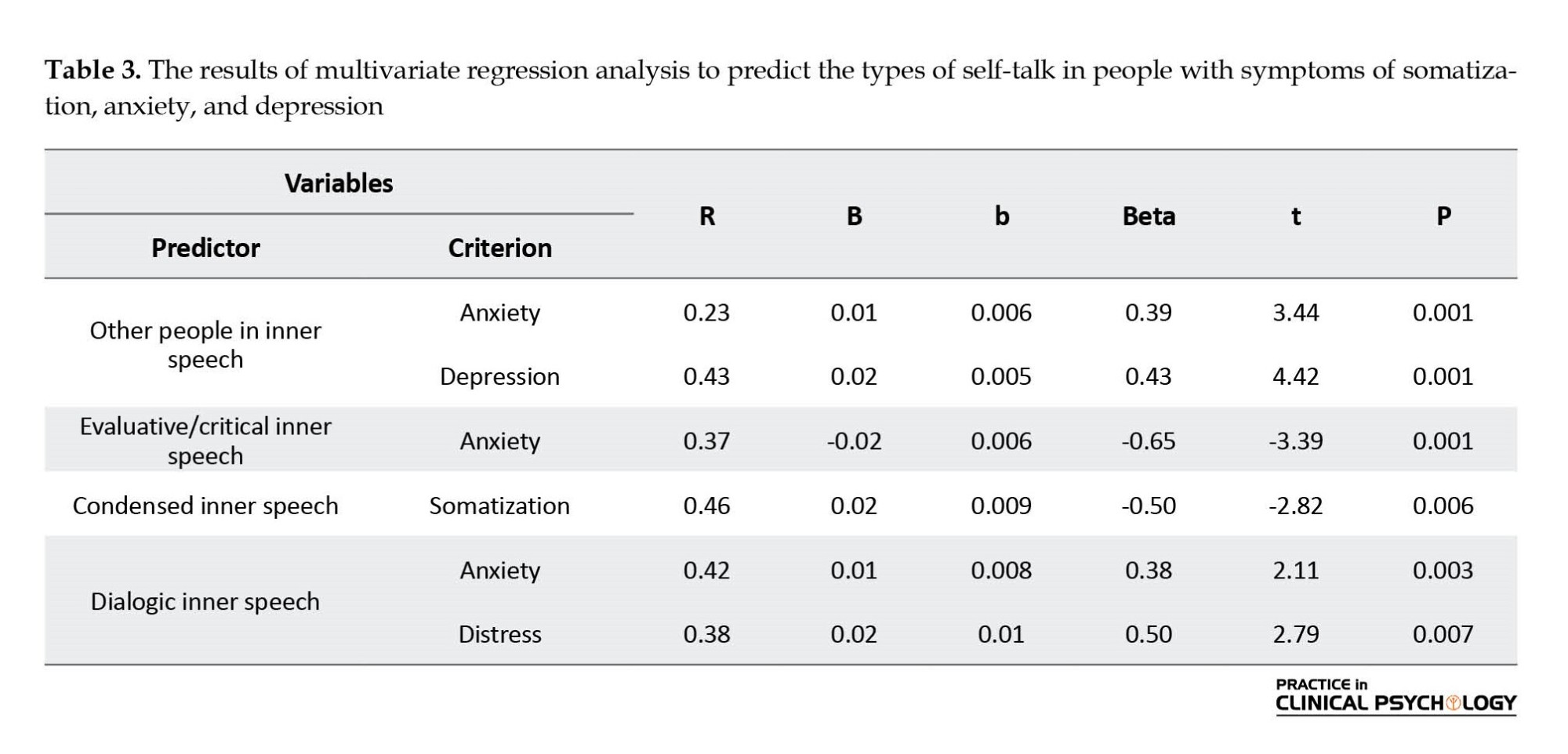
In Table 3, according to the stepwise multivariable regression analysis of anxiety, high anxiety was correlated with the inner speech of others, evaluative/critical (low), and dialectical. In the stepwise multivariable regression analysis for depression, the inner speech of others was included, which explained 18% of the variance of depression (P<0.001). Higher depression was correlated with others’ inner speech and stepwise multivariate regression analysis for somatization, condensed inner speech explained 22% of the variance of somatization (P<0.001). Higher somatization was correlated with lower condensed inner speech. In the stepwise multivariate regression analysis for distress, dialogic inner speech explained 14% of the variance of distress (P<0.04). Higher distress was correlated with dialogic inner speech.
4. Discussion
The present study was conducted to study and survey the role of types of inner speech in predicting symptoms of anxiety, depression, somatization, and distress in the normal population in Iran. According to the results of the current study, in people with symptoms of anxiety, depression, and somatization disorders, the inner speech of others was a stronger predictor compared to other types of inner speech. Talking to others means hearing the other person’s voice. In other words, a person says something to himself in another person’s voice. This is consistent with the study results of de Sousa et al., 2016, Perona et al., 2017, and Abitante, 2022. However, in the study conducted by de Sousa et al., condensed inner speech and talking to others were related to psychological trauma. However, the condensed inner speech was not decisive in any of the people with symptoms of anxiety, depression, and somatization disorders in the current study (de Sousa et al., 2016).
On the other hand, in subjects with distress symptoms, evaluative/critical inner speech was a good predictor. This result suggests that evaluative/critical inner speech primes individuals’ susceptibility to general distress as a common indicator of psychological distress. One thing to note in the current study is that positive-regulatory inner speech is significantly negative in people with symptoms of anxiety, depression, and distress (Perona et al., 2017; Abitante, 2022). Patients had higher scores in condensed inner speech than others, but not in conversational and evaluation inner speech. In the study conducted by McCarthy-Jones & Fernyhough (2011), inner speech was more prevalent among students with anxiety symptoms. McCarthy-Jones and Fernyhough believe that no serious field studies on inner speech were found. However, the study conducted by McCarthy-Jones and Fernyhough was designed to evaluate the phenomenological properties of inner speech types in conversational dimensions, the quality of density/expansion, the level of evaluation/arousal, and the extent to which inner speech integrates the voices of others (McCarthy & Fernyhough, 2011). In addition, the relationship between some types of disorders, such as anxiety and depression, and the tendency to auditory and visual hallucinations with inner speech was investigated. The results showed a positive correlation between anxiety and evaluative/critical inner speech and the presence of other people’s voices in inner speech (Perona et al., 2017).
5. Conclusion
As a result, in subjects with distress symptoms, evaluative/critical inner speech is a good predictor. In normal people, positive-regulatory inner speech is considered a suitable predictive regulator. These results lead us to conclude that two evaluative/critical inner speeches due to their stronger predictive ability for distress and positive-regulatory to predict normal people have stronger differential construct validity. One of the practical benefits of research in the field of psychotherapy is to identify the patient’s self-talk and work on it. The psychotherapist should focus on reducing the evaluation-critical self-talk instead of increasing the positive-regulatory self-talk. Preparing a treatment package for direct intervention on self-evaluation-critical self-talk is considered an appropriate intervention method. From the practical aspects of this research, in addition to the previous materials, the following can be mentioned, it is essential to reduce self-talk of evaluation-criticism in students during participation in exams and in athletes during participation in competitions, and reduce it in marriage counseling as well. Evaluative-critical self-talk in daily life can lead to improvement of individual efficiency and improvement of two-person communication. It seems that negative self-talk of the evaluation-critical type has an effect on psychopathology, and more research is needed to determine its specific effect on each disorder. Therefore, in the field of counseling, specific self-talk is not necessarily a predictor of a specific mental disorder.
Limitations and future research
One of the crucial limitations of this research was that it was difficult to get the satisfaction of people with disorders to respond to the questionnaires. Because negative inner speech of the evaluative/critical type seems to affect on psychopathology, further research is suggested to determine its specific effect on each disorder. Also, avoid using different types of inner speech before determining the structural validity of each one.
Ethical Considerations
Compliance with ethical guidelines
The present study is consistent with the Helsinki Declaration. Furthermore, while conducting this research, the ethical instructions of the University of Mohaghegh Ardabili have been observed. Before conducting the current work, the researchers obtained the approval of the Ethics Review Committee of University of Mohaghegh Ardabili (Code: IR.ARUMS.REC.1398.410).
Funding
This research project has been financially supported by the office of the Vice-Chancellor for Research in the University of Mohaghegh Ardabili.
Authors' contributions
Conceptualization and supervision: Hossein Ghamari Kivi; Investigation, data collection, data analysis: Hossein Ghamari Kivi, Fatemeh Jamshiddoust Miyanroudi and Effat Ghavibazu; Methodology and writing-original draft: Sara Mousavi; Review, and editing: Fatemeh Jjamshiddoust Miyanroudi and Sara Mousavi.
Conflict of interest
The authors declared no conflict of interest.
References
Abitante, G. (2019). Change your self-talk to reduce anxiety, healthy place. Retrieved from: [Link]
Alderson-Day, B., McCarthy-Jones, S., Bedford, S., Collins, H., Dunne, H., & Rooke, C., et al. (2014). Shot through with voices: Dissociation mediates the relationship between varieties of inner speech and auditory hallucination proneness. Consciousness and Cognition, 27(100), 288–296. [DOI:10.1016/j.concog.2014.05.010] [PMID]
Alderson-Day, B., Bernini, M., & Fernyhough, C. (2017). Uncharted features and dynamics of reading: Voices, characters, and crossing of experiences. Consciousness and Cognition, 49, 98-109. [DOI:10.1016/j.concog.2017.01.003] [PMID]
Alderson-Day, B., Mitrenga, K., Wilkinson, S., McCarthy-Jones, S., & Fernyhough, C. (2018). The varieties of inner speech questionnaire-revised (VISQ-R): Replicating and refining links between inner speech and psychopathology. Consciousness and Cognition, 65, 48-58. [DOI:10.1016/j.concog.2018.07.001] [PMID]
Beck, A.T. (1979). Cognitive therapy and the emotional disorders. New York: Penguin. [Link]
Carroll, A. (2022). The impact of self-talk on college students’ self-esteem, educational self-efficacy, and mood [PhD dissertation]. Dublin: National College of Ireland. [Link]
Sadri Damirchi, E., Mojarrad, A., Pireinaladin, S., & Grjibovski, A. M. (2020). The role of self-talk in predicting death anxiety, obsessive-compulsive disorder, and coping strategies in the face of coronavirus disease (COVID-19). Iranian Journal of Psychiatry, 15(3), 182-188. [DOI:10.18502/ijps.v15i3.3810] [PMID]
Davis, P. E., Meins, E., & Fernyhough, C. (2013). Individual differences in children’s private speech: The role of imaginary companions. Journal of Experimental Child Psychology, 116(3), 561-571. [DOI:10.1016/j.jecp.2013.06.010] [PMID]
de Sousa, P., Sellwood, W., Spray, A., Fernyhough, C., & Bentall, R. P. (2016). Inner speech and clarity of self-concept in thought disorder and auditory-verbal hallucinations. The Journal of nervous and mental disease, 204(12), 885–893. [DOI:10.1097/NMD.0000000000000584] [PMID]
Fritsch, J., Jekauc, D., Elsborg, P., Latinjak, A. T., Reichert, M., & Hatzigeorgiadis, A. (2022). Self-talk and emotions in tennis players during competitive matches. Journal of Applied Sport Psychology, 34(3), 518-538. [DOI:10.1080/10413200.2020.1821406]
Hatzigeorgiadis, A., Zourbanos, N., Goltsios, C., & Theodorakis, Y. (2008). Investigating the functions of self-talk: The effects of motivational self-talk on self-efficacy and performance in young tennis players. The Sport Psychologist, 22(4), 458-471. [DOI:10.1123/tsp.22.4.458]
Latinjak, A. T., Viladrich, C., Alcaraz, S., & Torregrosa, M. (2016). Spanish adaptation and validation of the Automatic Self-Talk Questionnaire for Sports. International Journal of Sport and Exercise Psychology, 14(4), 402-413. [DOI:10.1080/1612197X.2015.1055287]
Marshall, D. V., Hanrahan, S. J., & Comoutos, N. (2016). The effects of self-talk cues on the putting performance of golfers susceptible to detrimental putting performances under high pressure settings. International Journal of Golf Science, 5(2), 116–134. [DOI:10.1123/ijgs.2016-0001]
McCarthy-Jones, S., & Fernyhough, C. (2011). The varieties of inner speech: Links between quality of inner speech and psychopathological variables in a sample of young adults. Consciousness and Cognition, 20(4), 1586-1593.-[DOI:10.1016/j.concog.2011.08.005.] [PMID]
Perona-Garcelán, S., Bellido-Zanin, G., Senín-Calderón, C., López-Jiménez, A. M., & Rodríguez-Testal, J. F. (2017). Spanish adaptation of the Varieties of Inner Speech Questionnaire (VISQ). Study of the relationship between inner speech, dissociation, and hallucination proneness. Clínica y Salud, 28(2), 93-100. [DOI:10.1016/j.clysa.2017.02.001]
Shi, X., Brinthaupt, T., & McCree, M. (2017). Understanding the influence of self-critical, self-managing, and social-assessing self-talk on performance outcomes in a public speaking context. Imagination, Cognition and Personality, 36(4), 356-378. [DOI:10.1177/0276236617708740]
Shadinger, D., Katsion, J., Myllykangas, S., & Case, D. (2020). The impact of a positive, self-talk statement on public speaking anxiety. College Teaching, 68(1), 5-11. [DOI:10.1080/87567555.2019.1680522]
Terluin, B., van Marwijk, H. W., Adèr, H. J., de Vet, H. C., Penninx, B. W., & Hermens, M. L., et al. (2006). The Four-Dimensional Symptom Questionnaire (4DSQ): A validation study of a multidimensional self-report questionnaire to assess distress, depression, anxiety and somatization. BMC Psychiatry, 6, 34. [DOI:10.1186/1471-244X-6-34] [PMID]
Terluin, B., Smits, N., Brouwers, E. P., & de Vet, H. C. (2016).The Four-Dimensional Symptom Questionnaire (4DSQ) in the general population: Scale structure, reliability, measurement invariance and normative data: A cross-sectional survey. Health and Quality of Life Outcomes, 14(1), 130. [DOI:10.1186/s12955-016-0533-4] [PMID]
Hurlburt, R. T. (1997). Randomly sampling thinking in the natural environment. Journal of Consulting and Clinical Psychology, 65(6), 941–949. [DOI:10.1037/0022-006X.65.6.941] [PMID]
Van Raalte, J. L., Vincent, A., & Brewer, B. W. (2016). Self-talk: Review and sport-specific model. Psychology of Sport and Exercise, 22, 139-148.-[DOI:10.1016/J.PSYCHSPORT.2015.08.004]
Walter, N., Nikoleizig, L., & Alfermann, D. (2019). Effects of self-talk training on competitive anxiety, self-efficacy, volitional skills, and performance: An intervention study with junior sub-elite athletes. Sports, 7(6), 148. [DOI:10.3390/sports7060148]
Using inner speech is a cognitive strategy that can influence thoughts, feelings, and behaviors (Walter et al., 2019). Self-talk or internal discussions are ways in which a person communicates with himself. It is a natural cognitive process. Using inner speech may increase when faced with obstacles or challenges. People can either speak to themselves or use inner speech. This is referred to as inner speaking. Self-talk can be positive or negative. Van Raalte et al. (2016) distinguish between automatic, spontaneous, and often emotionally motivated self-talk, on the one hand, and directed and consciously motivated self-talk, on the other (Van Raalte et al., 2016). Cognitive-behavioral models emphasize the link between inner speech and the development of emotional disorders (Beck, 1972). This relationship is mainly considered from two different but complementary perspectives. One approach focuses on assessing the influence of positive and negative valence of thoughts on psychological maladjustment (Beck, 1972).
The second issue revolves around the hypothesis of cognitive content specificity and attempts to determine whether each affective disorder (i.e. depression and anxiety) is characterized by the perception of different contents (Beck, 1972). Self-talk is an internal dialogue. It is influenced by each individual’s subconscious and reveals his thoughts, beliefs, questions, and ideas. Self-talk can be negative or positive. It can be encouraging and painful. Most individuals’ self-talk depends on their personality. If people are optimistic, their self-talk may be more upbeat. The opposite is often true if people tend to be pessimistic.
Positive thinking and optimism can be effective stress management tools (Carroll, 2022). Having a more positive outlook on life can provide you with some health benefits. In the study conducted by Fritsch et al., the intensity of felt emotions and the intensity of external emotional reactions were lower when players reported only self-talk about their goals rather than spontaneous self-talk. These results support the relevance of dual-process self-talk. These results suggest that spontaneity is crucial for players to understand their emotions, but goal-directed self-talk is helpful in emotion regulation (Fritsch et al., 2022).
Research shows that how people talk to themselves during self-talk affects how they feel. For example, according to the source, using non-first-person pronouns, such as “you” and your name, instead of first-person pronouns, such as “I,” helps people adjust their thinking, their emotions, and behavior under social pressure. A 2019 study supports this theory, showing that using second-person pronouns in positive self-talk improves time and performance in endurance sports (Shadinger, 2020). Research, employing a variety of designs, has shown that self-talk strategies help athletes engage in positive self-talk and, in turn, reduce levels of competition-related anxiety (Walter et al., 2019). Additionally, a structural model that included pre-competitive anxiety provided further evidence of the association between self-talk and competitive anxiety. Finally, some methodological implications will be discussed (Marshall et al., 2016). Hatzigeorgiadis et al examined the effects of motivational self-talk on self-efficacy and performance. Research results suggest that enhancing self-efficacy may be a mechanism to explain the facilitative effects of self-talk on performance (Hatzigeorgiadis et al., 2008; Latinjak et al., 2016). Previous studies have shown its positive effects on anxiety, behavioral control under fearful conditions, and self-efficacy (Sadri Damirchi, 2020). Recently, in research conducted by Alderson-Day et al., it was discovered that inner speech can be studied using a precise method. The new scale called the varieties of inner speech questionnaire–revised (VISQ-R) includes both positive and negative self-talk. This research has shown that evaluative states are related to feelings of anxiety and depression and more evaluative states are associated with more negative self-esteem. However, motivational and regulatory self-talk is more related to the new positivity factor (Alderson-Day et al., 2017). Research in the field of sport psychology is more concerned with strong self-talk and presents aspects of self-regulatory and goal-directed behavior. However, the phenomenon of self-talk and its relationship with psychological trauma are less studied. This study shows that we can do research in this area, for example, people who are capable of positive/moderated self-talk will have a positive impact on their performance by practicing strategies instead of critical evaluation/self-talk (Davis et al., 2013). Positive/moderated self-talk has been shown to play a crucial role in creativity and visualization (Alderson et al., 2017).
According to Shi et al., reinforcing self-talk was not effective in overcoming anxiety. Speech anxiety seems to be primarily caused by frequent self-criticism (Shi, et al., 2017). McCarthy-Jones and Fernyhough showed that the factors “evaluative/motivational self-talk” and “presence of another person’s voice during self-talk” were positively related to anxiety (McCarthy & Fernyhough, 2011). The tendency toward auditory hallucinations was also positively correlated with conversational inner speech. In a recent study conducted by Alderson-Day et al. in a sample of healthy subjects, the VISQ factor “evaluative/motivational self-talk” was associated with lower self-esteem and more frequent dissociative experiences. Using structural equation modeling, they found that dissociation mediated between specific components of inner speech (evaluators and others participating in inner speech) and dispositions leading to auditory hallucinations (Alderson-Day, 2014). According to this literature review, the present study was conducted to investigate the role of self-talk styles in predicting symptoms of anxiety, depression, sleepiness, and distress in the general population in Iran. Because the signs of these problems are also present in normal people and can be easily studied.
2. Materials and Methods
Participants
The research method was a descriptive correlation type. The statistical population of the study included all 10 000 students from the University of Mohaghegh Ardabili in Iran in the academic year of 2019-2020. The sample size was calculated via Morgan’s table. To detect the optimum sample size, we considered a confidence level of 80% and a margin of error of 5%; therefore, the smallest sample size was calculated to be 378.
Inclusion criteria
The inclusion criteria included the existence of positive or negative self-talk in the subject, experiencing symptoms of anxiety, depression, physicalization, and distress, being a student in any field and level of study in the university, the consent of the person to complete the questionnaires, students at the University of Mohaghegh Ardabili interested in cooperation with more than 18 years of age.
Exclusion criteria
The exclusion criteria included the absence of clear self-talk in the subject, the existence of a specific mental disorder, and the absence of the subject’s request to implement the questionnaire.
Study procedure
To implement the study, all students were referred to the Sepand Counseling Center and interviewed at the Counseling Center of the University of Mohaghegh Ardabili in the first six months of 2019-2020. The population of this study was all those who were referred to the Sepand Counseling Center and students who were willing to complete the questionnaires. Additionally, all inclusion and exclusion criteria were considered in the early screening stages, and no sample loss was observed after the final selection. Furthermore, students completed the VISQ and the four-dimensional symptom questionnaire (4DSQ), including four symptom scales. Most sample participants were at the University of Mohaghegh Ardabili. Finally, a total of 372 of the 378 respondents completed the questionnaires, while 5 questionnaires were discarded due to incompletion. The researchers have followed all the current Iranian laws and regulations. In this study, ethical issues, such as informed consent, privacy, confidentiality, and anonymity were considered. According to the regulation of compliance with ethical standards, the consent form for free participation in the research was completed by all examinees.
Research tools
Varieties of inner speech questionnaire (VISQ)
Varieties of inner speech questionnaire–revised (VISQ-R) phenomenological properties of inner speech were assessed using the 35-item VISQ-R (Hurlburt, 1997). In addition to the original 18 items on dialogue, evaluation, succinctness, and the presence of others in self-talk, the expanded version includes new items on literal and metaphorical use of language, and how to define the speaker’s position and address as well as regulations on language usage, different moods, and positive moods /regulations. Responses were made on a seven-item frequency scale, in which respondents rated the frequency of experiencing the inner speech experience from “never” (1) to “always” (7). Exploratory factor analysis indicated a five-factor structure consisting of the three previous subscales (dialogue, succinctness, and others talking to themselves), an evaluative/critical factor, a positive/active factor, and a new regulation (Alderson-Day et al., 2018). The result of calculating Cronbach’s α coefficient in this study is 0.899.
The four-dimensional symptom questionnaire (4DSQ)
The four-dimensional symptom questionnaire (4DSQ) includes four symptom scales, distress (16 items), depression (6 items), anxiety (12 items), and lethargy (16 items) (Terluin, 2006). 4DSQ uses a 7-day time reference. Questions are answered on a 5-point frequency scale, from “not at all” to “very often or constantly.” To calculate the total score, responses were coded on a 3-point scale: “Never” (0 points), “sometimes” (1 point), “often,” “often,” and “very often or continuously” (2 points). By grouping the reaction categories “often,” “regularly,” and “very often or continuously,” we placed more weight on the number of symptoms experienced than on their perceived frequency. The 4DSQ is a self-report questionnaire consisting of 50 items divided into four scales. These items are formulated as questions similar to those that may be asked in daily primary care practice. The distress scale contains 16 items and has a score range of 0–32, the depression scale contains 6 items and has a range of 0–12, the anxiety scale contains 12 items and has a range of 0–24, and the somatization scale contains 16 items and has a range of 0–32 (Terluin et al., 2016). This questionnaire is based on the symptoms of mental patients. The internal correlation for the four scales is from 0.35 to 0.71. The result of calculating Cronbach’s α coefficient in the current study is equal to 0.95.
Data analysis
The research method is descriptive and correlational, using the statistical method of multivariate analysis of variance. Data were analyzed using-SPSS software, version 23. Descriptive statistics (Mean±SD, percentage, and frequency) and inferential statistics (Pearson correlation method) were used. Additionally, in this study, stepwise multivariate regression analysis to determine depression, including self-talk by others, explained 18% of the variance in depression.
3. Results
The demographic characteristics of the participants showed that 0.8% of the participants were diploma students, 83.1% were undergraduate students, 14% were postgraduate students, and 2.2% were doctoral students. The marital status of the subjects participating in the project was as follows, out of 212 women (57%) and 160 men (43%), 270 people (72.6%) were single and 102 people (27.4%) were married. Table 1 presents a positive correlation between types of inner speech with various symptoms of disorders, and as expected only a very slight and sometimes negative correlation between positive-regulatory inner speech and other disorders. Therefore, the highest correlated of correlation is between others’ inner speech and anxiety. Stepwise regression analysis was used to investigate the following questions.
In stepwise multivariate regression analysis for anxiety, inner speech (others) was entered first, which explained 20% of anxiety variance (F(1, 370)=45.95, P<0.001). After that, inner speech (positive-regulatory) was entered, which explained another 2% (F(1, 369)=10.98, P<0.001). Finally, inner speech (evaluation-critical) was entered, which explained the remaining 2% (F(1, 368)=41.12, P<0.001). Higher anxiety was correlated with inner speech (higher others, lower positive-regulatory, and higher evaluative/critical inner speech). In the stepwise multivariate regression analysis for depression, inner speech (others) was entered first, which explained 17% of the variance of depression (F(1, 370)=60.76, P<0.001). After that, inner speech (positive-regulatory) was entered, which explained another 2% (F(1, 369)=51.9, P<0.002). Finally, the inner speech (evaluation-critical) was included, which explained the remaining 5% (F(1, 368)=55.24, P<0.001). Higher depression was correlated with inner speech (others and higher critical evaluation and lower positive-regulatory). In the stepwise multivariate regression analysis for somatization, inner speech (others) were entered first, which explained 16% of the variance of somatization (F(1, 370)=90.72, P<0.001). After that, inner speech (dialogic) was entered, which explained another 1% (F(1, 369)=34.7, P<0.007). Finally, inner speech (evaluation-critical) was entered, which explained the remaining 9% (F(1, 368)=4.10, P<0.04). Higher somatization was correlated with higher inner speech (others, conversational, and evaluative-critical). In the stepwise multivariate regression analysis for distress, first, the self-evaluation-critical inner speech was entered, which explained 21% of the variance of distress (F(1, 370)=48.101, P<0.001). After that, inner speech (others) was entered, which explained another 5% (F(1, 369)=27.78, P<0.001). Finally, inner speech (positive-regulatory) was entered, which explained the remaining 3% (F(1, 368)=20.20, P<0.001). Higher distress was correlated with inner speech (higher evaluative-critical and others and lower positive-regulatory, Table 1).
According to Table 2, to more accurately determine the components of inner speech in people with symptoms of anxiety, depression, somatization, and distress, by standardizing the scores and converting them to Z scores, scores of 0-1 were selected, and typical people had disorders.
In Table 3, according to the stepwise multivariable regression analysis of anxiety, high anxiety was correlated with the inner speech of others, evaluative/critical (low), and dialectical. In the stepwise multivariable regression analysis for depression, the inner speech of others was included, which explained 18% of the variance of depression (P<0.001). Higher depression was correlated with others’ inner speech and stepwise multivariate regression analysis for somatization, condensed inner speech explained 22% of the variance of somatization (P<0.001). Higher somatization was correlated with lower condensed inner speech. In the stepwise multivariate regression analysis for distress, dialogic inner speech explained 14% of the variance of distress (P<0.04). Higher distress was correlated with dialogic inner speech.
4. Discussion
The present study was conducted to study and survey the role of types of inner speech in predicting symptoms of anxiety, depression, somatization, and distress in the normal population in Iran. According to the results of the current study, in people with symptoms of anxiety, depression, and somatization disorders, the inner speech of others was a stronger predictor compared to other types of inner speech. Talking to others means hearing the other person’s voice. In other words, a person says something to himself in another person’s voice. This is consistent with the study results of de Sousa et al., 2016, Perona et al., 2017, and Abitante, 2022. However, in the study conducted by de Sousa et al., condensed inner speech and talking to others were related to psychological trauma. However, the condensed inner speech was not decisive in any of the people with symptoms of anxiety, depression, and somatization disorders in the current study (de Sousa et al., 2016).
On the other hand, in subjects with distress symptoms, evaluative/critical inner speech was a good predictor. This result suggests that evaluative/critical inner speech primes individuals’ susceptibility to general distress as a common indicator of psychological distress. One thing to note in the current study is that positive-regulatory inner speech is significantly negative in people with symptoms of anxiety, depression, and distress (Perona et al., 2017; Abitante, 2022). Patients had higher scores in condensed inner speech than others, but not in conversational and evaluation inner speech. In the study conducted by McCarthy-Jones & Fernyhough (2011), inner speech was more prevalent among students with anxiety symptoms. McCarthy-Jones and Fernyhough believe that no serious field studies on inner speech were found. However, the study conducted by McCarthy-Jones and Fernyhough was designed to evaluate the phenomenological properties of inner speech types in conversational dimensions, the quality of density/expansion, the level of evaluation/arousal, and the extent to which inner speech integrates the voices of others (McCarthy & Fernyhough, 2011). In addition, the relationship between some types of disorders, such as anxiety and depression, and the tendency to auditory and visual hallucinations with inner speech was investigated. The results showed a positive correlation between anxiety and evaluative/critical inner speech and the presence of other people’s voices in inner speech (Perona et al., 2017).
5. Conclusion
As a result, in subjects with distress symptoms, evaluative/critical inner speech is a good predictor. In normal people, positive-regulatory inner speech is considered a suitable predictive regulator. These results lead us to conclude that two evaluative/critical inner speeches due to their stronger predictive ability for distress and positive-regulatory to predict normal people have stronger differential construct validity. One of the practical benefits of research in the field of psychotherapy is to identify the patient’s self-talk and work on it. The psychotherapist should focus on reducing the evaluation-critical self-talk instead of increasing the positive-regulatory self-talk. Preparing a treatment package for direct intervention on self-evaluation-critical self-talk is considered an appropriate intervention method. From the practical aspects of this research, in addition to the previous materials, the following can be mentioned, it is essential to reduce self-talk of evaluation-criticism in students during participation in exams and in athletes during participation in competitions, and reduce it in marriage counseling as well. Evaluative-critical self-talk in daily life can lead to improvement of individual efficiency and improvement of two-person communication. It seems that negative self-talk of the evaluation-critical type has an effect on psychopathology, and more research is needed to determine its specific effect on each disorder. Therefore, in the field of counseling, specific self-talk is not necessarily a predictor of a specific mental disorder.
Limitations and future research
One of the crucial limitations of this research was that it was difficult to get the satisfaction of people with disorders to respond to the questionnaires. Because negative inner speech of the evaluative/critical type seems to affect on psychopathology, further research is suggested to determine its specific effect on each disorder. Also, avoid using different types of inner speech before determining the structural validity of each one.
Ethical Considerations
Compliance with ethical guidelines
The present study is consistent with the Helsinki Declaration. Furthermore, while conducting this research, the ethical instructions of the University of Mohaghegh Ardabili have been observed. Before conducting the current work, the researchers obtained the approval of the Ethics Review Committee of University of Mohaghegh Ardabili (Code: IR.ARUMS.REC.1398.410).
Funding
This research project has been financially supported by the office of the Vice-Chancellor for Research in the University of Mohaghegh Ardabili.
Authors' contributions
Conceptualization and supervision: Hossein Ghamari Kivi; Investigation, data collection, data analysis: Hossein Ghamari Kivi, Fatemeh Jamshiddoust Miyanroudi and Effat Ghavibazu; Methodology and writing-original draft: Sara Mousavi; Review, and editing: Fatemeh Jjamshiddoust Miyanroudi and Sara Mousavi.
Conflict of interest
The authors declared no conflict of interest.
References
Abitante, G. (2019). Change your self-talk to reduce anxiety, healthy place. Retrieved from: [Link]
Alderson-Day, B., McCarthy-Jones, S., Bedford, S., Collins, H., Dunne, H., & Rooke, C., et al. (2014). Shot through with voices: Dissociation mediates the relationship between varieties of inner speech and auditory hallucination proneness. Consciousness and Cognition, 27(100), 288–296. [DOI:10.1016/j.concog.2014.05.010] [PMID]
Alderson-Day, B., Bernini, M., & Fernyhough, C. (2017). Uncharted features and dynamics of reading: Voices, characters, and crossing of experiences. Consciousness and Cognition, 49, 98-109. [DOI:10.1016/j.concog.2017.01.003] [PMID]
Alderson-Day, B., Mitrenga, K., Wilkinson, S., McCarthy-Jones, S., & Fernyhough, C. (2018). The varieties of inner speech questionnaire-revised (VISQ-R): Replicating and refining links between inner speech and psychopathology. Consciousness and Cognition, 65, 48-58. [DOI:10.1016/j.concog.2018.07.001] [PMID]
Beck, A.T. (1979). Cognitive therapy and the emotional disorders. New York: Penguin. [Link]
Carroll, A. (2022). The impact of self-talk on college students’ self-esteem, educational self-efficacy, and mood [PhD dissertation]. Dublin: National College of Ireland. [Link]
Sadri Damirchi, E., Mojarrad, A., Pireinaladin, S., & Grjibovski, A. M. (2020). The role of self-talk in predicting death anxiety, obsessive-compulsive disorder, and coping strategies in the face of coronavirus disease (COVID-19). Iranian Journal of Psychiatry, 15(3), 182-188. [DOI:10.18502/ijps.v15i3.3810] [PMID]
Davis, P. E., Meins, E., & Fernyhough, C. (2013). Individual differences in children’s private speech: The role of imaginary companions. Journal of Experimental Child Psychology, 116(3), 561-571. [DOI:10.1016/j.jecp.2013.06.010] [PMID]
de Sousa, P., Sellwood, W., Spray, A., Fernyhough, C., & Bentall, R. P. (2016). Inner speech and clarity of self-concept in thought disorder and auditory-verbal hallucinations. The Journal of nervous and mental disease, 204(12), 885–893. [DOI:10.1097/NMD.0000000000000584] [PMID]
Fritsch, J., Jekauc, D., Elsborg, P., Latinjak, A. T., Reichert, M., & Hatzigeorgiadis, A. (2022). Self-talk and emotions in tennis players during competitive matches. Journal of Applied Sport Psychology, 34(3), 518-538. [DOI:10.1080/10413200.2020.1821406]
Hatzigeorgiadis, A., Zourbanos, N., Goltsios, C., & Theodorakis, Y. (2008). Investigating the functions of self-talk: The effects of motivational self-talk on self-efficacy and performance in young tennis players. The Sport Psychologist, 22(4), 458-471. [DOI:10.1123/tsp.22.4.458]
Latinjak, A. T., Viladrich, C., Alcaraz, S., & Torregrosa, M. (2016). Spanish adaptation and validation of the Automatic Self-Talk Questionnaire for Sports. International Journal of Sport and Exercise Psychology, 14(4), 402-413. [DOI:10.1080/1612197X.2015.1055287]
Marshall, D. V., Hanrahan, S. J., & Comoutos, N. (2016). The effects of self-talk cues on the putting performance of golfers susceptible to detrimental putting performances under high pressure settings. International Journal of Golf Science, 5(2), 116–134. [DOI:10.1123/ijgs.2016-0001]
McCarthy-Jones, S., & Fernyhough, C. (2011). The varieties of inner speech: Links between quality of inner speech and psychopathological variables in a sample of young adults. Consciousness and Cognition, 20(4), 1586-1593.-[DOI:10.1016/j.concog.2011.08.005.] [PMID]
Perona-Garcelán, S., Bellido-Zanin, G., Senín-Calderón, C., López-Jiménez, A. M., & Rodríguez-Testal, J. F. (2017). Spanish adaptation of the Varieties of Inner Speech Questionnaire (VISQ). Study of the relationship between inner speech, dissociation, and hallucination proneness. Clínica y Salud, 28(2), 93-100. [DOI:10.1016/j.clysa.2017.02.001]
Shi, X., Brinthaupt, T., & McCree, M. (2017). Understanding the influence of self-critical, self-managing, and social-assessing self-talk on performance outcomes in a public speaking context. Imagination, Cognition and Personality, 36(4), 356-378. [DOI:10.1177/0276236617708740]
Shadinger, D., Katsion, J., Myllykangas, S., & Case, D. (2020). The impact of a positive, self-talk statement on public speaking anxiety. College Teaching, 68(1), 5-11. [DOI:10.1080/87567555.2019.1680522]
Terluin, B., van Marwijk, H. W., Adèr, H. J., de Vet, H. C., Penninx, B. W., & Hermens, M. L., et al. (2006). The Four-Dimensional Symptom Questionnaire (4DSQ): A validation study of a multidimensional self-report questionnaire to assess distress, depression, anxiety and somatization. BMC Psychiatry, 6, 34. [DOI:10.1186/1471-244X-6-34] [PMID]
Terluin, B., Smits, N., Brouwers, E. P., & de Vet, H. C. (2016).The Four-Dimensional Symptom Questionnaire (4DSQ) in the general population: Scale structure, reliability, measurement invariance and normative data: A cross-sectional survey. Health and Quality of Life Outcomes, 14(1), 130. [DOI:10.1186/s12955-016-0533-4] [PMID]
Hurlburt, R. T. (1997). Randomly sampling thinking in the natural environment. Journal of Consulting and Clinical Psychology, 65(6), 941–949. [DOI:10.1037/0022-006X.65.6.941] [PMID]
Van Raalte, J. L., Vincent, A., & Brewer, B. W. (2016). Self-talk: Review and sport-specific model. Psychology of Sport and Exercise, 22, 139-148.-[DOI:10.1016/J.PSYCHSPORT.2015.08.004]
Walter, N., Nikoleizig, L., & Alfermann, D. (2019). Effects of self-talk training on competitive anxiety, self-efficacy, volitional skills, and performance: An intervention study with junior sub-elite athletes. Sports, 7(6), 148. [DOI:10.3390/sports7060148]
Type of Study: Original Research Article |
Subject:
Rehabilitation
Received: 2023/02/19 | Accepted: 2023/06/13 | Published: 2023/10/28
Received: 2023/02/19 | Accepted: 2023/06/13 | Published: 2023/10/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
