

Volume 7, Issue 1 (Winter 2019)
PCP 2019, 7(1): 11-20 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khademi M, Ayatmehr F, Khosravan Mehr N, Razjooyan K, Davari Ashtiani R, Arabgol F. Evaluation of the Effects of Positive Parenting Program on Symptoms of Preschool Children With Attention Deficit Hyperactivity Disorder. PCP 2019; 7 (1) :11-20
URL: http://jpcp.uswr.ac.ir/article-1-512-en.html
URL: http://jpcp.uswr.ac.ir/article-1-512-en.html
Mojgan Khademi1 

 , Fatemeh Ayatmehr2 , Najmeh Khosravan Mehr *3 , Katayoon Razjooyan1 , Rozita Davari Ashtiani1 , Fariba Arabgol1
, Fatemeh Ayatmehr2 , Najmeh Khosravan Mehr *3 , Katayoon Razjooyan1 , Rozita Davari Ashtiani1 , Fariba Arabgol1
, Fatemeh Ayatmehr2 , Najmeh Khosravan Mehr *3 , Katayoon Razjooyan1 , Rozita Davari Ashtiani1 , Fariba Arabgol1
1- Behavioral Science Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,nkhosrovan@yahoo.com
2- Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 647 kb]
(4323 Downloads)
| Abstract (HTML) (8668 Views)



In Moharreri et al. (2008) study, the parents participating in the Triple-P group displayed significant reduction in the mean number of problems identified between parents on child rearing. This reduction was significant in the over-reactivity, laxness, and verbosity of the studied parents (Moharreri et al., 2008). Such results were similar to Ralph and Sanders study results in terms of reducing the parents’ disagreement with their partner over parenting issues and improving their style (Ralph & Sanders, 2003). Meanwhile, after intervention of Stepping Stones Triple-P among families with children with autism spectrum disorder aged between 2 and 9 years, Whittingham et al. (2008) demonstrated significant improvements in parental reports of child behavior and parenting styles with the treatment effects for the child behavior, parental over-reactivity, and parental verbosity being maintained at 6 months follow-up (Whittingham et al. 2008).
One of the important findings of this study was the impact of positive parenting program on ADHD symptoms in preschool children suffering from this disorder. By reviewing the obtained results, we concluded that training parents with Triple-P methods could reduce the ADHD symptoms in their children. These findings are consistent with the findings of previous studies. The results of Moharari study, conducted by standard level of Triple-P among elementary school students, are in line with the results of the present study among preschoolers. Moharreri et al. (2008) concluded that by implementing positive parenting program, the ADHD-related symptoms would be improved (Moharreri et al., 2008).
A finding of Daley study also suggests a reduction of hyperactivity symptoms using this program (Daley and et al., 2009). In our study, along with reducing overall disorder symptoms, the Triple-P method was effective in reducing Conner’s three subscales and could reduce the symptoms of ADHD. This study is the first group research on Triple-P in Iranian parents with ADHD children in preschool age. It seems that the Triple-P is compatible with Iranian culture.
Applying Triple-P on Iranian families brings considerable comfort in lowering the risk of dealing with advanced and prolonged oppositional/antisocial aspects of ADHD. Furthermore, the results of the present study indicate that Triple-P can also reduce parents’ depression and stress. This can be the result of parents’ empowerment feeling in parenting. As mentioned earlier, Ireland et al. (2003) reported the positive feeling of parents in parenting that lasted after 3 months (Ireland et al., 2003). While in the present study, no effect was observed on parents’ anxiety after evaluation of the results. In contrast, Moharreri et al. (2008) reported a significant reduction in the parents’ level of depression, anxiety, and stress scores (Moharreri et al., 2008).
The discrepancy in the results of the present research and Moharrari study could be due to study subjects of Moharrari who were children aged 6-12 years, while our study was conducted on preschoolers. Besides, parents are worried that their children might experience the relapse symptoms when entering school and facing harder homework. This can be a factor of preserving their anxiety in high level. Likewise, Leung et al. (2006) following intervention on their study participants, reported significantly lower levels of child behavior problems, lower parenting stress, lower depression, anxiety and stress scores, and higher parenting sense of competence.
In this study, positive parenting training had a positive and significant impact on parents’ problem checklist and reduced their problems. In a study conducted by Tehranidoost et al. (2009) performing Triple-P improved parents’ problems and parenting method Tehranidoost et al., 2009). Another finding of our research points to the parenting improvement, which is consistent with other studies. Sanders (1999) performed an advanced form of Triple-P on some families having ADHD children aged 5 to 9 years and found a significant decrease in destructive behavior and improvement in parenting patterns. Besides, the feeling of having better positive-parenting ability in child rearing was reported in comparison to controls and the positive impacts were persistent at least for 3 months.
In Moharreri et al. (2008) study, Triple-P was effective on the reduction of dysfunctional parenting style, as the post-intervention compared the subscale scores and the total score of parenting scale in the subject group with those in the control group (Moharreri et al., 2008). Dean et al. (2003) conducted a research on positive parenting program in a sample group of the society and reported that the program could increase parents’ knowledge about parenting methods.
Considering the difficulties in the rearing of ADHD children compared to non-ADHD children, the affected families need parenting patience, skills, and abilities, and as much as these families acquire parenting skills and receive proper education, their abilities will be increased in controlling the behavior of their children. Positive parenting program for parents of ADHD children will improve their parenting skills and reduce problems related to parenting such as depression and frustration. These methods also reduce behavioral problems of children and increase their abilities.
One of our study limitations was the absence of fathers in Triple-P sessions and the mothers were the only receivers of the training. The other limitation of the present study was comorbid disorders, which overlooked in the studied children. Therefore, we suggest to do further work on these topics in the future similar studies. Triple-P is defined as a brief and time-saving program with significant impact on therapist’s skills, self-confidence and satisfaction of advising parents of children with behavioral problems. Thus, we suggest its use for public health and in line with preventing psychopathology in children. Future work can no doubt lead us to other vast applications of Triple-P.
Ethical Considerations
Compliance with ethical guidelines
All participants signed written informed consent and could leave the study whenever they wished. The participants’ personal information was kept confidential. The routine therapy of children was continued; however, if drug adjustment were required, the medication would be changed but the participant would be excluded from the study.
Funding
This study was supported by Behavioral Sciences Research Centre of Shahid Beheshti University of Medical Sciences.
Authors contributions
Conceptualization: Mojgan Khademi; Methodology: Katayoon Razjooyan, Najmeh Khosrovan Mehr; Investigation: Rozita Davari Ashtiani; Writing–original draft: Mojgan Khademi, Najmeh Khosrovan Mehr; Writing– review & editing: Fatemeh Ayatmehr. Najmeh Khosrovan Mehr; Resources: Mojgan Khademi, Najmeh Khosrovan Mehr; and Supervision: Fariba Arabgol.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
We wish to express our sincere gratitude to the internal manager of Behavioral Sciences Research Centre of Shahid Beheshti University of Medical Sciences for sharing expertise, and sincere and valuable guidance, financial support and encouragement.
References
Full-Text: (2475 Views)
1. Introduction
Attention-Deficit Hyperactivity Disorder (ADHD) is one of the most common psychiatric disorders in children and adolescents and if left untreated, it could result in numerous problems for the child and his or her family (Sonuga-Barke et al., 2001). Treatment of ADHD at preschool age is very important, otherwise it can cause a lot of disabilities for the child and the family at this age and later in life (Sonuga-Barke et al., 2001).
Since the last decade, ADHD diagnosis has been increased at preschool age, with more demand for non-pharmacological intervention at this age. One reason is the lack of enough study on the efficacy and adverse effects of drugs in children at preschool age. In addition, previous research indicates that Ritalin is not so effective on school-aged children and has more side effects (Greenhill et al., 2006). If non-pharmacological therapies start at lower ages, before the emergence of other disorders and the occurrence of educational and behavioral problems or loss of self-confidence, treatment can be simpler and more effective (Daley & Thompson, 2007).
Training parents about the methods of behavioral management has been suggested as the first treatment of reducing the ADHD symptoms at preschool age (Conner, 1997). Besides, many studies support the effectiveness of this method (Jones et al., 2007; Chronis, Jones, & Raggi, 2006). Parenting practices are in one way different from parenting style as the former focuses on specific parenting behaviors related to nutrition and physical activity while the latter emphasizes on parent-child interactions in different situations (Darling & Steinberg, 1993; Sleddens, Gerards, Thijs, Vries, & Kremers, 2011). In addition, parenting interventions seem to have positive long-term effects on a range of other problems at young age, namely mental, emotional and behavioral disorders; it also affects successful developmental competence (Sandler, Schoenfelder, Wolchik & Mackinnon, 2011).
In particular, positive parenting has been suggested as a critical external factor with strong influences on child’s follow-up issues. In particular, to be a supportive parent since the very young ages of the child, has been proven to positively affect child’s development in cognitive, behavioral, and psychological aspects (Beckwith, Rodning, & Cohen, 1992; Eshel, Daelmans, deMello, & Martines, 2006; Landry, Smith, Swank, & Guttentag, 2008).
Parenting is especially important because of the familial nature of the ADHD disorder. In addition much evidence indicates that such behaviors and ADHD symptoms will appear during child development or even consolidate with comorbid psychopathologies, and so on (Johnston, Mash, Miller, & Ninowski, 2010). In this regard, three interventions are considered as the most effective child-rearing interventions that can reduce the ADHD symptoms in children at preschool age; one of them is Positive Parenting Program (Triple-P) which consists of different training levels. Triple-P is a multi-level parenting and family support strategy developed by the University of Queensland in Brisbane, Australia.
It uses social learning principles and adopts a supportive system-contextual or ecological perspective in parents. The program is widely supported at international level and several related programs have been developed so far to address parents’ special needs (West & Sander, 2012). The standard level of Triple-P method is suitable for training the normal children. This level was taught to a group of child and adolescent’s psychiatrists in Iran and its effectiveness was confirmed on mothers with normal and ADHD children at preschool age.
Considering the importance of non-pharmacological treatment of ADHD at preschool age, evaluation of this kind of treatment in this age group in Iran is essential. The innovation of this research is the use of standard level Triple-P to reduce the symptoms of ADHD in preschoolers. This level is not specific for children with ADHD, but according to our study, it can be useful in reducing symptoms of this disorder. Paying attention to children’s age in our research is also of great importance. The study children were of preschool age and for the first time in Iran, the standard level Triple-P was conducted for ADHD children in this age group. In addition, the number of the participants was higher than other similar research studies. Therefore, we evaluated the impact of implementing Triple-P on preschool aged children suffering from ADHD.
There are several studies in the literature in this topic. Dean et al. (2003) examined Triple-P in a group of people and found that this program could promote parents’ knowledge about child rearing and improve children’s behavior and these effects were persistent for 12 months (Dean, Myors, & Evans, 2003). Besides, Leung, Sanders, Francis, & Joseph, (2006) examined the effectiveness of the Triple-P in a government child-health service context with 661 Chinese parents of preschool and primary school-aged children in Hong Kong.
They showed significant decrease in disruptive child’s behaviors, levels of parenting stress, general stress and anxiety and an increase in parenting sense of competence as well as lower levels of family earnings in the relative social and professional position of the newly immigrant family, and greater pre-intervention levels of parenting stress (Leung et al., 2006). Furthermore, (McTaggart & Sanders, 2007) reported that parents who completed the Triple-P are equally likely to succeed in changing their parenting practices. Their findings suggest the robustness of intervention effects across a diverse range of parents (McTaggart & Sanders, 2007).
The evidence for the efficacy of Triple-P is supported by a series of controlled trials in Australia, although similar trials are in progress in several other countries in Europe and North America (Sanders, 1999). A series of studies have shown that Triple-P is effective in a number of delivery formats (group, individual, phone-assisted and self-directed) with significant reductions in both observed and parent-reported disruptive behaviors, increased parental self-efficacy, reduced levels of dysfunctional parenting (laxness, over-reactivity and verbosity), parental anger, depression, stress, marital conflict and work stress (Ireland, Sanders, & Markie-Dadds, 2003).
Leung et al. (2006) also evaluated Tripe-P on Chinese parents of children with early onset conduct-related problems in Hong Kong. They showed significantly lower levels of child behavioral problems, less parenting styles impairment, and higher parental sense of competence (Leung, Sanders, Leung, Mak, & Lau, 2003). Meanwhile, Whittingham, Sofronoff, Sheffield, & Sanders, (2008) studied 59 families with children suffering from autism spectrum disorders aged between 2 and 9 years.
Using Stepping Stones Triple-P, the researchers reported that the parents’ expectations were better met, their children exhibited acceptable behavior, and their relationship with their partners got better (Whittingham et al., 2008). However, Danforth, Harvey, Ulaszek, and Mckee (2006) Evaluated the effects of group parent training on parent performance, and on the response of 45 children with ADHD and defiant aggressive behavior and reported reduced children’s hyperactive, defiant, and harmful behavior, enhanced parenting style, and minimized parents’ stress (Danforth et al., 2006). In a case study conducted by Daley, Jones, Hutchings and Thompson (2009). three non-pharmacological treatments (one of them was positive parenting) were evaluated in order to reduce ADHD symptoms among preschool aged children (Daley et al., 2009).
In addition, Tehranidoost, Shahrivar, MahmoudiGharaie, and Alaghband-Rad (2009) conducted a study on 120 mothers in Tehran. The results revealed that performing Triple-P child-rearing program improved children’s behavior, parents’ problems and child rearing methods (Tehranidoost et al., 2009). Moreover, Moharreri, Shahrivar, Tehranidoost, and MahmoudiGhara (2008) performed a study on 30 parents with ADHD school-aged children and compared them to controls. They performed standard Triple-P method and observed that ADHD symptoms improved along with the child-rearing scales (Moharreri et al., 2008). After an initial evaluation of the group teen Triple-P program for parents of teenagers, Ralph and Sanders reported significant reductions in conflicts with their young children and the measures of negligent, strong reactions and lack of communication with parents about parenting issues (Ralph & Sanders, 2003).
Because the medication efficacy has been less studied at preschool age or there is controversy among many experts in this regard, alternative methods, including Triple-P can be of great help for managing this disorder at this age. Thus, this research aimed to study the effects of Triple-P on ADHD symptoms of preschool children.
2. Methods
This study is a randomized controlled trial. The study population consisted of parents of ADHD children referred to Imam Hossain Psychiatry Clinic in Tehran, in 2010 and 2011. A total number of 110 parents with preschool-aged children diagnosed with ADHD were recruited from Child Psychiatry Clinic of Imam Hossain Hospital with convenience sampling method. The parents were being interviewed before participating in the study to check the inclusion criteria.
The inclusion criteria were having passed at least 5th grade education, having a preschool child with ADHD diagnosis according to child psychiatrist interview, lacking untreated major psychiatric problems such as psychotic disorders or bipolar disorders (Parents’ psychological health were examined by psychiatrists in Imam Hossain Hospital based on DSM-IV).
The study children should be under stable dose of medication for at least one month. If there were a need for changing medication or its amount, then their mothers would be excluded from the study. In addition, if parents missed more than 3 training sessions they were also excluded. All participants signed a written informed consent. Then, eligible individuals were randomly assigned into control and treatment (subject) group.
After all parents completed a demographic form and pre-test questionnaire, a psychoeducational session about ADHD was held for all parents. Then, the subject group attended in a Triple-P program (Standard level). The subject parents participated in 2-hour sessions per week for 4 weeks followed by 4 phone-based sessions. Each training group included 12 to 15 participants. The first 4 sessions were training sessions. In the next 4 sessions, family problems during practicing and conducting methods in house were addressed. The experienced psychiatrists conducted the course. The experts from the University of Queensland, Australia have taught The standard level of Triple-P to some Iranian child and adolescent psychiatrists and the Iran Ministry of Health confirmed its effectiveness in a large group of mothers with normal children.
Parents in the control group received conventional managements based on routine clinic program, after receiving a psychoeducational session about ADHD. At the end of 8 weeks, the subject and control groups completed the same questionnaires. During the study period, some participants of the subject group were excluded because of more than three sessions absence. In addition, some participants were excluded from the control group due to lack of cooperation in filling the final questionnaires or the need to change their medication during the study. Finally, 94 participants (53 in the subject group and 41 in the control group) finished the study. The obtained data were presented as Mean±SD. A series of Analysis of Covariance (ANCOVA) were performed to compare the groups before and after the intervention. All of these analyses were done in SPSS for Windows (version 19; SPSS Inc., Chicago, IL, USA).
The Family Background Questionnaire provides reliable family history information. Reliability and validity analyses suggest that it is a useful screening instrument for obtaining family history information (Melchert & Kalemeer, 2009). A brief version of this instrument assesses parental responsiveness, child maltreatment, and parental substance abuse. This questionnaire contains essential biographical information, including 1. Name, age, gender and date of birth of the child; 2. Parents’ marital status and relationship with the child; 3. Their current employment status; and 4. Educational background and total family income (Moharreri et al., 2008). The scale has good test-retest reliability and construct validity and internal consistency obtained by Cronbach α as 0.79 to 0.95 (Melchert & Kalemeer, 2009).
The Conner’s ADHD Rating Scale, Parents’ Form screens and evaluates treatment results. This 27-item test is an abbreviated and revised form of an unabridged 93-item version, and parents should respond to it before and after the program. The scale is useful for children aged 3-17 years old and its diagnostic validity and reliability are consistent with DSM-IV criteria.(Conner, 1997). Its subscales include oppositionality, cognitive problems, inattention, hyperactivity, and ADHD index. Its internal consistency is around 0.75 to 0.90 and the test-retest reliability with 8 weeks interval is 0.6 to 0.9. Construction validity of this scale is obtained by factor analysis (ZargariNejad & YekkeYazdandoost, 2007).
The 30-item Parenting Scale measures the dysfunctional discipline style in parents. It yields a total score based on three factors: laxness (permissive discipline); over-reactivity (authoritarian discipline, displaying anger, and irritability); and verbosity (overly long reprimands or reliance on talking) as measured on a 7-point scale. The scale has acceptable internal consistency for the total score (0.87), laxness (0.87), over-reactivity (0.83) and verbosity (0.82) subscales. This scale can differentiate between parents of clinic and non-clinic children. It correlates with self-report measures of child’s behavior, marital discord, and depressive symptoms, as well as observational measures of dysfunctional discipline and child behavior (Arnold, O’leary, Wolff, & Acker, 1993).
The Parent Problem Checklist has 16 items that measures inter-parental conflict on child rearing. The Parent Problem Checklist (PPC) has high internal consistency (α=0.92). It has also high test-retest reliability (r=.90) (Dadds & Powll, 1991). The 42-item Depression, Anxiety Stress Scale measures parental levels of depression and anxiety. The scale has high reliability for the depression (0.91), anxiety (0.81), and stress (0.89) subscales and good discriminative and concurrent validity (Moharreri et al., 2008).
Parenting Sense of Competency Scale was made by Giboud-Wallston and Wandesman in 1978. A 16-item version of this questionnaire, “being a parent scale”, was used to assess parents’ view of their competence as parents’ satisfaction with their parenting role and feeling of efficacy as a parent. The total score shows a good internal consistency (α=0.79) (Bor, Saners, & Marki-Dadds, 2002). Other positive parenting studies have already used all above-mentioned questionnaires and Iranian researchers approved their validity.
3. Results
In the present study, 110 parents participated, but 93 completed the study. Data analysis was performed by analyses of covariance. Result showed that the Mean±SD ages of the children in the treatment and control group were 4.2±1.09 and 3.9±1.23 years, respectively. Data analysis showed no significant difference between two groups (t=0.92, df=82, P=0.35). Table 1 presents the other descriptive statistics of study participants.
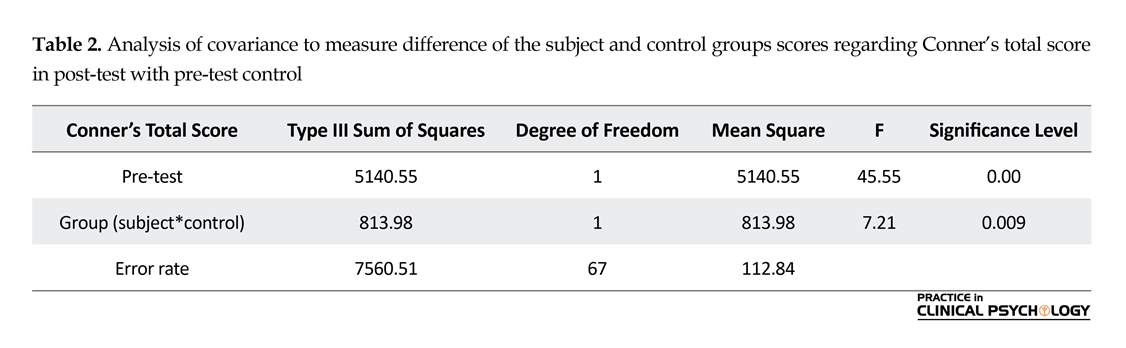
Data analysis revealed no significant difference between two groups regarding sex of children (χ2=0.03, df=1, P=0.83), mothers’ education (χ2=4.42, df=5, P=0.53) and mothers’ employment (χ2=2.98, df=1, P=0.08). According to Table 2, ADHD mean of the groups indicated that with 99% confidence, Triple-P has a positive and significant impact on ADHD. Thus, this program could reduce the symptoms of ADHD in the subject group (F=7.21; P<0.01).
Attention-Deficit Hyperactivity Disorder (ADHD) is one of the most common psychiatric disorders in children and adolescents and if left untreated, it could result in numerous problems for the child and his or her family (Sonuga-Barke et al., 2001). Treatment of ADHD at preschool age is very important, otherwise it can cause a lot of disabilities for the child and the family at this age and later in life (Sonuga-Barke et al., 2001).
Since the last decade, ADHD diagnosis has been increased at preschool age, with more demand for non-pharmacological intervention at this age. One reason is the lack of enough study on the efficacy and adverse effects of drugs in children at preschool age. In addition, previous research indicates that Ritalin is not so effective on school-aged children and has more side effects (Greenhill et al., 2006). If non-pharmacological therapies start at lower ages, before the emergence of other disorders and the occurrence of educational and behavioral problems or loss of self-confidence, treatment can be simpler and more effective (Daley & Thompson, 2007).
Training parents about the methods of behavioral management has been suggested as the first treatment of reducing the ADHD symptoms at preschool age (Conner, 1997). Besides, many studies support the effectiveness of this method (Jones et al., 2007; Chronis, Jones, & Raggi, 2006). Parenting practices are in one way different from parenting style as the former focuses on specific parenting behaviors related to nutrition and physical activity while the latter emphasizes on parent-child interactions in different situations (Darling & Steinberg, 1993; Sleddens, Gerards, Thijs, Vries, & Kremers, 2011). In addition, parenting interventions seem to have positive long-term effects on a range of other problems at young age, namely mental, emotional and behavioral disorders; it also affects successful developmental competence (Sandler, Schoenfelder, Wolchik & Mackinnon, 2011).
In particular, positive parenting has been suggested as a critical external factor with strong influences on child’s follow-up issues. In particular, to be a supportive parent since the very young ages of the child, has been proven to positively affect child’s development in cognitive, behavioral, and psychological aspects (Beckwith, Rodning, & Cohen, 1992; Eshel, Daelmans, deMello, & Martines, 2006; Landry, Smith, Swank, & Guttentag, 2008).
Parenting is especially important because of the familial nature of the ADHD disorder. In addition much evidence indicates that such behaviors and ADHD symptoms will appear during child development or even consolidate with comorbid psychopathologies, and so on (Johnston, Mash, Miller, & Ninowski, 2010). In this regard, three interventions are considered as the most effective child-rearing interventions that can reduce the ADHD symptoms in children at preschool age; one of them is Positive Parenting Program (Triple-P) which consists of different training levels. Triple-P is a multi-level parenting and family support strategy developed by the University of Queensland in Brisbane, Australia.
It uses social learning principles and adopts a supportive system-contextual or ecological perspective in parents. The program is widely supported at international level and several related programs have been developed so far to address parents’ special needs (West & Sander, 2012). The standard level of Triple-P method is suitable for training the normal children. This level was taught to a group of child and adolescent’s psychiatrists in Iran and its effectiveness was confirmed on mothers with normal and ADHD children at preschool age.
Considering the importance of non-pharmacological treatment of ADHD at preschool age, evaluation of this kind of treatment in this age group in Iran is essential. The innovation of this research is the use of standard level Triple-P to reduce the symptoms of ADHD in preschoolers. This level is not specific for children with ADHD, but according to our study, it can be useful in reducing symptoms of this disorder. Paying attention to children’s age in our research is also of great importance. The study children were of preschool age and for the first time in Iran, the standard level Triple-P was conducted for ADHD children in this age group. In addition, the number of the participants was higher than other similar research studies. Therefore, we evaluated the impact of implementing Triple-P on preschool aged children suffering from ADHD.
There are several studies in the literature in this topic. Dean et al. (2003) examined Triple-P in a group of people and found that this program could promote parents’ knowledge about child rearing and improve children’s behavior and these effects were persistent for 12 months (Dean, Myors, & Evans, 2003). Besides, Leung, Sanders, Francis, & Joseph, (2006) examined the effectiveness of the Triple-P in a government child-health service context with 661 Chinese parents of preschool and primary school-aged children in Hong Kong.
They showed significant decrease in disruptive child’s behaviors, levels of parenting stress, general stress and anxiety and an increase in parenting sense of competence as well as lower levels of family earnings in the relative social and professional position of the newly immigrant family, and greater pre-intervention levels of parenting stress (Leung et al., 2006). Furthermore, (McTaggart & Sanders, 2007) reported that parents who completed the Triple-P are equally likely to succeed in changing their parenting practices. Their findings suggest the robustness of intervention effects across a diverse range of parents (McTaggart & Sanders, 2007).
The evidence for the efficacy of Triple-P is supported by a series of controlled trials in Australia, although similar trials are in progress in several other countries in Europe and North America (Sanders, 1999). A series of studies have shown that Triple-P is effective in a number of delivery formats (group, individual, phone-assisted and self-directed) with significant reductions in both observed and parent-reported disruptive behaviors, increased parental self-efficacy, reduced levels of dysfunctional parenting (laxness, over-reactivity and verbosity), parental anger, depression, stress, marital conflict and work stress (Ireland, Sanders, & Markie-Dadds, 2003).
Leung et al. (2006) also evaluated Tripe-P on Chinese parents of children with early onset conduct-related problems in Hong Kong. They showed significantly lower levels of child behavioral problems, less parenting styles impairment, and higher parental sense of competence (Leung, Sanders, Leung, Mak, & Lau, 2003). Meanwhile, Whittingham, Sofronoff, Sheffield, & Sanders, (2008) studied 59 families with children suffering from autism spectrum disorders aged between 2 and 9 years.
Using Stepping Stones Triple-P, the researchers reported that the parents’ expectations were better met, their children exhibited acceptable behavior, and their relationship with their partners got better (Whittingham et al., 2008). However, Danforth, Harvey, Ulaszek, and Mckee (2006) Evaluated the effects of group parent training on parent performance, and on the response of 45 children with ADHD and defiant aggressive behavior and reported reduced children’s hyperactive, defiant, and harmful behavior, enhanced parenting style, and minimized parents’ stress (Danforth et al., 2006). In a case study conducted by Daley, Jones, Hutchings and Thompson (2009). three non-pharmacological treatments (one of them was positive parenting) were evaluated in order to reduce ADHD symptoms among preschool aged children (Daley et al., 2009).
In addition, Tehranidoost, Shahrivar, MahmoudiGharaie, and Alaghband-Rad (2009) conducted a study on 120 mothers in Tehran. The results revealed that performing Triple-P child-rearing program improved children’s behavior, parents’ problems and child rearing methods (Tehranidoost et al., 2009). Moreover, Moharreri, Shahrivar, Tehranidoost, and MahmoudiGhara (2008) performed a study on 30 parents with ADHD school-aged children and compared them to controls. They performed standard Triple-P method and observed that ADHD symptoms improved along with the child-rearing scales (Moharreri et al., 2008). After an initial evaluation of the group teen Triple-P program for parents of teenagers, Ralph and Sanders reported significant reductions in conflicts with their young children and the measures of negligent, strong reactions and lack of communication with parents about parenting issues (Ralph & Sanders, 2003).
Because the medication efficacy has been less studied at preschool age or there is controversy among many experts in this regard, alternative methods, including Triple-P can be of great help for managing this disorder at this age. Thus, this research aimed to study the effects of Triple-P on ADHD symptoms of preschool children.
2. Methods
This study is a randomized controlled trial. The study population consisted of parents of ADHD children referred to Imam Hossain Psychiatry Clinic in Tehran, in 2010 and 2011. A total number of 110 parents with preschool-aged children diagnosed with ADHD were recruited from Child Psychiatry Clinic of Imam Hossain Hospital with convenience sampling method. The parents were being interviewed before participating in the study to check the inclusion criteria.
The inclusion criteria were having passed at least 5th grade education, having a preschool child with ADHD diagnosis according to child psychiatrist interview, lacking untreated major psychiatric problems such as psychotic disorders or bipolar disorders (Parents’ psychological health were examined by psychiatrists in Imam Hossain Hospital based on DSM-IV).
The study children should be under stable dose of medication for at least one month. If there were a need for changing medication or its amount, then their mothers would be excluded from the study. In addition, if parents missed more than 3 training sessions they were also excluded. All participants signed a written informed consent. Then, eligible individuals were randomly assigned into control and treatment (subject) group.
After all parents completed a demographic form and pre-test questionnaire, a psychoeducational session about ADHD was held for all parents. Then, the subject group attended in a Triple-P program (Standard level). The subject parents participated in 2-hour sessions per week for 4 weeks followed by 4 phone-based sessions. Each training group included 12 to 15 participants. The first 4 sessions were training sessions. In the next 4 sessions, family problems during practicing and conducting methods in house were addressed. The experienced psychiatrists conducted the course. The experts from the University of Queensland, Australia have taught The standard level of Triple-P to some Iranian child and adolescent psychiatrists and the Iran Ministry of Health confirmed its effectiveness in a large group of mothers with normal children.
Parents in the control group received conventional managements based on routine clinic program, after receiving a psychoeducational session about ADHD. At the end of 8 weeks, the subject and control groups completed the same questionnaires. During the study period, some participants of the subject group were excluded because of more than three sessions absence. In addition, some participants were excluded from the control group due to lack of cooperation in filling the final questionnaires or the need to change their medication during the study. Finally, 94 participants (53 in the subject group and 41 in the control group) finished the study. The obtained data were presented as Mean±SD. A series of Analysis of Covariance (ANCOVA) were performed to compare the groups before and after the intervention. All of these analyses were done in SPSS for Windows (version 19; SPSS Inc., Chicago, IL, USA).
The Family Background Questionnaire provides reliable family history information. Reliability and validity analyses suggest that it is a useful screening instrument for obtaining family history information (Melchert & Kalemeer, 2009). A brief version of this instrument assesses parental responsiveness, child maltreatment, and parental substance abuse. This questionnaire contains essential biographical information, including 1. Name, age, gender and date of birth of the child; 2. Parents’ marital status and relationship with the child; 3. Their current employment status; and 4. Educational background and total family income (Moharreri et al., 2008). The scale has good test-retest reliability and construct validity and internal consistency obtained by Cronbach α as 0.79 to 0.95 (Melchert & Kalemeer, 2009).
The Conner’s ADHD Rating Scale, Parents’ Form screens and evaluates treatment results. This 27-item test is an abbreviated and revised form of an unabridged 93-item version, and parents should respond to it before and after the program. The scale is useful for children aged 3-17 years old and its diagnostic validity and reliability are consistent with DSM-IV criteria.(Conner, 1997). Its subscales include oppositionality, cognitive problems, inattention, hyperactivity, and ADHD index. Its internal consistency is around 0.75 to 0.90 and the test-retest reliability with 8 weeks interval is 0.6 to 0.9. Construction validity of this scale is obtained by factor analysis (ZargariNejad & YekkeYazdandoost, 2007).
The 30-item Parenting Scale measures the dysfunctional discipline style in parents. It yields a total score based on three factors: laxness (permissive discipline); over-reactivity (authoritarian discipline, displaying anger, and irritability); and verbosity (overly long reprimands or reliance on talking) as measured on a 7-point scale. The scale has acceptable internal consistency for the total score (0.87), laxness (0.87), over-reactivity (0.83) and verbosity (0.82) subscales. This scale can differentiate between parents of clinic and non-clinic children. It correlates with self-report measures of child’s behavior, marital discord, and depressive symptoms, as well as observational measures of dysfunctional discipline and child behavior (Arnold, O’leary, Wolff, & Acker, 1993).
The Parent Problem Checklist has 16 items that measures inter-parental conflict on child rearing. The Parent Problem Checklist (PPC) has high internal consistency (α=0.92). It has also high test-retest reliability (r=.90) (Dadds & Powll, 1991). The 42-item Depression, Anxiety Stress Scale measures parental levels of depression and anxiety. The scale has high reliability for the depression (0.91), anxiety (0.81), and stress (0.89) subscales and good discriminative and concurrent validity (Moharreri et al., 2008).
Parenting Sense of Competency Scale was made by Giboud-Wallston and Wandesman in 1978. A 16-item version of this questionnaire, “being a parent scale”, was used to assess parents’ view of their competence as parents’ satisfaction with their parenting role and feeling of efficacy as a parent. The total score shows a good internal consistency (α=0.79) (Bor, Saners, & Marki-Dadds, 2002). Other positive parenting studies have already used all above-mentioned questionnaires and Iranian researchers approved their validity.
3. Results
In the present study, 110 parents participated, but 93 completed the study. Data analysis was performed by analyses of covariance. Result showed that the Mean±SD ages of the children in the treatment and control group were 4.2±1.09 and 3.9±1.23 years, respectively. Data analysis showed no significant difference between two groups (t=0.92, df=82, P=0.35). Table 1 presents the other descriptive statistics of study participants.
Data analysis revealed no significant difference between two groups regarding sex of children (χ2=0.03, df=1, P=0.83), mothers’ education (χ2=4.42, df=5, P=0.53) and mothers’ employment (χ2=2.98, df=1, P=0.08). According to Table 2, ADHD mean of the groups indicated that with 99% confidence, Triple-P has a positive and significant impact on ADHD. Thus, this program could reduce the symptoms of ADHD in the subject group (F=7.21; P<0.01).
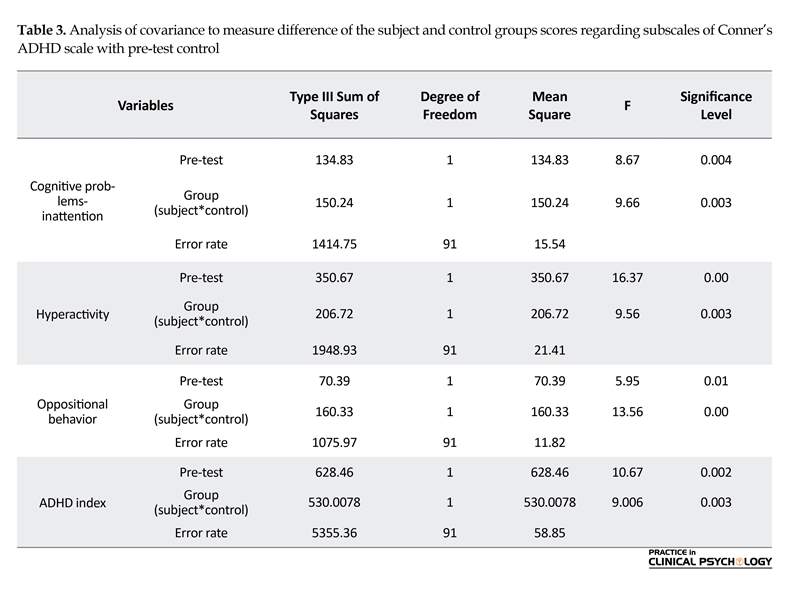
Table 3 presents the covariance test results to measure difference of subscales of Conner’s ADHD rating scale with pre-test control through covariance. As it is seen, the results indicate that Triple-P was effective on cognitive problems of inattention (F=9.66, P<0.01), hyperactivity (F=9.56; P<0.01), oppositional behavior (F=13.56, P<0.01), and ADHD index (P<0.01, F=9.00) improvement.
Table 4 indicates the covariance test for difference measures of depression, anxiety and stress with pre-test control. The results of Table 4 indicate that Triple-P was effective in the depression (F=4.94, P<0.05) and stress (F=3.74, P<0.05) improvement; however, Triple-P had no effect on parents’ anxiety (F=1.74, P=0.19).
According to Table 5, “being a parent” mean value of the two groups indicated that Triple-P had a positive and significant impact on “being a parent scale” (F=19.99; P<0.01). In doing so, Triple-P had a positive and significant impact on parent problem checklist (F=18.51; P<0.01) and also a positive and significant impact on parenting scale and resulted in improving “parenting scale” (F=35.18; P<0.01).
4. Discussion
This study was designed to evaluate the effectiveness of implementing the standard level of positive Parenting Program (Triple-P) in preschool children with ADHD and their parents. Our findings indicate that this method improves the symptoms of children with ADHD and has a positive effect on parents’ relationship.
Table 4 indicates the covariance test for difference measures of depression, anxiety and stress with pre-test control. The results of Table 4 indicate that Triple-P was effective in the depression (F=4.94, P<0.05) and stress (F=3.74, P<0.05) improvement; however, Triple-P had no effect on parents’ anxiety (F=1.74, P=0.19).
According to Table 5, “being a parent” mean value of the two groups indicated that Triple-P had a positive and significant impact on “being a parent scale” (F=19.99; P<0.01). In doing so, Triple-P had a positive and significant impact on parent problem checklist (F=18.51; P<0.01) and also a positive and significant impact on parenting scale and resulted in improving “parenting scale” (F=35.18; P<0.01).
4. Discussion
This study was designed to evaluate the effectiveness of implementing the standard level of positive Parenting Program (Triple-P) in preschool children with ADHD and their parents. Our findings indicate that this method improves the symptoms of children with ADHD and has a positive effect on parents’ relationship.
This finding is in line with many studies indicating the benefits of group-administered Triple-P as an early intervention program for children with disruptive behavior (Whittingham et al., 2008; Markie-Dadds, Sanders, & Turner, 1999; Sanders & McFarland, 2000; Zubrick, Silburn, Burton, & Blair, 2000; Sanders, Kirby, Tellegen, & Day, 2014). Leung et al. (2003) strongly confirmed the efficacy of Triple-P in reducing parental reports of children’ conduct problems and in promoting more harmonious family relationships in Chinese parents living in Hong Kong (Leung and et al., 2003). In Sanders (1999) study, the effect of standard positive parenting on parents with preschool ADHD children with comorbidities was compared to its advanced form and the control group. At the end of the study, the same effect was noted in both treatment groups as behavioral problems reduced in ADHD children compared to the controls (Sanders, 1999). Danforth et al. (2006) also showed that Parent Management Training (PMT) using the behavior management flow chart on parents of children with ADHD improved parenting behaviors and reduced parents’ stress (Danforth et al., 2006).
In Moharreri et al. (2008) study, the parents participating in the Triple-P group displayed significant reduction in the mean number of problems identified between parents on child rearing. This reduction was significant in the over-reactivity, laxness, and verbosity of the studied parents (Moharreri et al., 2008). Such results were similar to Ralph and Sanders study results in terms of reducing the parents’ disagreement with their partner over parenting issues and improving their style (Ralph & Sanders, 2003). Meanwhile, after intervention of Stepping Stones Triple-P among families with children with autism spectrum disorder aged between 2 and 9 years, Whittingham et al. (2008) demonstrated significant improvements in parental reports of child behavior and parenting styles with the treatment effects for the child behavior, parental over-reactivity, and parental verbosity being maintained at 6 months follow-up (Whittingham et al. 2008).
One of the important findings of this study was the impact of positive parenting program on ADHD symptoms in preschool children suffering from this disorder. By reviewing the obtained results, we concluded that training parents with Triple-P methods could reduce the ADHD symptoms in their children. These findings are consistent with the findings of previous studies. The results of Moharari study, conducted by standard level of Triple-P among elementary school students, are in line with the results of the present study among preschoolers. Moharreri et al. (2008) concluded that by implementing positive parenting program, the ADHD-related symptoms would be improved (Moharreri et al., 2008).
A finding of Daley study also suggests a reduction of hyperactivity symptoms using this program (Daley and et al., 2009). In our study, along with reducing overall disorder symptoms, the Triple-P method was effective in reducing Conner’s three subscales and could reduce the symptoms of ADHD. This study is the first group research on Triple-P in Iranian parents with ADHD children in preschool age. It seems that the Triple-P is compatible with Iranian culture.
Applying Triple-P on Iranian families brings considerable comfort in lowering the risk of dealing with advanced and prolonged oppositional/antisocial aspects of ADHD. Furthermore, the results of the present study indicate that Triple-P can also reduce parents’ depression and stress. This can be the result of parents’ empowerment feeling in parenting. As mentioned earlier, Ireland et al. (2003) reported the positive feeling of parents in parenting that lasted after 3 months (Ireland et al., 2003). While in the present study, no effect was observed on parents’ anxiety after evaluation of the results. In contrast, Moharreri et al. (2008) reported a significant reduction in the parents’ level of depression, anxiety, and stress scores (Moharreri et al., 2008).
The discrepancy in the results of the present research and Moharrari study could be due to study subjects of Moharrari who were children aged 6-12 years, while our study was conducted on preschoolers. Besides, parents are worried that their children might experience the relapse symptoms when entering school and facing harder homework. This can be a factor of preserving their anxiety in high level. Likewise, Leung et al. (2006) following intervention on their study participants, reported significantly lower levels of child behavior problems, lower parenting stress, lower depression, anxiety and stress scores, and higher parenting sense of competence.
In this study, positive parenting training had a positive and significant impact on parents’ problem checklist and reduced their problems. In a study conducted by Tehranidoost et al. (2009) performing Triple-P improved parents’ problems and parenting method Tehranidoost et al., 2009). Another finding of our research points to the parenting improvement, which is consistent with other studies. Sanders (1999) performed an advanced form of Triple-P on some families having ADHD children aged 5 to 9 years and found a significant decrease in destructive behavior and improvement in parenting patterns. Besides, the feeling of having better positive-parenting ability in child rearing was reported in comparison to controls and the positive impacts were persistent at least for 3 months.
In Moharreri et al. (2008) study, Triple-P was effective on the reduction of dysfunctional parenting style, as the post-intervention compared the subscale scores and the total score of parenting scale in the subject group with those in the control group (Moharreri et al., 2008). Dean et al. (2003) conducted a research on positive parenting program in a sample group of the society and reported that the program could increase parents’ knowledge about parenting methods.
Considering the difficulties in the rearing of ADHD children compared to non-ADHD children, the affected families need parenting patience, skills, and abilities, and as much as these families acquire parenting skills and receive proper education, their abilities will be increased in controlling the behavior of their children. Positive parenting program for parents of ADHD children will improve their parenting skills and reduce problems related to parenting such as depression and frustration. These methods also reduce behavioral problems of children and increase their abilities.
One of our study limitations was the absence of fathers in Triple-P sessions and the mothers were the only receivers of the training. The other limitation of the present study was comorbid disorders, which overlooked in the studied children. Therefore, we suggest to do further work on these topics in the future similar studies. Triple-P is defined as a brief and time-saving program with significant impact on therapist’s skills, self-confidence and satisfaction of advising parents of children with behavioral problems. Thus, we suggest its use for public health and in line with preventing psychopathology in children. Future work can no doubt lead us to other vast applications of Triple-P.
Ethical Considerations
Compliance with ethical guidelines
All participants signed written informed consent and could leave the study whenever they wished. The participants’ personal information was kept confidential. The routine therapy of children was continued; however, if drug adjustment were required, the medication would be changed but the participant would be excluded from the study.
Funding
This study was supported by Behavioral Sciences Research Centre of Shahid Beheshti University of Medical Sciences.
Authors contributions
Conceptualization: Mojgan Khademi; Methodology: Katayoon Razjooyan, Najmeh Khosrovan Mehr; Investigation: Rozita Davari Ashtiani; Writing–original draft: Mojgan Khademi, Najmeh Khosrovan Mehr; Writing– review & editing: Fatemeh Ayatmehr. Najmeh Khosrovan Mehr; Resources: Mojgan Khademi, Najmeh Khosrovan Mehr; and Supervision: Fariba Arabgol.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
We wish to express our sincere gratitude to the internal manager of Behavioral Sciences Research Centre of Shahid Beheshti University of Medical Sciences for sharing expertise, and sincere and valuable guidance, financial support and encouragement.
References
- Arnold, D. S., O’leary S. G., Wolff, L. S., & Acker, M. M. (1993). The parenting scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5(2), 137-44. [DOI:10.1037/1040-3590.5.2.137]
- Beckwith, C., Rodning, S., & Cohen, D. B. (1992). Preterm children at early adolescence and continuity and discontinuity in maternal responsiveness from infancy. Child Development, 63(5), 1198-208. [PMID]
- Bor, W., Saners, M. R., & Marki-Dadds, C. (2002). The effects of the triple P-positive parecting program on preschool children with co-occurring disruptive behavior and attention/hyperactivity difficulties. Journal of Abnormal Child Psychology, 3(6), 571-8. [DOI:10.1023/A:1020807613155]
- Chronis, A. M., Jones, H. A., & Raggi, V. L. (2006). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Clinical Psychology Review, 26(4), 486-502. [DOI:10.1016/j.cpr.2006.01.002] [PMID]
- Conner, C. O. (1997). Conner’s rating scale revised technical manual. Toronto: Multi-Health Systems.
- Dadds, M. R., & Powll, M. B. (1991). The relationship of interparental conflict and global marital adjustment to aggressive and nonclinic children. Journal of Abnormal Psychology. 19(5), 553-67. [DOI:10.1007/BF00925820]
- Daley, D., & Thompson, M. (2007). Parent training for ADHD in preschool children. Advances in ADHD Research through the Lifespan, 2(1), 11-6.
- Daley, D., Jones, K., Hutchings, J., & Thompson, M. (2009). Attention deficit hyperactivity disorder in pre-school children: current findings, recommended interventions and future directions. Child: Care, Health and Development, 35(6), 754-66.
- Danforth, J. S., Harvey, E., Ulaszek, W. R., & Mckee, T. E. (2006). The outcome of group parent training for families of children with ADHD and defiant/aggressive behavior. Journal of Behavior Therapy and Experimental Psychiatry, 37(3), 188-206. [DOI:10.1016/j.jbtep.2005.05.009] [PMID]
- Darling, N., & Steinberg, L. (1993). Parenting style as context: an integrative model. Psychological Bulletin, 113(3), 487-96. [DOI:10.1037/0033-2909.113.3.487]
- Dean, C., Myors, K., & Evans, E. (2003). Community-wide implementation of a parenting program: The South East Sydney positive parenting project. Australian e-Journal for the Advancement of Mental Health, 2(3), 1446-984. [DOI:10.5172/jamh.2.3.179]
- Eshel, B., Daelmans, M. C., de Mello, M. C., & Martines, J. (2006). Responsive parenting: Interventions and outcomes. Bulletin of the World Health Organization, 84(12), 991-8.
- Greenhill, L., Kollins, S., Abikoff, H., McCracken, J., Riddle, M., & Swanson, B. (2006). Efficacy and safety of immediate-release methylphenidate treatment for preschoolers with ADHD. Journal of the American Academy of Child and Adolescent Psychiatry, 45(11), 1284-93. [DOI:10.1097/01.chi.0000235077.32661.61] [PMID]
- Ireland, J. L, Sanders, M. R., & Markie-Dadds, C. (2003). The impact of parent training on marital functioning: a comparison of two group versions of the triple p–positive parenting Program for parents of children with early-onset conduct problems. Behavioural and Cognitive Psychotherapy, 31(2), 127–42. [DOI:10.1017/S1352465803002017]
- Johnston, C., Mash, E. J., Miller, N., & Ninowski, J. E. (2012). Parenting in adults with Attention-Deficit/Hyperactivity Disorder (ADHD). Clinical Psychology Review, 32(4), 215-28. [DOI:10.1016/j.cpr.2012.01.007] [PMID] [PMCID]
- Jones, K. , Daley, D., Hutchings, J., Bywater, T., & Eames, C. (2007). Efficacy of the incredible years basic parent training programme as an early intervention for children with conduct problems and ADHD. Child: Care, Health and Development, 33(6), 749-56.
- Landry, S. H., Smith, K. E., Swank, P. R., & Guttentag, C. (2008). A responsive parenting intervention: The optimal timing across early childhood for impacting maternal behaviors and child outcomes. Developmental Psychology. 44(5), 335–1353 [DOI:10.1037/a0013030] [PMID] [PMCID]
- Leung, C., Sanders, M., Francis, I. P., & Joseph, L. (2006). Implementation of triple P-positive parenting program in Hong Kong: Predictors of programme completion and clinical outcomes. Journal of Children’s Services, 1(2), 4 17.
- Leung, C., Sanders, M., Leung, S., Mak, R., & Lau, J. (2003). An outcome evaluation of the implementation of the Triple-P- positive parenting programme in Hong Kong. Family Process, 42(4), 531-44. [PMID]
- Markie-Dadds, C., Sanders, M. R., & Turner, K. M. T. (1999). Every parent’s self-help workbook. Brisbane: Triple P International.
- McTaggart, P., & Sanders, M. (2007). Mediators and moderators of change in dysfunctional parenting in a school based universal application of the Triple-P positive parenting programme. Journal of Children’s Services, 2(1), 4-17. [DOI:10.1108/17466660200700002]
- Melchert, T. P., & Kalemeer, A. (2009). A brief version of the family background questionnaire. Measurement and Evaluation in Counseling and Development, 41(4), 1-14.
- Moharreri, F., Shahrivar, Z., Tehranidoost, M., & MahmoudiGhara, J. (2008). Efficacy of the positive parenting program (Triple-p) for parent of children with Attention Deficit Hyperactivity Disorder (ADHD). Iranian Journal of Psychiatry, 3(2), 59-63.
- Ralph, A., & Sanders, M. R. (2003). Preliminary evaluation of the group teen triple P program for parents of teenagers making the transition to high school. Australian e-Journal for the Advancement of Mental Health, 2(3), 1-10.
- Sanders, M. R. (1999). triple P-positive parenting program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clinical Child and Family Psychology Review, 2(2), 71-90.
- Sanders, M. R., Kirby, J. N, Tellegen, C. L., & Day, J. J. (2014). the triple P-positive parenting program: A systematic review and meta-analysis of a multi-level system of parenting support review article. Clinical Psychology Review Journal, 34(4), 337-57. [DOI:10.1016/j.cpr.2014.04.003]
- Sanders, M. R., McFarland, M. (2000).Treatment of depressed mothers with disruptive children: A controlled evaluation of cognitive behavioral family intervention. Behaviour Research and Therapy Journal, 31(1), 89-112.
- Sandler, I. N., Schoenfelder, E. N., Wolchik, S. A., & Mackinnon, D. P. (2011). Long-term impact of prevention programs to promote effective parenting: Lasting effects but uncertain processes. Annual Review of Psychology, 62, 299-329. [DOI:10.1146/annurev.psych.121208.131619] [PMID] [PMCID]
- Sleddens, E. F., Gerards, S. M., Thijs, C., Vries, N. K., & Kremers, S. P. (2011). General parenting, childhood overweight and obesity-inducing behaviors: A review. International Journal of Pediatric Obesity, 6, 12-27. [DOI:10.3109/17477166.2011.566339] [PMID]
- Sonuga-Barke, E. J., Daley, D., Thompson, M., Laver-Bradbury, C., & Weeks, A. (2001). Parent-based therapies for preschool attention-deficit/hyperactivity disorder: A randomized, controlled trial with a community sample. Journal of the American Academy of Child and Adolescent Psychiatry, 40(4), 402-8. [DOI:10.1097/00004583-200104000-00008] [PMID]
- Tehranidoost, M., Shahrivar, Z., MahmoudiGharaie, J.,& Alaghband-Rad, J. (2009). [Efficacy of positive parenting on improving children’s behavior problems and parenting styles (Persian)]. Iranian Journal of Psychiatry, 4(14), 371-9.
- West, F., & Sanders, M. R. (2012). Facilitator’s manual for group lifestyle Triple P. Triple P International. Brisbane: Milton QLD.
- Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M. R. (2008). Stepping stones triple p: An RCT of a parenting program with parents of a child diagnosed with an Autism Spectrum Disorder. Journal of Abnormal Child Psychology, 37(4), 469-80. [DOI:10.1007/s10802-008-9285-x] [PMID]
- ZargariNejad, G. H., & YekkeYazdandoost, R. (2007). [Efficacy of parent’s training on problem behaviors in ADHD children (Persian)]. Psychological Studies, 3(2), 29-48.
- Zubrick, S. R., Silburn, P. B., Burton, P., & Blair, E. (2000). Mental health disorders in children and young people: Scope, cause and prevention. Australian and New Zealand Journal of Psychiatry, 34(4), 570-8. [DOI:10.1080/j.1440-1614.2000.00703.x] [PMID]
Type of Study: Original Research Article |
Subject:
Family and group therapy
Received: 2018/04/13 | Accepted: 2018/10/10 | Published: 2019/01/1
Received: 2018/04/13 | Accepted: 2018/10/10 | Published: 2019/01/1
References
1. Arnold, D. S., O'leary S. G., Wolff, L. S., & Acker, M. M. (1993). The parenting scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5(2), 137-44. [DOI:10.1037/1040-3590.5.2.137] [DOI:10.1037/1040-3590.5.2.137]
2. Beckwith, C., Rodning, S., & Cohen, D. B. (1992). Preterm children at early adolescence and continuity and discontinuity in maternal responsiveness from infancy. Child Development, 63(5), 1198-208. [PMID] [DOI:10.2307/1131527] [PMID]
3. Bor, W., Saners, M. R., & Marki-Dadds, C. (2002). The effects of the triple P-positive parecting program on preschool children with co-occurring disruptive behavior and attention/hyperactivity difficulties. Journal of Abnormal Child Psychology, 3(6), 571-8. [DOI:10.1023/A:1020807613155] [DOI:10.1023/A:1020807613155]
4. Chronis, A. M., Jones, H. A., & Raggi, V. L. (2006). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Clinical Psychology Review, 26(4), 486-502. [DOI:10.1016/j.cpr.2006.01.002] [PMID] [DOI:10.1016/j.cpr.2006.01.002]
5. Conner, C. O. (1997). Conner's rating scale revised technical manual. Toronto: Multi-Health Systems.
6. Dadds, M. R., & Powll, M. B. (1991). The relationship of interparental conflict and global marital adjustment to aggressive and nonclinic children. Journal of Abnormal Psychology. 19(5), 553-67. [DOI:10.1007/BF00925820] [DOI:10.1007/BF00925820]
7. Daley, D., & Thompson, M. (2007). Parent training for ADHD in preschool children. Advances in ADHD Research through the Lifespan, 2(1), 11-6.
8. Daley, D., Jones, K., Hutchings, J., & Thompson, M. (2009). Attention deficit hyperactivity disorder in pre-school children: current findings, recommended interventions and future directions. Child: Care, Health and Development, 35(6), 754-66. [DOI:10.1111/j.1365-2214.2009.00938.x]
9. Danforth, J. S., Harvey, E., Ulaszek, W. R., & Mckee, T. E. (2006). The outcome of group parent training for families of children with ADHD and defiant/aggressive behavior. Journal of Behavior Therapy and Experimental Psychiatry, 37(3), 188-206. [DOI:10.1016/j.jbtep.2005.05.009] [PMID] [DOI:10.1016/j.jbtep.2005.05.009]
10. Darling, N., & Steinberg, L. (1993). Parenting style as context: an integrative model. Psychological Bulletin, 113(3), 487-96. [DOI:10.1037/0033-2909.113.3.487] [DOI:10.1037/0033-2909.113.3.487]
11. Dean, C., Myors, K., & Evans, E. (2003). Community-wide implementation of a parenting program: The South East Sydney positive parenting project. Australian e-Journal for the Advancement of Mental Health, 2(3), 1446-984. [DOI:10.5172/jamh.2.3.179] [DOI:10.5172/jamh.2.3.179]
12. Eshel, B., Daelmans, M. C., de Mello, M. C., & Martines, J. (2006). Responsive parenting: Interventions and outcomes. Bulletin of the World Health Organization, 84(12), 991-8. [DOI:10.2471/BLT.06.030163] [PMID] [PMCID]
13. Greenhill, L., Kollins, S., Abikoff, H., McCracken, J., Riddle, M., & Swanson, B. (2006). Efficacy and safety of immediate-release methylphenidate treatment for preschoolers with ADHD. Journal of the American Academy of Child and Adolescent Psychiatry, 45(11), 1284-93. [DOI:10.1097/01.chi.0000235077.32661.61] [PMID] [DOI:10.1097/01.chi.0000235077.32661.61]
14. Ireland, J. L, Sanders, M. R., & Markie-Dadds, C. (2003). The impact of parent training on marital functioning: a comparison of two group versions of the triple p–positive parenting Program for parents of children with early-onset conduct problems. Behavioural and Cognitive Psychotherapy, 31(2), 127–42. [DOI:10.1017/S1352465803002017] [DOI:10.1017/S1352465803002017]
15. Johnston, C., Mash, E. J., Miller, N., & Ninowski, J. E. (2012). Parenting in adults with Attention-Deficit/Hyperactivity Disorder (ADHD). Clinical Psychology Review, 32(4), 215-28. [DOI:10.1016/j.cpr.2012.01.007] [PMID] [PMCID] [DOI:10.1016/j.cpr.2012.01.007]
16. Jones, K. , Daley, D., Hutchings, J., Bywater, T., & Eames, C. (2007). Efficacy of the incredible years basic parent training programme as an early intervention for children with conduct problems and ADHD. Child: Care, Health and Development, 33(6), 749-56. [DOI:10.1111/j.1365-2214.2007.00747.x]
17. Landry, S. H., Smith, K. E., Swank, P. R., & Guttentag, C. (2008). A responsive parenting intervention: The optimal timing across early childhood for impacting maternal behaviors and child outcomes. Developmental Psychology. 44(5), 335–1353 [DOI:10.1037/a0013030] [PMID] [PMCID] [DOI:10.1037/a0013030]
18. Leung, C., Sanders, M., Francis, I. P., & Joseph, L. (2006). Implementation of triple P-positive parenting program in Hong Kong: Predictors of programme completion and clinical outcomes. Journal of Children's Services, 1(2), 4 17. [DOI:10.1108/17466660200600010]
19. Leung, C., Sanders, M., Leung, S., Mak, R., & Lau, J. (2003). An outcome evaluation of the implementation of the Triple-P- positive parenting programme in Hong Kong. Family Process, 42(4), 531-44. [PMID] [DOI:10.1111/j.1545-5300.2003.00531.x] [PMID]
20. Markie-Dadds, C., Sanders, M. R., & Turner, K. M. T. (1999). Every parent's self-help workbook. Brisbane: Triple P International.
21. McTaggart, P., & Sanders, M. (2007). Mediators and moderators of change in dysfunctional parenting in a school based universal application of the Triple-P positive parenting programme. Journal of Children's Services, 2(1), 4-17. [DOI:10.1108/17466660200700002] [DOI:10.1108/17466660200700002]
22. Melchert, T. P., & Kalemeer, A. (2009). A brief version of the family background questionnaire. Measurement and Evaluation in Counseling and Development, 41(4), 1-14. [DOI:10.1080/07481756.2009.11909830]
23. Moharreri, F., Shahrivar, Z., Tehranidoost, M., & MahmoudiGhara, J. (2008). Efficacy of the positive parenting program (Triple-p) for parent of children with Attention Deficit Hyperactivity Disorder (ADHD). Iranian Journal of Psychiatry, 3(2), 59-63.
24. Ralph, A., & Sanders, M. R. (2003). Preliminary evaluation of the group teen triple P program for parents of teenagers making the transition to high school. Australian e-Journal for the Advancement of Mental Health, 2(3), 1-10. [DOI:10.5172/jamh.2.3.169]
25. Sanders, M. R. (1999). triple P-positive parenting program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clinical Child and Family Psychology Review, 2(2), 71-90. [DOI:10.1023/A:1021843613840] [PMID]
26. Sanders, M. R., Kirby, J. N, Tellegen, C. L., & Day, J. J. (2014). the triple P-positive parenting program: A systematic review and meta-analysis of a multi-level system of parenting support review article. Clinical Psychology Review Journal, 34(4), 337-57. [DOI:10.1016/j.cpr.2014.04.003] [DOI:10.1016/j.cpr.2014.04.003]
27. Sanders, M. R., McFarland, M. (2000).Treatment of depressed mothers with disruptive children: A controlled evaluation of cognitive behavioral family intervention. Behaviour Research and Therapy Journal, 31(1), 89-112. [DOI:10.1016/S0005-7894(00)80006-4]
28. Sandler, I. N., Schoenfelder, E. N., Wolchik, S. A., & Mackinnon, D. P. (2011). Long-term impact of prevention programs to promote effective parenting: Lasting effects but uncertain processes. Annual Review of Psychology, 62, 299-329. [DOI:10.1146/annurev.psych.121208.131619] [PMID] [PMCID] [DOI:10.1146/annurev.psych.121208.131619]
29. Sleddens, E. F., Gerards, S. M., Thijs, C., Vries, N. K., & Kremers, S. P. (2011). General parenting, childhood overweight and obesity-inducing behaviors: A review. International Journal of Pediatric Obesity, 6, 12-27. [DOI:10.3109/17477166.2011.566339] [PMID] [DOI:10.3109/17477166.2011.566339]
30. Sonuga-Barke, E. J., Daley, D., Thompson, M., Laver-Bradbury, C., & Weeks, A. (2001). Parent-based therapies for preschool attention-deficit/hyperactivity disorder: A randomized, controlled trial with a community sample. Journal of the American Academy of Child and Adolescent Psychiatry, 40(4), 402-8. [DOI:10.1097/00004583-200104000-00008] [PMID] [DOI:10.1097/00004583-200104000-00008]
31. Tehranidoost, M., Shahrivar, Z., MahmoudiGharaie, J.,& Alaghband-Rad, J. (2009). [Efficacy of positive parenting on improving children's behavior problems and parenting styles (Persian)]. Iranian Journal of Psychiatry, 4(14), 371-9.
32. West, F., & Sanders, M. R. (2012). Facilitator's manual for group lifestyle Triple P. Triple P International. Brisbane: Milton QLD.
33. Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M. R. (2008). Stepping stones triple p: An RCT of a parenting program with parents of a child diagnosed with an Autism Spectrum Disorder. Journal of Abnormal Child Psychology, 37(4), 469-80. [DOI:10.1007/s10802-008-9285-x] [PMID] [DOI:10.1007/s10802-008-9285-x]
34. ZargariNejad, G. H., & YekkeYazdandoost, R. (2007). [Efficacy of parent's training on problem behaviors in ADHD children (Persian)]. Psychological Studies, 3(2), 29-48.
35. Zubrick, S. R., Silburn, P. B., Burton, P., & Blair, E. (2000). Mental health disorders in children and young people: Scope, cause and prevention. Australian and New Zealand Journal of Psychiatry, 34(4), 570-8. [DOI:10.1080/j.1440-1614.2000.00703.x] [PMID] [DOI:10.1080/j.1440-1614.2000.00703.x]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
