

Volume 13, Issue 4 (Autumn 2025)
PCP 2025, 13(4): 319-332 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Azhdari A, Soleimanian A, Darrodi H. The Effectiveness of Time Perspective Intervention on Quality of Life and Brain Behavioral Systems in a Group of Obese and Overweight Women. PCP 2025; 13 (4) :319-332
URL: http://jpcp.uswr.ac.ir/article-1-1030-en.html
URL: http://jpcp.uswr.ac.ir/article-1-1030-en.html



1- Department of Counseling, Faculty of Basic Sciences and Humanities, Bojnourd Branch, Islamic Azad University, Bojnourd, Iran.
2- Department of Counseling, Faculty of Humanities, University of Bojnord, Bojnord, Iran. ,soliemanian@gmail.com
3- Department of Educational Sciences and Counseling, Faculty of Humanities, University of Bojnord, Bojnord, Iran.
2- Department of Counseling, Faculty of Humanities, University of Bojnord, Bojnord, Iran. ,
3- Department of Educational Sciences and Counseling, Faculty of Humanities, University of Bojnord, Bojnord, Iran.
Full-Text [PDF 695 kb]
(596 Downloads)
| Abstract (HTML) (1267 Views)

Full-Text: (495 Views)
Introduction
Obesity and overweight are critical global health issues that significantly impact physical and mental well-being. According to the World Health Organization (WHO), in 2022, 43% of adults aged 18 years and older were overweight, and 16% were obese. The prevalence of obesity has more than doubled since 1990, with 2.5 billion adults being overweight, including 890 million with obesity (Murray et al., 2020). Obesity is more prevalent in women than in men. A recent study, conducted between 2016 and 2019 on over 8,000 Iranian adults aged >35 years, revealed that approximately 37.5% of women and 34.5% of men in Tehran Province, Iran, were either obese or overweight. Additionally, the study indicated a higher prevalence of obesity and overweight among individuals from lower socioeconomic classes and older age groups (Shafiee et al., 2024). This concerning trend underscores the critical need to investigate the consequences of obesity.
Obesity, a multifaceted disorder influenced by both genetic and environmental factors, has significant adverse effects on individuals’ physical and mental health. A comprehensive analysis of adults aged >18 years in India found that obesity is positively correlated with issues, such as fatigue, joint pain, back pain, shortness of breath, binge eating, irritability, stress, anxiety, and depressive symptoms. Additionally, individuals with a higher body mass index (BMI) reported lower quality of life (QoL) (Asharaf et al., 2024). Further studies have indicated that obese women experience more dissatisfaction with their body image than obese men (Sarwer & Polonsky, 2016). The relationship between obesity and mental health appears to be bidirectional. Some studies have shown that the risk of obesity increases two- to three-fold in individuals with mental illness, while the risk of developing mental illness in obese individuals ranges from 30% to 70% (De Hert et al., 2011). Moreover, obesity is associated with various psychiatric disorders, including mood disorders, anxiety, personality disorders, attention deficit hyperactivity disorder, binge eating disorder, trauma, and schizophrenia. It is also a common side effect among individuals using medications to treat mental illnesses (Remington, 2006).
While numerous studies have explored the factors influencing obesity and its physical, psychological, and social impacts, there has been less research on obesity and overweight in women. Obese women face a heightened risk of various diseases, including heart disease, diabetes, and certain cancers, such as breast and colorectal cancer (Elmaleh-Sachs et al., 2023). Additionally, obesity can adversely affect reproductive health, causing complications, such as polycystic ovary syndrome and fertility issues (Kulie et al., 2011). The psychological burden is also substantial, with higher incidences of depression and anxiety among obese women (Lingvay et al., 2024). Studies have demonstrated that obesity can impact multiple dimensions of QoL (Davis et al., 2024; Li & Tien, 2024).
WHO defines QoL as an individual’s perception of their position in life within the context of their culture, value systems, goals, expectations, standards, and concerns. QoL encompasses various components, including physical health, psychological state, level of independence, social relationships, and the environment. These components collectively contribute to an individual’s overall well-being and life satisfaction (Kahn et al., 2020). Women with obesity are at a higher risk of developing mental health disorders, such as depression, anxiety, and eating disorders (Golmohammadi et al., 2024). Social stigma and discrimination associated with obesity can exacerbate these mental health issues, leading to a vicious cycle of emotional distress and further weight gain. Obesity can also impact social health by affecting interpersonal relationships and social interactions. Women with obesity may experience social isolation, reduced social support, and lower self-esteem due to societal beauty standards and weight-related prejudices (Hajek et al., 2021; Cho et al., 2014; González-Fernández et al., 2024). These social challenges can hinder their ability to form and maintain healthy relationships, diminishing their QoL. Overall life satisfaction is often lower among women with obesity than their non-obese counterparts. Physical and mental health burdens and social challenges contribute to a lower sense of well-being and fulfillment.
Another factor associated with obesity and overweight individuals is the functioning of behavioral brain systems. Obese women often face significant difficulties in both behavioral inhibition and activation, leading to challenges in resisting food cravings and overeating. Behavioral inhibition involves suppressing inappropriate or undesired behaviors, whereas behavioral activation involves initiating and maintaining goal-directed behaviors. Research indicates that obese women exhibit notable impairments in behavioral inhibition, which are linked to increased impulsivity and altered neural circuits, particularly in the frontal and limbic regions of the brain that are essential for cognitive control and inhibition. These neural alterations contribute to the difficulty obese women experience in managing their eating behaviors, thus promoting weight gain and the persistence of obesity (Saruco & Pleger, 2021). Furthermore, obese women with additional psychological comorbidities, such as depression, tend to encounter even greater challenges in behavioral activation due to diminished motivation and reduced physical activity. This results in a cycle of emotional eating and inactivity, which further exacerbates weight gain and complicates efforts to manage weight (Kern et al., 2019).
Numerous therapeutic and psychological methods have been employed to assist obese and overweight patients. One particularly effective intervention is time perspective (TP). Zimbardo and Boyd describe TP as “the often non-conscious personal attitude we each hold towards time, which segments the continuous flow of existence into time categories that provide order, coherence, and meaning to our live” (Zimbardo, 2002). Based on their foundational theoretical perspectives and empirical studies, Zimbardo and Boyd identified five dimensions of TP: Past-positive (a warm and sentimental view of the past), past-negative (a negative and aversive view of the past), present-hedonistic (a focus on immediate pleasure with little regard for future consequences), present-fatalistic (a sense of having little control over one’s life and an attitude of helplessness), and future (aspirations for future rewards and goals). Additionally, Zimbardo and Boyd introduced the balanced TP (BTP) concept, defining it as the mental ability to switch effectively among TPs depending on task characteristics, situational contexts, and personal resources. This balanced approach contrasts with a bias towards a specific TP, which may not be the most adaptive for a given situation. Zimbardo further argued that “in an optimally balanced TP, the past, present, and future elements blend and flexibly engage, responding to situational demands and our needs and values” (Zimbardo, 2002).
Previous studies in Iran have provided promising evidence for the effectiveness of TP therapy in various populations and psychological conditions. For instance, it has been shown to reduce anxiety in adolescent girls (Hosseini et al., 2020), alleviate psychological distress in menopausal women (Ebrahimi et al., 2023), enhance well-being and happiness in veterans with PTSD (Malekiha & Moradi, 2019), and decrease depressive symptoms while improving social health in bereaved women (Mousavi et al., 2019). While these findings support the general value of TP-based interventions, several limitations in the existing literature distinguish this study. First, many prior studies, such as Ebrahimi et al. (2023), did not include a follow-up phase, leaving the long-term effectiveness of the intervention uncertain. Second, some studies have combined TP therapy with other techniques, such as mindfulness (Rahimpour et al., 2021; Hemmati et al., 2025), making it difficult to isolate the specific contribution of TP interventions to the observed outcomes. Furthermore, most existing research has been conducted on academic or student populations, limiting the generalizability of the findings to broader health contexts. Critically, the role of TP intervention in health psychology—and specifically among high-risk groups such as overweight and obese women—remains underexplored. The current study addresses these gaps by evaluating the independent effects of TP therapy, including a follow-up phase, in a clinical sample of obese and overweight women, thereby offering novel insights into its potential applications in health-related behavioral and psychological outcomes.
While the relationship between TP and psychological well-being has been widely explored in correlational and cross-sectional research, there remains a significant gap in experimental studies evaluating the therapeutic effectiveness of TP-based interventions. Most existing studies have focused on the general population or individuals with specific psychological disorders, with limited attention to clinical applications targeting lifestyle-related health conditions, such as obesity. Moreover, obese and overweight women represent a particularly vulnerable group, often experiencing reduced QoL and altered behavioral regulation due to physiological and psychosocial factors. Despite this, little empirical evidence exists on whether modifying TP can positively influence their psychological functioning and brain-behavioral systems. To address this gap, the present study investigated the effectiveness of TP-based psychotherapy in improving QoL and behavioral activation/inhibition systems in overweight and obese women.
Materials and Methods
Participants and design
This study utilized a quasi-experimental design with a pre-test-post-test arrangement, incorporating a control group and a one-month follow-up period. The statistical population consisted of overweight and obese women aged 18-48 who sought services at the Amin Counseling Center of the Islamic Azad University, Bojnourd Branch, during the first half of 2024.
Using G*Power software, version 3.1 (Faul et al., 2009), a priori power analysis was conducted to estimate the required sample size for a repeated-measure analysis of variance (ANOVA), assuming a medium effect size (f=0.25), an alpha level of 0.05, and a statistical power of 0.8. The analysis suggested a minimum of 20 participants. Accordingly, 21 eligible individuals were purposefully selected and randomly assigned to either the experimental group (n=10) or the control group (n=11), meeting the recommended sample size for adequate statistical power. The experimental group participated in six sessions of the TP intervention, each lasting 90 minutes and conducted weekly, while the control group did not receive any psychological intervention. During the intervention, three participants from the experimental group withdrew, leaving a final sample of 18 participants (seven in the experimental group and 11 in the control group). The study sampling process is illustrated in Figure 1.
Obesity and overweight are critical global health issues that significantly impact physical and mental well-being. According to the World Health Organization (WHO), in 2022, 43% of adults aged 18 years and older were overweight, and 16% were obese. The prevalence of obesity has more than doubled since 1990, with 2.5 billion adults being overweight, including 890 million with obesity (Murray et al., 2020). Obesity is more prevalent in women than in men. A recent study, conducted between 2016 and 2019 on over 8,000 Iranian adults aged >35 years, revealed that approximately 37.5% of women and 34.5% of men in Tehran Province, Iran, were either obese or overweight. Additionally, the study indicated a higher prevalence of obesity and overweight among individuals from lower socioeconomic classes and older age groups (Shafiee et al., 2024). This concerning trend underscores the critical need to investigate the consequences of obesity.
Obesity, a multifaceted disorder influenced by both genetic and environmental factors, has significant adverse effects on individuals’ physical and mental health. A comprehensive analysis of adults aged >18 years in India found that obesity is positively correlated with issues, such as fatigue, joint pain, back pain, shortness of breath, binge eating, irritability, stress, anxiety, and depressive symptoms. Additionally, individuals with a higher body mass index (BMI) reported lower quality of life (QoL) (Asharaf et al., 2024). Further studies have indicated that obese women experience more dissatisfaction with their body image than obese men (Sarwer & Polonsky, 2016). The relationship between obesity and mental health appears to be bidirectional. Some studies have shown that the risk of obesity increases two- to three-fold in individuals with mental illness, while the risk of developing mental illness in obese individuals ranges from 30% to 70% (De Hert et al., 2011). Moreover, obesity is associated with various psychiatric disorders, including mood disorders, anxiety, personality disorders, attention deficit hyperactivity disorder, binge eating disorder, trauma, and schizophrenia. It is also a common side effect among individuals using medications to treat mental illnesses (Remington, 2006).
While numerous studies have explored the factors influencing obesity and its physical, psychological, and social impacts, there has been less research on obesity and overweight in women. Obese women face a heightened risk of various diseases, including heart disease, diabetes, and certain cancers, such as breast and colorectal cancer (Elmaleh-Sachs et al., 2023). Additionally, obesity can adversely affect reproductive health, causing complications, such as polycystic ovary syndrome and fertility issues (Kulie et al., 2011). The psychological burden is also substantial, with higher incidences of depression and anxiety among obese women (Lingvay et al., 2024). Studies have demonstrated that obesity can impact multiple dimensions of QoL (Davis et al., 2024; Li & Tien, 2024).
WHO defines QoL as an individual’s perception of their position in life within the context of their culture, value systems, goals, expectations, standards, and concerns. QoL encompasses various components, including physical health, psychological state, level of independence, social relationships, and the environment. These components collectively contribute to an individual’s overall well-being and life satisfaction (Kahn et al., 2020). Women with obesity are at a higher risk of developing mental health disorders, such as depression, anxiety, and eating disorders (Golmohammadi et al., 2024). Social stigma and discrimination associated with obesity can exacerbate these mental health issues, leading to a vicious cycle of emotional distress and further weight gain. Obesity can also impact social health by affecting interpersonal relationships and social interactions. Women with obesity may experience social isolation, reduced social support, and lower self-esteem due to societal beauty standards and weight-related prejudices (Hajek et al., 2021; Cho et al., 2014; González-Fernández et al., 2024). These social challenges can hinder their ability to form and maintain healthy relationships, diminishing their QoL. Overall life satisfaction is often lower among women with obesity than their non-obese counterparts. Physical and mental health burdens and social challenges contribute to a lower sense of well-being and fulfillment.
Another factor associated with obesity and overweight individuals is the functioning of behavioral brain systems. Obese women often face significant difficulties in both behavioral inhibition and activation, leading to challenges in resisting food cravings and overeating. Behavioral inhibition involves suppressing inappropriate or undesired behaviors, whereas behavioral activation involves initiating and maintaining goal-directed behaviors. Research indicates that obese women exhibit notable impairments in behavioral inhibition, which are linked to increased impulsivity and altered neural circuits, particularly in the frontal and limbic regions of the brain that are essential for cognitive control and inhibition. These neural alterations contribute to the difficulty obese women experience in managing their eating behaviors, thus promoting weight gain and the persistence of obesity (Saruco & Pleger, 2021). Furthermore, obese women with additional psychological comorbidities, such as depression, tend to encounter even greater challenges in behavioral activation due to diminished motivation and reduced physical activity. This results in a cycle of emotional eating and inactivity, which further exacerbates weight gain and complicates efforts to manage weight (Kern et al., 2019).
Numerous therapeutic and psychological methods have been employed to assist obese and overweight patients. One particularly effective intervention is time perspective (TP). Zimbardo and Boyd describe TP as “the often non-conscious personal attitude we each hold towards time, which segments the continuous flow of existence into time categories that provide order, coherence, and meaning to our live” (Zimbardo, 2002). Based on their foundational theoretical perspectives and empirical studies, Zimbardo and Boyd identified five dimensions of TP: Past-positive (a warm and sentimental view of the past), past-negative (a negative and aversive view of the past), present-hedonistic (a focus on immediate pleasure with little regard for future consequences), present-fatalistic (a sense of having little control over one’s life and an attitude of helplessness), and future (aspirations for future rewards and goals). Additionally, Zimbardo and Boyd introduced the balanced TP (BTP) concept, defining it as the mental ability to switch effectively among TPs depending on task characteristics, situational contexts, and personal resources. This balanced approach contrasts with a bias towards a specific TP, which may not be the most adaptive for a given situation. Zimbardo further argued that “in an optimally balanced TP, the past, present, and future elements blend and flexibly engage, responding to situational demands and our needs and values” (Zimbardo, 2002).
Previous studies in Iran have provided promising evidence for the effectiveness of TP therapy in various populations and psychological conditions. For instance, it has been shown to reduce anxiety in adolescent girls (Hosseini et al., 2020), alleviate psychological distress in menopausal women (Ebrahimi et al., 2023), enhance well-being and happiness in veterans with PTSD (Malekiha & Moradi, 2019), and decrease depressive symptoms while improving social health in bereaved women (Mousavi et al., 2019). While these findings support the general value of TP-based interventions, several limitations in the existing literature distinguish this study. First, many prior studies, such as Ebrahimi et al. (2023), did not include a follow-up phase, leaving the long-term effectiveness of the intervention uncertain. Second, some studies have combined TP therapy with other techniques, such as mindfulness (Rahimpour et al., 2021; Hemmati et al., 2025), making it difficult to isolate the specific contribution of TP interventions to the observed outcomes. Furthermore, most existing research has been conducted on academic or student populations, limiting the generalizability of the findings to broader health contexts. Critically, the role of TP intervention in health psychology—and specifically among high-risk groups such as overweight and obese women—remains underexplored. The current study addresses these gaps by evaluating the independent effects of TP therapy, including a follow-up phase, in a clinical sample of obese and overweight women, thereby offering novel insights into its potential applications in health-related behavioral and psychological outcomes.
While the relationship between TP and psychological well-being has been widely explored in correlational and cross-sectional research, there remains a significant gap in experimental studies evaluating the therapeutic effectiveness of TP-based interventions. Most existing studies have focused on the general population or individuals with specific psychological disorders, with limited attention to clinical applications targeting lifestyle-related health conditions, such as obesity. Moreover, obese and overweight women represent a particularly vulnerable group, often experiencing reduced QoL and altered behavioral regulation due to physiological and psychosocial factors. Despite this, little empirical evidence exists on whether modifying TP can positively influence their psychological functioning and brain-behavioral systems. To address this gap, the present study investigated the effectiveness of TP-based psychotherapy in improving QoL and behavioral activation/inhibition systems in overweight and obese women.
Materials and Methods
Participants and design
This study utilized a quasi-experimental design with a pre-test-post-test arrangement, incorporating a control group and a one-month follow-up period. The statistical population consisted of overweight and obese women aged 18-48 who sought services at the Amin Counseling Center of the Islamic Azad University, Bojnourd Branch, during the first half of 2024.
Using G*Power software, version 3.1 (Faul et al., 2009), a priori power analysis was conducted to estimate the required sample size for a repeated-measure analysis of variance (ANOVA), assuming a medium effect size (f=0.25), an alpha level of 0.05, and a statistical power of 0.8. The analysis suggested a minimum of 20 participants. Accordingly, 21 eligible individuals were purposefully selected and randomly assigned to either the experimental group (n=10) or the control group (n=11), meeting the recommended sample size for adequate statistical power. The experimental group participated in six sessions of the TP intervention, each lasting 90 minutes and conducted weekly, while the control group did not receive any psychological intervention. During the intervention, three participants from the experimental group withdrew, leaving a final sample of 18 participants (seven in the experimental group and 11 in the control group). The study sampling process is illustrated in Figure 1.
All participants provided informed consent after being thoroughly informed of the study’s purpose, procedures, and potential risks and benefits. The confidentiality and anonymity of the participants were strictly maintained throughout the study, and the data were securely stored to ensure privacy.
Inclusion and exclusion criteria
The inclusion criteria included absence of a mental disorder (self-reported), not being pregnant, a body mass index greater than 24, willingness to participate in the study, having at least a high school diploma, and being within the age range of 18 to 48 years. The exclusion criteria included missing more than one session, not completing assigned tasks, and taking certain medications.
Procedures
To recruit participants, a public announcement was disseminated under the title “Free group therapy for obese and overweight women.” The announcement included a brief introduction to the facilitator’s background and qualifications and an overview of the intervention, which was described as a TP psychotherapy program. The advertisement outlined the potential psychological and emotional benefits of participation and clearly stated that the program was offered free of charge. The eligibility criteria were specified, and it was emphasized that both students and non-students who met these criteria were welcome to participate. The recruitment strategy aimed to ensure broad accessibility and encourage voluntary participation by women in the target population. Data were collected using the WHO QoL questionnaire (WHOQOL-BREF) and the behavioral inhibition and activation system scales (BIS/BAS).
QoL questionnaire
The present study utilized the WHO QoL questionnaire (WHOQOL-BREF) as one of its instruments. This questionnaire assesses various domains of individuals’ QoL using 26 items. It comprises four subscales: Physical health (items 3, 4, 10, 15, 16, 17, and 18), psychological health (items 5, 6, 7, 11, 19, and 26), social relationships (items 20, 21, and 22), environment (items 8, 9, 12, 13, 14, 23, 24, 25), and overall QoL (items 1 and 2). Higher scores indicate better QoL in the respective domains (WHOQOL Group, 1995). Bonomi reported an internal reliability of 0.95 for the test in his study (Bonomi et al., 2000). This questionnaire, designed and translated in 2000 across 15 countries, underwent standardization, translation, and psychometric testing of the Persian version by Nejat et al. (2006). To assess its validity and reliability, the questionnaire was administered to 1,167 individuals from Tehran, divided into two groups with chronic and non-chronic diseases. The test re-test reliability for the subscales was as follows: Physical health, 0.77; mental health, 0.77; social relationships, 0.75; and environmental health, 0.84.
BIS/BAS
Another instrument utilized in this study was the BIS/BAS, designed by Carver and White in 1994. This self-report questionnaire measures responses on a four-point Likert scale ranging from “strongly agree” to “strongly disagree,” with scores ranging from 1 to 4. The questionnaire comprises 20 items and two primary factors: Inhibition (seven items) and activation (13 items). The activation factor comprises three components: Drive (four items), fun-seeking (four items), and reward responsiveness (five items). The inhibition factor also includes sensitivity to the behavioral inhibition system (BIS) (seven items). The reported Cronbach’s α coefficients are 0.74 for the inhibition scale, and for the activation scales—reward, drive, and fun seeking—they are 0.73, 0.76, and 0.66, respectively (Carver & White, 1994). The psychometric properties of this scale were evaluated with the student population at Shiraz University, revealing good validity and reliability. The correlation coefficients for the behavioral inhibition scale with depression and anxiety were found to be significant at 0.22 and 0.31, respectively. Examination of the internal consistency showed Cronbach’s α coefficients of 0.69 for the inhibition scale, 0.78 for the total activation score, and 0.87, 0.74, and 0.65 for its three subscales—drive, reward, and fun seeking, respectively. The test re-test reliability over two weeks yielded coefficients of 0.71 for the inhibition scale, 0.73 for the total activation score, and 0.62 and 0.71 for the drive, reward, and fun-seeking subscales, respectively, all of which were significant (Mohammadi, 2008).
TP intervention plan
The TP intervention was implemented based on the training protocol developed by Zimbardo and Boyd (2014). The program consisted of six structured sessions, each lasting approximately one hour and conducted once per week. The intervention was designed to help participants recognize and adjust their cognitive and emotional orientations toward time, to foster a more balanced TP. The sessions included a combination of psychoeducation, guided mental imagery exercises focusing on positive and negative past experiences, motivational enhancement strategies, mindfulness and breathing techniques, and practical activities to increase future-oriented thinking while reducing over-reliance on past-negative and present-fatalistic perspectives.
The content and structure of the sessions were adapted to the needs of overweight and obese women, with an emphasis on improving psychological well-being and enhancing self-regulation. Each session built upon the previous one, encouraging reflection and behavioral integration of TP concepts into daily life. Table 1 presents the details of the intervention in the experimental group.

Data analysis
Data analysis encompassed descriptive (Mean±SD) and inferential statistical (mixed analysis of variance) methods.
Results
Descriptive results
The demographic analysis revealed that the average age of participants in the experimental group was 32.57±9.78 years, while the control group had an average age of 36.91±7.36 years. Additionally, 71.43% of individuals in the experimental group and 63.64% in the control group held a bachelor’s degree. Employment status was distributed as follows: In the experimental group, 42.86% were students, 14.29% were employed, and 42.86% were housewives; in the control group, 54.54% were employed and 45.46% were housewives. Regarding marital status, 42.86% of the experimental group were married with children, whereas all participants in the control group were married with children. The mean BMI was 30.06 in the experimental group and 28.72 in the control group. Statistical analyses showed no significant differences in age, employment status, education level, or BMI (P<0.05). However, chi-square test results indicated a significant difference in marital status and childbearing between the groups (χ2=11.67 (4), P<0.05).
Table 2 presents the Mean±SD of the QoL variables and behavioral brain systems across the pre-test, post-test, and follow-up stages, for both the experimental and control groups.
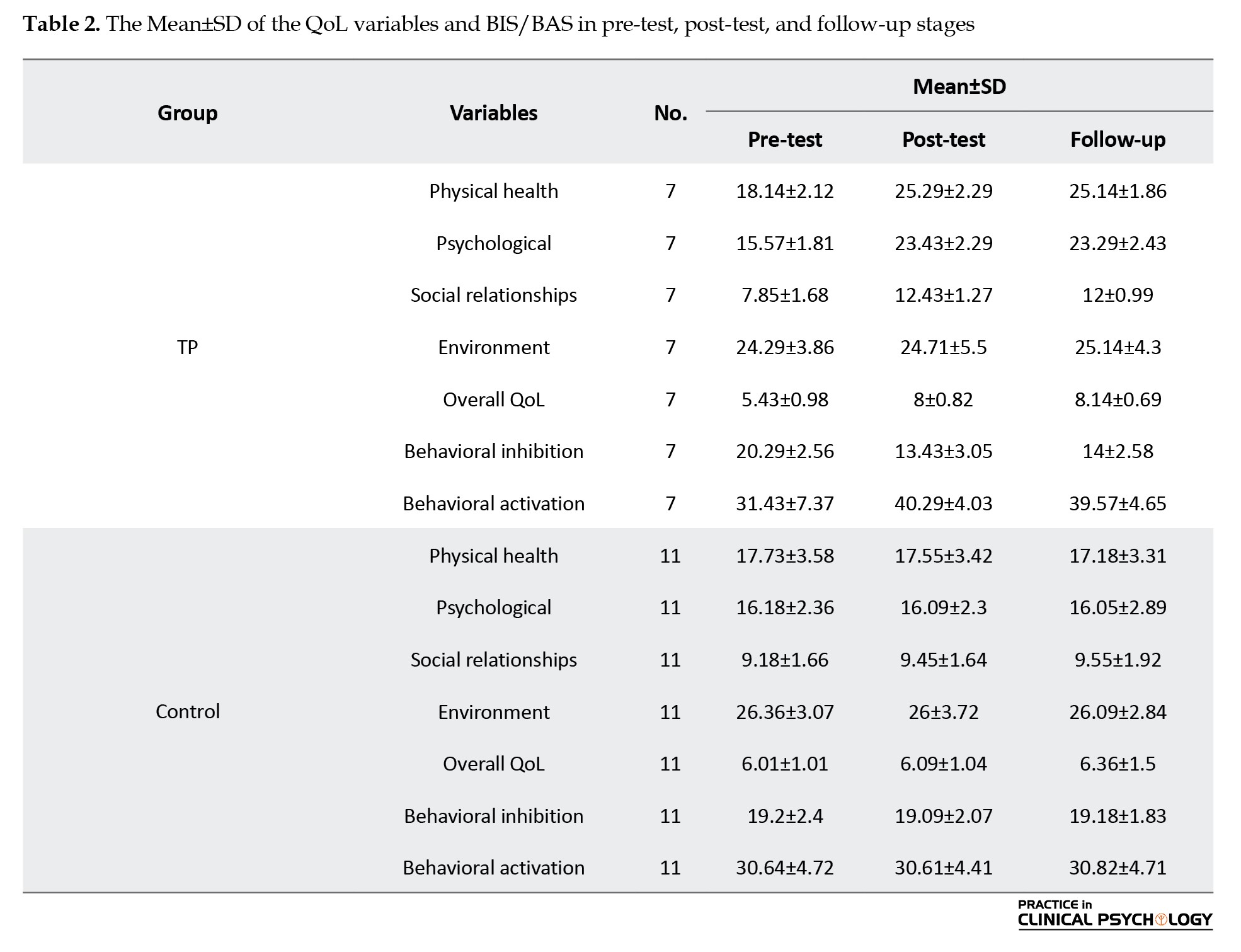
Analysis of Table 2 indicates that the mean scores for QoL and behavioral inhibition and activation in the experimental group improved from the pre-test to the post-test stage. Specifically, post-test mean scores for QoL and behavioral activation increased, while mean scores for behavioral inhibition decreased.
Repeated measures analysis of variance (ANOVA)
Before the repeated measures analysis of variance, the assumptions underlying this parametric test were evaluated. The Shapiro-Wilk test confirmed normality by group (P<0.05). Levene’s test verified the homogeneity of variances (P<0.05). However, the Mauchly test suggested that the sphericity assumption was not met for the variables of physical health, overall QoL, and behavioral activation (P<0.05); thus, the Greenhouse-Geiser correction was applied.
The Wilks’ Lambda test yielded significant results for test stages, group membership, and the interaction between test stages and group membership (P<0.01). Table 3 presents the detailed outcomes of the repeated measures analysis of variance for QoL and behavioral inhibition/activation dimensions.

Table 3 reveals significant differences between the TP and control groups regarding behavioral inhibition, activation, and most dimensions of QoL, except for environmental health. These differences were observed across the test stages, group membership, and their interaction effects (P<0.05). The effect sizes for TP on physical, mental, and social health, overall QoL, and behavioral inhibition and activation ranged from 0.57 to 0.90 for the interaction of test and group membership. Table 4 presents the results of the Bonferroni post hoc test for mean comparisons across the test stages and groups.
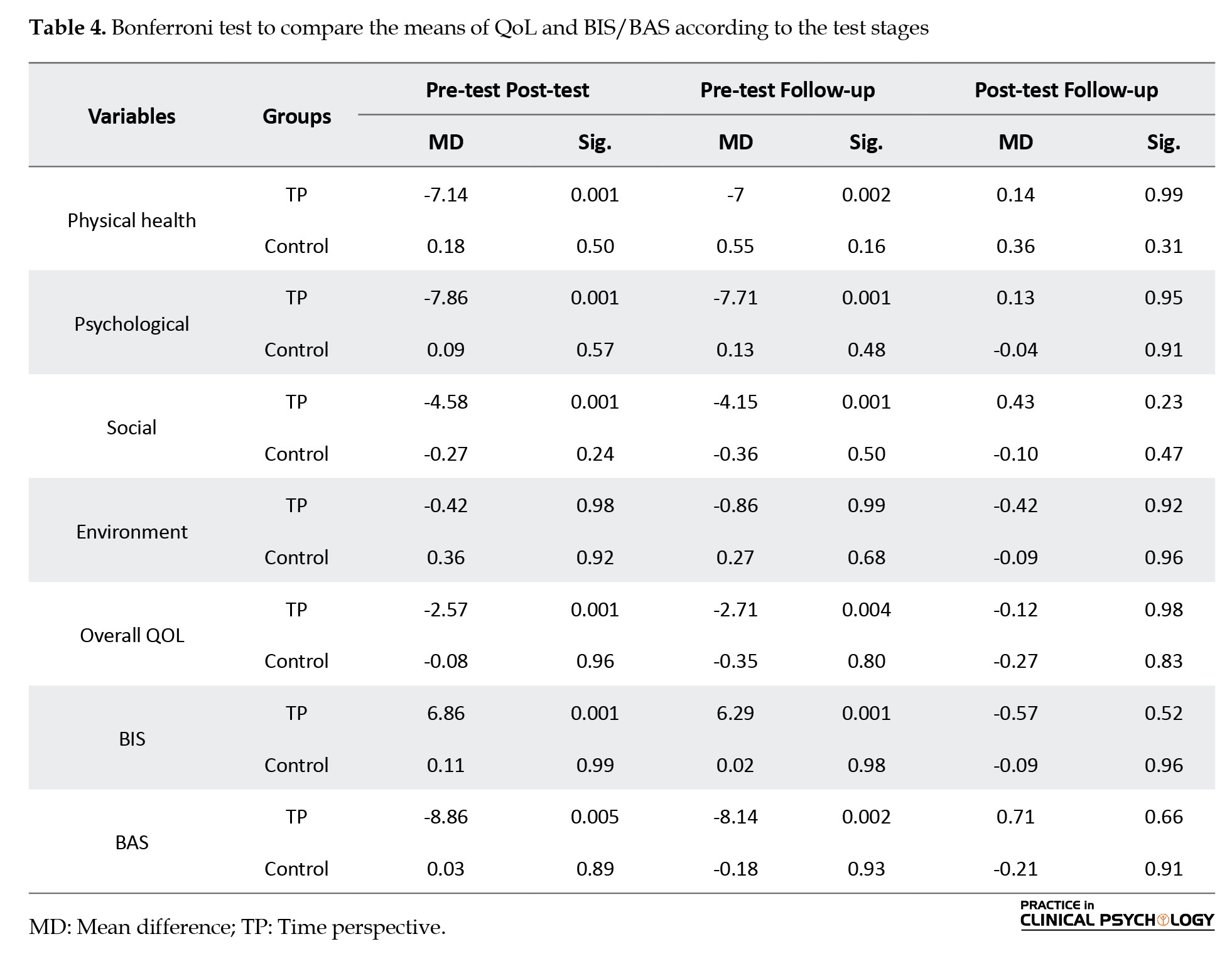
The data in Table 4 reveal that, within the TP group, significant changes were observed in the average scores for behavioral inhibition and activation and all dimensions of QoL, except for environmental health, from pre-test to post-test and pre-test to follow-up (P<0.05). However, no significant differences were observed between the post-test and follow-up stages (P<0.05). In contrast, the control group showed no significant changes across the test stages (P<0.05). These findings support the study’s hypothesis regarding the effectiveness of TP on various dimensions of QoL and brain and behavioral systems.
Discussion
The findings indicated that the TP intervention significantly influenced behavioral inhibition and activation in obese women. This outcome aligns with previous research findings (Germano & Brenlla, 2021; Moon et al., 2023; Zancu et al., 2024). Several key points should be considered to explain the effect of the TP intervention on reducing behavioral inhibition in obese women: According to Gray’s theory of behavior and brain function (Carver & White, 1994), the BIS inhibits behaviors that may result in negative or painful outcomes. Consequently, activation of the BIS restrains goal-directed actions. Gray further noted that the BIS is responsible for eliciting negative emotions such as fear, anxiety, frustration, and sadness in response to relevant signals and cues. Regarding individual personality differences, greater sensitivity of the BIS is associated with increased anxiety levels. The current study revealed that obese and overweight women exhibit relatively high levels of behavioral inhibition. Participants reported experiencing above-average fear, worry, and anxiety regarding criticism, blame from others, and their mistakes. These concerns were significantly associated with evaluation and judgment by others, as well as fear and anxiety about poor performance. Post-intervention, the average behavioral inhibition among participants decreased to below-average levels. This finding is crucial because excessively low behavioral inhibition can result in a diminished response to punishment signals, potentially leading to disorders, such as attention deficit/hyperactivity disorder. Specifically, individuals with a deterministic present perspective exhibit greater deficiencies in executive functions, including behavioral inhibition, due to heightened stress levels (Witowska & Zajenkowski, 2019).
The current study’s findings indicate that a TP-based psychotherapy intervention effectively increased the behavioral activation system (BAS) activity. The BAS, also known as the behavioral approach system, is a key component of the brain and behavioral systems, though its neurological basis is less well understood than the BIS. This system is believed to be responsive to reward signals and the avoidance of punishment, driving individuals towards goal-directed behaviors. According to Gray’s theory, the BAS is responsible for positive emotions such as hope, euphoria, and happiness. Individual personality differences suggest that higher sensitivity of the BAS correlates with a greater propensity to engage in goal-oriented efforts and experience positive emotions in anticipation of rewards. The present study found that the mean BAS activation scores of obese and overweight women were moderately low before the intervention. Most participants initially had moderate scores in drive-seeking behaviors (the desire to pursue and achieve goals), excitement (the desire for new experiences), and reward-responsiveness (continuing activities and experiencing positive emotions upon achieving goals). Following the TP-based psychotherapy intervention, these scores increased to above-average levels, but not excessively. This finding is significant because, according to Gray’s theory, an overactive BAS can lead to heightened responses to reward signals, potentially resulting in behavioral disorders. During TP psychotherapy, individuals learn to explore both positive and negative perspectives. In a positive future perspective, individuals practice future planning, which, along with an attitude shift, fosters greater readiness to pursue goals and welcome new experiences. This positive outlook can help sustain individuals’ engagement in tasks and activities, reducing the impact of temporary failures on their commitment to goals. Consequently, such interventions lead to increased BAS activity.
The results demonstrated that the TP-based intervention significantly improved QoL in obese women. This outcome aligns with the findings of several prior studies (Davis et al., 2024; Li & Tien, 2024). To interpret the findings, the study discusses the impact of TP on various health domains, including physical, mental, social, and environmental health, as well as overall QoL.
The results indicated that TP-based psychotherapy significantly influences participants’ physical health. This relationship can be understood by connecting time orientation and physical activity engagement. An individual’s decision to engage in a particular behavior often depends on the anticipated outcomes. According to social learning theories, outcome expectancies are shaped by evaluating the likelihood and motivation of these outcomes (Maddux, 1999). For many health behaviors, such as exercising or maintaining a healthy diet, the benefits, such as reduced risks of heart disease and cancer, may manifest in the distant future. These activities may also involve short-term sacrifices or discomforts. How individuals value future benefits versus immediate pleasure influences their behavior expectations (Bandura, 1991). Some individuals with a long-term perspective prioritize future health and engage in behaviors to safeguard it. Conversely, others may undervalue future health, believing they are either not at risk, can mitigate adverse effects later, or have time to correct their behaviors before consequences occur. Outcome expectations differ between near-term and distant outcomes (Guthrie et al., 2013). Since health education often aims to motivate individuals to adopt behaviors that yield future health benefits, understanding TPs is crucial for designing effective health-promoting interventions. TP interventions encourage individuals to weigh physical activity’s short-term and long-term benefits and drawbacks. These assessments can help individuals shift from a hedonic present orientation to a positive future outlook, leading to better planning and goal-setting for physical activity regulation.
Another key finding was the positive impact of TP psychotherapy on mental health. This effectiveness can be attributed to several factors: First, respectful treatment, effective communication through active listening, and a collaborative intervention environment encouraged participants to re-evaluate and reinterpret their memories in a safe, trustworthy setting. The techniques employed in this study likely assisted individuals in realistically assessing their past, present, and future continuities. Focusing on positive experiences across different timeframes helped participants shift their perspectives, transforming negative views of the past, present, and future into positive ones. By guiding individuals to focus on a transcendent future, the intervention fostered a more positive outlook on life and encouraged then to view problems as natural and developmental aspects of life. Future-oriented TP techniques emphasize personal capabilities and potential, promoting a life filled with meaning and self-acceptance. One of the core elements of this approach is self-acceptance, which involves embracing both positive and negative aspects of oneself. This acceptance also fosters self-compassion, enabling obese and overweight women to cease self-blame and adopt a responsible, committed approach to alleviating their suffering. Therefore, this intervention likely reduced worries and anxieties and improved mental health by reshaping participants’ self-perception, emphasizing the importance of past experiences, effective use of the present, and purposeful future planning.
The study’s results also demonstrated that TP-based psychotherapy significantly improved the social health of obese and overweight women. This finding can be interpreted from several aspects. The primary objective of TP-based therapy is to help individuals achieve a balanced TP, which integrates past, present, and future orientations healthily. A balanced TP can reduce social anxiety and enhance individuals’ engagement and enjoyment of social interactions (Stout et al., 2024).
Although limited, some research indicates a significant association between TP domains and social health-related constructs such as loneliness (Stout et al., 2024; Dąbrowska et al., 2022). For instance, one study found significant correlations between various temporal dimensions (past-negative, past-positive, and present-deterministic) and adolescent loneliness. Adolescents with a more negative view of the past and those focused on short-term positive experiences reported more loneliness symptoms. In contrast, those with a more positive past view experienced fewer loneliness symptoms (Dąbrowska et al., 2022). In line with these findings, the current study suggests that individuals who tend to (a) plan and think ahead, (b) look back on their past fondly, and (c) enjoy the present in a balanced manner are more likely to be satisfied with their social relationships and support. TP-based psychotherapy likely enhances self-reported social well-being by encouraging planning, finding positivity in past experiences, and mindful present usage.
The findings concerning the impact of TP on QoL components indicated that the TP intervention did not significantly affect environmental health. A comparative analysis with existing studies revealed that this specific effect has not been previously examined. The lack of significant impact can be attributed to several factors, primarily related to the measurement tool and questions in the Environmental Health Index. Most questions within this index pertain to aspects beyond the control of individuals, such as the healthiness of the surrounding environment, access to daily information, availability of health services, and transportation conditions.
Conclusion
In conclusion, this study demonstrated that TP interventions significantly influence behavioral inhibition, activation, and various dimensions of QoL. These findings underscore the potential of TP-based psychotherapy as an effective approach to improving both psychological and physiological well-being among obese and overweight women. However, the intervention did not yield significant changes in environmental health, suggesting the need for future research to explore this dimension further and potentially identify factors beyond individual control that may impact QoL.
Recommendations
Based on the findings of this study, it is recommended that healthcare providers and mental health professionals incorporate TP-based psychotherapy interventions into treatment programs for obese and overweight women. These interventions can effectively enhance behavioral activation and inhibition and improve QoL dimensions. Training sessions for practitioners should emphasize techniques that help patients develop a balanced TP, integrating positive past experiences, mindful present awareness, and constructive future planning. Additionally, public health initiatives could promote awareness of the benefits of TP interventions, encouraging individuals to adopt these practices as part of a holistic approach to health and well-being. Further research should explore ways to address environmental health through TP strategies, ensuring comprehensive care for this population.
Practical implications
The results of this study highlight the potential of TP-based interventions as a complementary approach to psychological care for obese and overweight women. Given the sustained improvements observed in both QoL and brain-behavioral systems, such interventions can serve as a valuable addition to multidisciplinary obesity management programs. Mental health professionals can integrate TP techniques into cognitive-behavioral frameworks to foster emotional regulation, motivation, and long-term behavioral changes. Additionally, healthcare systems should consider offering structured TP training as part of preventive and supportive care in weight management clinics. These findings suggest that community-based programs and wellness workshops can benefit beyond clinical settings by incorporating time-orientation strategies to support healthier lifestyle choices and psychological resilience in at-risk populations. Importantly, these implications extend to policy-level planning, where mental health promotion strategies for obesity can be enriched by acknowledging the temporal dimensions of self-perception and behavior change.
Research limitations
This study had several limitations. The small sample size and limited number of intervention sessions (six) restricted the generalizability of the findings. Additionally, the study’s scope was confined to a single city, which may not accurately represent the broader population. The self-reported nature of the data could introduce bias and affect the reliability of our results. Finally, the short follow-up period might have limited our ability to capture the long-term effects of the intervention. Future research should address these limitations by including larger, more diverse samples, extending the number of sessions, and incorporating longer follow-up periods to better assess the sustainability of the observed outcomes.
Future research
For future research, it is recommended to explore the long-term effects of TP interventions on behavioral inhibition and activation and various dimensions of QoL. Future studies should consider larger and more diverse sample sizes to enhance generalizability. Additionally, extending the duration and frequency of intervention sessions could provide deeper insights into the sustained impact of these interventions. Investigating the underlying mechanisms through which TP influences QoL and brain behavioral systems is crucial. Furthermore, examining the role of cultural, socioeconomic, and environmental factors in shaping the effectiveness of TP interventions can contribute to a more comprehensive understanding of their applicability to different populations. Future research should incorporate mixed-methods approaches to capture quantitative and qualitative data, providing a holistic view of the intervention’s impact.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by Ethics Committee of the Bojnourd Branch, Islamic Azad University, Bojnourd, Iran (Code: IR.IAU.BOJNOURD.REC.1402.005), and was conducted in full compliance with applicable guidelines and regulatory standards.
Funding
This research received no specific grants or financial support from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, methodology, investigation, review and editing: All authors; Writing the original draft: Afsaneh Ajhdari; Supervision: Ali-Akbar Soleimaniana and Hamid Darrodi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank the participants for their valuable time and commitment to this study. Special thanks are also extended to the staff of the Amin Counseling Center at the Islamic Azad University, Bojnourd Branch, Bojnourd, Iran, for their support and cooperation throughout the research process.
References
Iren Jaison, K., Asharaf, H., Thimothy, G., George, S., Jose, J., & Paily, R., et al. (2024). Psychological impact of obesity: A comprehensive analysis of health-related quality of life and weight-related symptoms. Obesity Medicine, 45, 100530. [DOI:10.1016/j.obmed.2023.100530]
Bandura, A. (1991). Social cognitive theory of self-regulation. Organizational Behavior and Human Decision Processes, 50(2), 248-287. [DOI:10.1016/0749-5978(91)90022-L]
Bonomi, A. E., Patrick, D. L., Bushnell, D. M., & Martin, M. (2000). Validation of the United States’ version of the world health organization quality of life (WHOQOL) instrument. Journal of Clinical Epidemiology, 53(1), 1-12. [DOI:10.1016/S0895-4356(99)00123-7] [PMID]
Carver, C. S., & White, T. L. (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS scales. Journal of Personality and Social Psychology, 67(2), 319-333. [DOI:10.1037/0022-3514.67.2.319]
Cho, J. H., Jae, S. Y., Choo, I. L., & Choo, J. (2014). Health-promoting behaviour among women with abdominal obesity: A conceptual link to social support and perceived stress. Journal of Advanced Nursing, 70(6), 1381–1390. [DOI:10.1111/jan.12300] [PMID]
Dąbrowska, A., Marek-Banach, J., Zimbardo, P., Łopatkiewicz, A., & Wysocka, E. (2022). Time perspective and experience of depression, stress, and loneliness among adolescents in youth educational centres. Przegląd Badań Edukacyjnych= Educational Studies Review, 1(36), 91-119. [DOI:10.12775/PBE.2022.005]
Davis, P. A., Trotter, M., Åström, E., & Rönnlund, M. (2024). Balancing time for health behaviors: Associations of time perspective with physical activity and weight management in older adults. American Journal of Health Promotion: AJHP, 38(7), 960–969. [DOI:10.1177/08901171241242546] [PMID]
De Hert, M., Correll, C. U., Bobes, J., Cetkovich-Bakmas, M., Cohen, D., & Asai, I., et al. (2011). Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry: Official Journal of the World Psychiatric Association (WPA), 10(1), 52–77. [DOI:10.1002/j.2051-5545.2011.tb00014.x] [PMID]
Ebrahimi, F., Kiamarsi, A., & Taklavi, S. (2023). [The effectiveness of time perspective therapy on physical self-concept and psychological helplessness in postmenopausal women (Persian)]. Rooyesh-e-Ravanshenasi Journal (RRJ), 12(5), 109-118. [Link]
Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. [DOI:10.3758/BRM.41.4.1149] [PMID]
Germano, G., & Brenlla, M. E. (2021). Effects of time perspective and self-control on psychological distress: A cross-sectional study in an Argentinian sample. Personality and Individual Differences, 171, 110512. [DOI:10.1016/j.paid.2020.110512]
Golmohammadi, M., Attari, V. E., Salimi, Y., Nachvak, S. M., & Samadi, M. (2024). The effect of MIND diet on sleep status, anxiety, depression, and cardiometabolic indices in obese diabetic women with insomnia: study protocol for a randomized controlled clinical trial {1}. Trials, 25(1), 660. [DOI:10.1186/s13063-024-08486-y] [PMID]
González-Fernández, E., Xandri-Martínez, R., Gómez-Díaz, M., & Navas-López, J. (2024). Nutritional and psychosocial intervention to improve the self-concept of body image and increase the self-esteem of overweight and obese individuals: A quasi-experimental study. Nutrients, 16(16), 2708. [DOI:10.3390/nu16162708] [PMID]
Guthrie, L. C., Lessl, K., Ochi, O., & Ward, M. M. (2013). Time perspective and smoking, obesity, and exercise in a community sample. American Journal of Health Behavior, 37(2), 171-180. [DOI:10.5993/AJHB.37.2.4] [PMID]
Elmaleh-Sachs, A., Schwartz, J. L., Bramante, C. T., Nicklas, J. M., Gudzune, K. A., & Jay, M. (2023). Obesity management in adults: A review. JAMA, 330(20), 2000–2015. [DOI:10.1001/jama.2023.19897] [PMID]
Hajek, A., Kretzler, B., & König, H. H. (2021). The association between obesity and social isolation as well as loneliness in the adult population: A systematic review. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 14, 2765–2773. [DOI:10.2147/DMSO.S313873] [PMID]
Hemmati, M., Tizdast, T., & Jadidi, M. (2025). [The efficacy of an integrated training package based on time perspective therapy and positive therapy on the quality of life and psychological well-being of depressed patients (Persian)]. Journal of Psychological Science, 24(145), 97-118. [Link]
Hosseini, M., Arefi, M., & Sajjadian, I. (2020). [Time perspective training package on balancing time and anxiety of students (Persian)]. Middle Eastern Journal of Disability Studies, 10, 15. [Link]
Kahn, S. R., Julian, J. A., Kearon, C., Gu, C. S., Cohen, D. J., & Magnuson, E. A., et al. (2020). Quality of life after pharmacochemical catheter-directed thrombolysis for proximal deep venous thrombosis. Journal of Vascular Surgery: Venous and Lymphatic Disorders, 8(1), 8-23. [DOI:10.1016/j.jvsv.2019.03.023] [PMID]
Kern, D., Busch, A., Schneider, K. L., Miller, S. A., Appelhans, B. M., & Waring, M. E., et al. (2019). Psychosocial factors associated with treatment outcomes in women with obesity and major depressive disorder who received behavioral activation for depression. Journal of Behavioral Medicine, 42(3), 522–533. [DOI:10.1007/s10865-018-9993-9] [PMID]
Kulie, T., Slattengren, A., Redmer, J., Counts, H., Eglash, A., & Schrager, S. (2011). Obesity and women's health: An evidence-based review. Journal of the American Board of Family Medicine: JABFM, 24(1), 75–85. [DOI:10.3122/jabfm.2011.01.100076] [PMID]
Li, T. T., & Tien, H. L. S. (2024). The relationship between time perspective and life satisfaction: career adaptability as an intermediate variable1. British Journal of Guidance & Counselling, 52(3), 537-545. [DOI:10.1080/03069885.2023.2224930]
Lingvay, I., Cohen, R. V., le Roux, C. W., & Sumithran, P. (2024). Obesity in adults. The Lancet, 404(10456), 972-987. [DOI:10.1016/S0140-6736(24)01210-8] [PMID]
Maddux, J. E. (1999). Expectancies and the social-cognitive perspective: Basic principles, processes, and variables. In I. Kirsch (Ed.), How expectancies shape experience (pp. 17-39). Washington: American Psychological Association. [DOI:10.1037/10332-001]
Malekiha, M., & Moradi, B. (2019). [Effectiveness of time perspective therapy on increasing psychological well-being and happiness in veterans with PTSD (Persian)]. Iranian Journal of War and Public Health, 11(3), 153-159. [DOI:10.29252/ijwph.11.3.153]
Mohammadi, N. (2008). [The psychometric properties of the behavioral inhibition system (BIS) and behavioral activation system (BAS) scales among students of Shiraz University (Persian)]. Clinical Psychology and Personality, 6(1), 61-68. [Link]
Moon, J., Lieber, R. J., Bayazitli, I., & Mello, Z. R. (2023). An examination of multidimensional time perspective and mental health outcomes. International Journal of Environmental Research and Public Health, 20(6), 4688. [DOI:10.3390/ijerph20064688] [PMID]
Mousavi, S. N., Hasanzadeh, R., & Dousti, Y. (2019). [Effectiveness of time perspective therapy on depression and social well-being of bereaved women (Persian)]. Journal of Research in Behavioural Sciences, 17(2), 205-213. [DOI:10.52547/rbs.17.2.205]
GBD 2019 Risk Factors Collaborators (2020). Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet (London, England), 396(10258), 1223–1249. [DOI:10.1016/S0140-6736(20)30752-2] [PMID]
Nejat, S., Montazeri, A., Holakouie Naieni, K., Mohammad, K., & Majdzadeh, S. (2006). [The World Health Organization quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version (Persian)]. Journal of School of Public Health and Institute of Public Health Research, 4(4), 1-12. [Link]
Rahimpour, S., Arefi, M., & Manshaii, G. R. (2021). [The effectiveness of mixed method of time perspective and mindfulness education on resilience and wisdom (Persian)]. Positive Psychology Research, 7(1), 35-52. [DOI:10.22108/ppls.2021.118779.1798]
Remington, G. (2006). Schizophrenia, antipsychotics, and the metabolic syndrome: Is there a silver lining? American Journal of Psychiatry, 163(7), 1132-1134. [DOI:10.1176/ajp.2006.163.7.1132] [PMID]
Saruco, E., & Pleger, B. (2021). A systematic review of obesity and binge eating associated impairment of the cognitive inhibition system. Frontiers in Nutrition, 8, 609012. [DOI:10.3389/fnut.2021.609012] [PMID]
Sarwer, D. B., & Polonsky, H. M. (2016). Body image and body contouring procedures. Aesthetic Surgery Journal, 36(9), 1039-1047. [DOI:10.1093/asj/sjw127] [PMID]
Shafiee, A., Nayebirad, S., Najafi, M. S., Jalali, A., Alaeddini, F., & Saadat, S., et al. (2023). Prevalence of obesity and overweight in an adult population of Tehran metropolis. Journal of Diabetes and Metabolic Disorders, 23(1), 895–907. [DOI:10.1007/s40200-023-01365-4] [PMID]
Stout, M. E., Medlin, A. R., Gupta, R., & Tsotsoros, C. E. (2024). Time perspective and perceived social isolation: The role of social interaction anxiety. Healthcare (Basel, Switzerland), 12(17), 1736. [DOI:10.3390/healthcare12171736] [PMID]
Whoqol Group. (1995). The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Social Science & Medicine, 41(10), 1403-1409. [DOI:10.1016/0277-9536(95)00112-K] [PMID]
Witowska, J., & Zajenkowski, M. (2018). How is perception of time associated with cognitive functioning? The relationship between time perspective and executive control. Time & Society, 28(3), 1124-1147. [DOI:10.1177/0961463X18763693]
Zancu, S. A., Măirean, C., & Diaconu-Gherasim, L. R. (2022). The longitudinal relation between time perspective and preventive behaviors during the COVID-19 pandemic: The mediating role of risk perception. Current Psychology, 43, 12981-12989. [PMID]
Zimbardo, P. (2002). Just think about it: Time to take our time. Looking to the future is important and very American-but living in the present is vital. Psychology Today, 35, 62. [Link]
Zimbardo, P. G., & Boyd, J. N. (2014). Putting time in perspective: A valid, reliable individual-differences metric. In M. Stolarski, N. Fieulaine& W. van Beek (Eds), Time Perspective Theory; Review, Research and Application. Cham: Springer.[DOI:10.1007/978-3-319-07368-2_2]
Inclusion and exclusion criteria
The inclusion criteria included absence of a mental disorder (self-reported), not being pregnant, a body mass index greater than 24, willingness to participate in the study, having at least a high school diploma, and being within the age range of 18 to 48 years. The exclusion criteria included missing more than one session, not completing assigned tasks, and taking certain medications.
Procedures
To recruit participants, a public announcement was disseminated under the title “Free group therapy for obese and overweight women.” The announcement included a brief introduction to the facilitator’s background and qualifications and an overview of the intervention, which was described as a TP psychotherapy program. The advertisement outlined the potential psychological and emotional benefits of participation and clearly stated that the program was offered free of charge. The eligibility criteria were specified, and it was emphasized that both students and non-students who met these criteria were welcome to participate. The recruitment strategy aimed to ensure broad accessibility and encourage voluntary participation by women in the target population. Data were collected using the WHO QoL questionnaire (WHOQOL-BREF) and the behavioral inhibition and activation system scales (BIS/BAS).
QoL questionnaire
The present study utilized the WHO QoL questionnaire (WHOQOL-BREF) as one of its instruments. This questionnaire assesses various domains of individuals’ QoL using 26 items. It comprises four subscales: Physical health (items 3, 4, 10, 15, 16, 17, and 18), psychological health (items 5, 6, 7, 11, 19, and 26), social relationships (items 20, 21, and 22), environment (items 8, 9, 12, 13, 14, 23, 24, 25), and overall QoL (items 1 and 2). Higher scores indicate better QoL in the respective domains (WHOQOL Group, 1995). Bonomi reported an internal reliability of 0.95 for the test in his study (Bonomi et al., 2000). This questionnaire, designed and translated in 2000 across 15 countries, underwent standardization, translation, and psychometric testing of the Persian version by Nejat et al. (2006). To assess its validity and reliability, the questionnaire was administered to 1,167 individuals from Tehran, divided into two groups with chronic and non-chronic diseases. The test re-test reliability for the subscales was as follows: Physical health, 0.77; mental health, 0.77; social relationships, 0.75; and environmental health, 0.84.
BIS/BAS
Another instrument utilized in this study was the BIS/BAS, designed by Carver and White in 1994. This self-report questionnaire measures responses on a four-point Likert scale ranging from “strongly agree” to “strongly disagree,” with scores ranging from 1 to 4. The questionnaire comprises 20 items and two primary factors: Inhibition (seven items) and activation (13 items). The activation factor comprises three components: Drive (four items), fun-seeking (four items), and reward responsiveness (five items). The inhibition factor also includes sensitivity to the behavioral inhibition system (BIS) (seven items). The reported Cronbach’s α coefficients are 0.74 for the inhibition scale, and for the activation scales—reward, drive, and fun seeking—they are 0.73, 0.76, and 0.66, respectively (Carver & White, 1994). The psychometric properties of this scale were evaluated with the student population at Shiraz University, revealing good validity and reliability. The correlation coefficients for the behavioral inhibition scale with depression and anxiety were found to be significant at 0.22 and 0.31, respectively. Examination of the internal consistency showed Cronbach’s α coefficients of 0.69 for the inhibition scale, 0.78 for the total activation score, and 0.87, 0.74, and 0.65 for its three subscales—drive, reward, and fun seeking, respectively. The test re-test reliability over two weeks yielded coefficients of 0.71 for the inhibition scale, 0.73 for the total activation score, and 0.62 and 0.71 for the drive, reward, and fun-seeking subscales, respectively, all of which were significant (Mohammadi, 2008).
TP intervention plan
The TP intervention was implemented based on the training protocol developed by Zimbardo and Boyd (2014). The program consisted of six structured sessions, each lasting approximately one hour and conducted once per week. The intervention was designed to help participants recognize and adjust their cognitive and emotional orientations toward time, to foster a more balanced TP. The sessions included a combination of psychoeducation, guided mental imagery exercises focusing on positive and negative past experiences, motivational enhancement strategies, mindfulness and breathing techniques, and practical activities to increase future-oriented thinking while reducing over-reliance on past-negative and present-fatalistic perspectives.
The content and structure of the sessions were adapted to the needs of overweight and obese women, with an emphasis on improving psychological well-being and enhancing self-regulation. Each session built upon the previous one, encouraging reflection and behavioral integration of TP concepts into daily life. Table 1 presents the details of the intervention in the experimental group.
Data analysis
Data analysis encompassed descriptive (Mean±SD) and inferential statistical (mixed analysis of variance) methods.
Results
Descriptive results
The demographic analysis revealed that the average age of participants in the experimental group was 32.57±9.78 years, while the control group had an average age of 36.91±7.36 years. Additionally, 71.43% of individuals in the experimental group and 63.64% in the control group held a bachelor’s degree. Employment status was distributed as follows: In the experimental group, 42.86% were students, 14.29% were employed, and 42.86% were housewives; in the control group, 54.54% were employed and 45.46% were housewives. Regarding marital status, 42.86% of the experimental group were married with children, whereas all participants in the control group were married with children. The mean BMI was 30.06 in the experimental group and 28.72 in the control group. Statistical analyses showed no significant differences in age, employment status, education level, or BMI (P<0.05). However, chi-square test results indicated a significant difference in marital status and childbearing between the groups (χ2=11.67 (4), P<0.05).
Table 2 presents the Mean±SD of the QoL variables and behavioral brain systems across the pre-test, post-test, and follow-up stages, for both the experimental and control groups.
Analysis of Table 2 indicates that the mean scores for QoL and behavioral inhibition and activation in the experimental group improved from the pre-test to the post-test stage. Specifically, post-test mean scores for QoL and behavioral activation increased, while mean scores for behavioral inhibition decreased.
Repeated measures analysis of variance (ANOVA)
Before the repeated measures analysis of variance, the assumptions underlying this parametric test were evaluated. The Shapiro-Wilk test confirmed normality by group (P<0.05). Levene’s test verified the homogeneity of variances (P<0.05). However, the Mauchly test suggested that the sphericity assumption was not met for the variables of physical health, overall QoL, and behavioral activation (P<0.05); thus, the Greenhouse-Geiser correction was applied.
The Wilks’ Lambda test yielded significant results for test stages, group membership, and the interaction between test stages and group membership (P<0.01). Table 3 presents the detailed outcomes of the repeated measures analysis of variance for QoL and behavioral inhibition/activation dimensions.
Table 3 reveals significant differences between the TP and control groups regarding behavioral inhibition, activation, and most dimensions of QoL, except for environmental health. These differences were observed across the test stages, group membership, and their interaction effects (P<0.05). The effect sizes for TP on physical, mental, and social health, overall QoL, and behavioral inhibition and activation ranged from 0.57 to 0.90 for the interaction of test and group membership. Table 4 presents the results of the Bonferroni post hoc test for mean comparisons across the test stages and groups.
The data in Table 4 reveal that, within the TP group, significant changes were observed in the average scores for behavioral inhibition and activation and all dimensions of QoL, except for environmental health, from pre-test to post-test and pre-test to follow-up (P<0.05). However, no significant differences were observed between the post-test and follow-up stages (P<0.05). In contrast, the control group showed no significant changes across the test stages (P<0.05). These findings support the study’s hypothesis regarding the effectiveness of TP on various dimensions of QoL and brain and behavioral systems.
Discussion
The findings indicated that the TP intervention significantly influenced behavioral inhibition and activation in obese women. This outcome aligns with previous research findings (Germano & Brenlla, 2021; Moon et al., 2023; Zancu et al., 2024). Several key points should be considered to explain the effect of the TP intervention on reducing behavioral inhibition in obese women: According to Gray’s theory of behavior and brain function (Carver & White, 1994), the BIS inhibits behaviors that may result in negative or painful outcomes. Consequently, activation of the BIS restrains goal-directed actions. Gray further noted that the BIS is responsible for eliciting negative emotions such as fear, anxiety, frustration, and sadness in response to relevant signals and cues. Regarding individual personality differences, greater sensitivity of the BIS is associated with increased anxiety levels. The current study revealed that obese and overweight women exhibit relatively high levels of behavioral inhibition. Participants reported experiencing above-average fear, worry, and anxiety regarding criticism, blame from others, and their mistakes. These concerns were significantly associated with evaluation and judgment by others, as well as fear and anxiety about poor performance. Post-intervention, the average behavioral inhibition among participants decreased to below-average levels. This finding is crucial because excessively low behavioral inhibition can result in a diminished response to punishment signals, potentially leading to disorders, such as attention deficit/hyperactivity disorder. Specifically, individuals with a deterministic present perspective exhibit greater deficiencies in executive functions, including behavioral inhibition, due to heightened stress levels (Witowska & Zajenkowski, 2019).
The current study’s findings indicate that a TP-based psychotherapy intervention effectively increased the behavioral activation system (BAS) activity. The BAS, also known as the behavioral approach system, is a key component of the brain and behavioral systems, though its neurological basis is less well understood than the BIS. This system is believed to be responsive to reward signals and the avoidance of punishment, driving individuals towards goal-directed behaviors. According to Gray’s theory, the BAS is responsible for positive emotions such as hope, euphoria, and happiness. Individual personality differences suggest that higher sensitivity of the BAS correlates with a greater propensity to engage in goal-oriented efforts and experience positive emotions in anticipation of rewards. The present study found that the mean BAS activation scores of obese and overweight women were moderately low before the intervention. Most participants initially had moderate scores in drive-seeking behaviors (the desire to pursue and achieve goals), excitement (the desire for new experiences), and reward-responsiveness (continuing activities and experiencing positive emotions upon achieving goals). Following the TP-based psychotherapy intervention, these scores increased to above-average levels, but not excessively. This finding is significant because, according to Gray’s theory, an overactive BAS can lead to heightened responses to reward signals, potentially resulting in behavioral disorders. During TP psychotherapy, individuals learn to explore both positive and negative perspectives. In a positive future perspective, individuals practice future planning, which, along with an attitude shift, fosters greater readiness to pursue goals and welcome new experiences. This positive outlook can help sustain individuals’ engagement in tasks and activities, reducing the impact of temporary failures on their commitment to goals. Consequently, such interventions lead to increased BAS activity.
The results demonstrated that the TP-based intervention significantly improved QoL in obese women. This outcome aligns with the findings of several prior studies (Davis et al., 2024; Li & Tien, 2024). To interpret the findings, the study discusses the impact of TP on various health domains, including physical, mental, social, and environmental health, as well as overall QoL.
The results indicated that TP-based psychotherapy significantly influences participants’ physical health. This relationship can be understood by connecting time orientation and physical activity engagement. An individual’s decision to engage in a particular behavior often depends on the anticipated outcomes. According to social learning theories, outcome expectancies are shaped by evaluating the likelihood and motivation of these outcomes (Maddux, 1999). For many health behaviors, such as exercising or maintaining a healthy diet, the benefits, such as reduced risks of heart disease and cancer, may manifest in the distant future. These activities may also involve short-term sacrifices or discomforts. How individuals value future benefits versus immediate pleasure influences their behavior expectations (Bandura, 1991). Some individuals with a long-term perspective prioritize future health and engage in behaviors to safeguard it. Conversely, others may undervalue future health, believing they are either not at risk, can mitigate adverse effects later, or have time to correct their behaviors before consequences occur. Outcome expectations differ between near-term and distant outcomes (Guthrie et al., 2013). Since health education often aims to motivate individuals to adopt behaviors that yield future health benefits, understanding TPs is crucial for designing effective health-promoting interventions. TP interventions encourage individuals to weigh physical activity’s short-term and long-term benefits and drawbacks. These assessments can help individuals shift from a hedonic present orientation to a positive future outlook, leading to better planning and goal-setting for physical activity regulation.
Another key finding was the positive impact of TP psychotherapy on mental health. This effectiveness can be attributed to several factors: First, respectful treatment, effective communication through active listening, and a collaborative intervention environment encouraged participants to re-evaluate and reinterpret their memories in a safe, trustworthy setting. The techniques employed in this study likely assisted individuals in realistically assessing their past, present, and future continuities. Focusing on positive experiences across different timeframes helped participants shift their perspectives, transforming negative views of the past, present, and future into positive ones. By guiding individuals to focus on a transcendent future, the intervention fostered a more positive outlook on life and encouraged then to view problems as natural and developmental aspects of life. Future-oriented TP techniques emphasize personal capabilities and potential, promoting a life filled with meaning and self-acceptance. One of the core elements of this approach is self-acceptance, which involves embracing both positive and negative aspects of oneself. This acceptance also fosters self-compassion, enabling obese and overweight women to cease self-blame and adopt a responsible, committed approach to alleviating their suffering. Therefore, this intervention likely reduced worries and anxieties and improved mental health by reshaping participants’ self-perception, emphasizing the importance of past experiences, effective use of the present, and purposeful future planning.
The study’s results also demonstrated that TP-based psychotherapy significantly improved the social health of obese and overweight women. This finding can be interpreted from several aspects. The primary objective of TP-based therapy is to help individuals achieve a balanced TP, which integrates past, present, and future orientations healthily. A balanced TP can reduce social anxiety and enhance individuals’ engagement and enjoyment of social interactions (Stout et al., 2024).
Although limited, some research indicates a significant association between TP domains and social health-related constructs such as loneliness (Stout et al., 2024; Dąbrowska et al., 2022). For instance, one study found significant correlations between various temporal dimensions (past-negative, past-positive, and present-deterministic) and adolescent loneliness. Adolescents with a more negative view of the past and those focused on short-term positive experiences reported more loneliness symptoms. In contrast, those with a more positive past view experienced fewer loneliness symptoms (Dąbrowska et al., 2022). In line with these findings, the current study suggests that individuals who tend to (a) plan and think ahead, (b) look back on their past fondly, and (c) enjoy the present in a balanced manner are more likely to be satisfied with their social relationships and support. TP-based psychotherapy likely enhances self-reported social well-being by encouraging planning, finding positivity in past experiences, and mindful present usage.
The findings concerning the impact of TP on QoL components indicated that the TP intervention did not significantly affect environmental health. A comparative analysis with existing studies revealed that this specific effect has not been previously examined. The lack of significant impact can be attributed to several factors, primarily related to the measurement tool and questions in the Environmental Health Index. Most questions within this index pertain to aspects beyond the control of individuals, such as the healthiness of the surrounding environment, access to daily information, availability of health services, and transportation conditions.
Conclusion
In conclusion, this study demonstrated that TP interventions significantly influence behavioral inhibition, activation, and various dimensions of QoL. These findings underscore the potential of TP-based psychotherapy as an effective approach to improving both psychological and physiological well-being among obese and overweight women. However, the intervention did not yield significant changes in environmental health, suggesting the need for future research to explore this dimension further and potentially identify factors beyond individual control that may impact QoL.
Recommendations
Based on the findings of this study, it is recommended that healthcare providers and mental health professionals incorporate TP-based psychotherapy interventions into treatment programs for obese and overweight women. These interventions can effectively enhance behavioral activation and inhibition and improve QoL dimensions. Training sessions for practitioners should emphasize techniques that help patients develop a balanced TP, integrating positive past experiences, mindful present awareness, and constructive future planning. Additionally, public health initiatives could promote awareness of the benefits of TP interventions, encouraging individuals to adopt these practices as part of a holistic approach to health and well-being. Further research should explore ways to address environmental health through TP strategies, ensuring comprehensive care for this population.
Practical implications
The results of this study highlight the potential of TP-based interventions as a complementary approach to psychological care for obese and overweight women. Given the sustained improvements observed in both QoL and brain-behavioral systems, such interventions can serve as a valuable addition to multidisciplinary obesity management programs. Mental health professionals can integrate TP techniques into cognitive-behavioral frameworks to foster emotional regulation, motivation, and long-term behavioral changes. Additionally, healthcare systems should consider offering structured TP training as part of preventive and supportive care in weight management clinics. These findings suggest that community-based programs and wellness workshops can benefit beyond clinical settings by incorporating time-orientation strategies to support healthier lifestyle choices and psychological resilience in at-risk populations. Importantly, these implications extend to policy-level planning, where mental health promotion strategies for obesity can be enriched by acknowledging the temporal dimensions of self-perception and behavior change.
Research limitations
This study had several limitations. The small sample size and limited number of intervention sessions (six) restricted the generalizability of the findings. Additionally, the study’s scope was confined to a single city, which may not accurately represent the broader population. The self-reported nature of the data could introduce bias and affect the reliability of our results. Finally, the short follow-up period might have limited our ability to capture the long-term effects of the intervention. Future research should address these limitations by including larger, more diverse samples, extending the number of sessions, and incorporating longer follow-up periods to better assess the sustainability of the observed outcomes.
Future research
For future research, it is recommended to explore the long-term effects of TP interventions on behavioral inhibition and activation and various dimensions of QoL. Future studies should consider larger and more diverse sample sizes to enhance generalizability. Additionally, extending the duration and frequency of intervention sessions could provide deeper insights into the sustained impact of these interventions. Investigating the underlying mechanisms through which TP influences QoL and brain behavioral systems is crucial. Furthermore, examining the role of cultural, socioeconomic, and environmental factors in shaping the effectiveness of TP interventions can contribute to a more comprehensive understanding of their applicability to different populations. Future research should incorporate mixed-methods approaches to capture quantitative and qualitative data, providing a holistic view of the intervention’s impact.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by Ethics Committee of the Bojnourd Branch, Islamic Azad University, Bojnourd, Iran (Code: IR.IAU.BOJNOURD.REC.1402.005), and was conducted in full compliance with applicable guidelines and regulatory standards.
Funding
This research received no specific grants or financial support from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, methodology, investigation, review and editing: All authors; Writing the original draft: Afsaneh Ajhdari; Supervision: Ali-Akbar Soleimaniana and Hamid Darrodi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank the participants for their valuable time and commitment to this study. Special thanks are also extended to the staff of the Amin Counseling Center at the Islamic Azad University, Bojnourd Branch, Bojnourd, Iran, for their support and cooperation throughout the research process.
References
Iren Jaison, K., Asharaf, H., Thimothy, G., George, S., Jose, J., & Paily, R., et al. (2024). Psychological impact of obesity: A comprehensive analysis of health-related quality of life and weight-related symptoms. Obesity Medicine, 45, 100530. [DOI:10.1016/j.obmed.2023.100530]
Bandura, A. (1991). Social cognitive theory of self-regulation. Organizational Behavior and Human Decision Processes, 50(2), 248-287. [DOI:10.1016/0749-5978(91)90022-L]
Bonomi, A. E., Patrick, D. L., Bushnell, D. M., & Martin, M. (2000). Validation of the United States’ version of the world health organization quality of life (WHOQOL) instrument. Journal of Clinical Epidemiology, 53(1), 1-12. [DOI:10.1016/S0895-4356(99)00123-7] [PMID]
Carver, C. S., & White, T. L. (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS scales. Journal of Personality and Social Psychology, 67(2), 319-333. [DOI:10.1037/0022-3514.67.2.319]
Cho, J. H., Jae, S. Y., Choo, I. L., & Choo, J. (2014). Health-promoting behaviour among women with abdominal obesity: A conceptual link to social support and perceived stress. Journal of Advanced Nursing, 70(6), 1381–1390. [DOI:10.1111/jan.12300] [PMID]
Dąbrowska, A., Marek-Banach, J., Zimbardo, P., Łopatkiewicz, A., & Wysocka, E. (2022). Time perspective and experience of depression, stress, and loneliness among adolescents in youth educational centres. Przegląd Badań Edukacyjnych= Educational Studies Review, 1(36), 91-119. [DOI:10.12775/PBE.2022.005]
Davis, P. A., Trotter, M., Åström, E., & Rönnlund, M. (2024). Balancing time for health behaviors: Associations of time perspective with physical activity and weight management in older adults. American Journal of Health Promotion: AJHP, 38(7), 960–969. [DOI:10.1177/08901171241242546] [PMID]
De Hert, M., Correll, C. U., Bobes, J., Cetkovich-Bakmas, M., Cohen, D., & Asai, I., et al. (2011). Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry: Official Journal of the World Psychiatric Association (WPA), 10(1), 52–77. [DOI:10.1002/j.2051-5545.2011.tb00014.x] [PMID]
Ebrahimi, F., Kiamarsi, A., & Taklavi, S. (2023). [The effectiveness of time perspective therapy on physical self-concept and psychological helplessness in postmenopausal women (Persian)]. Rooyesh-e-Ravanshenasi Journal (RRJ), 12(5), 109-118. [Link]
Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. [DOI:10.3758/BRM.41.4.1149] [PMID]
Germano, G., & Brenlla, M. E. (2021). Effects of time perspective and self-control on psychological distress: A cross-sectional study in an Argentinian sample. Personality and Individual Differences, 171, 110512. [DOI:10.1016/j.paid.2020.110512]
Golmohammadi, M., Attari, V. E., Salimi, Y., Nachvak, S. M., & Samadi, M. (2024). The effect of MIND diet on sleep status, anxiety, depression, and cardiometabolic indices in obese diabetic women with insomnia: study protocol for a randomized controlled clinical trial {1}. Trials, 25(1), 660. [DOI:10.1186/s13063-024-08486-y] [PMID]
González-Fernández, E., Xandri-Martínez, R., Gómez-Díaz, M., & Navas-López, J. (2024). Nutritional and psychosocial intervention to improve the self-concept of body image and increase the self-esteem of overweight and obese individuals: A quasi-experimental study. Nutrients, 16(16), 2708. [DOI:10.3390/nu16162708] [PMID]
Guthrie, L. C., Lessl, K., Ochi, O., & Ward, M. M. (2013). Time perspective and smoking, obesity, and exercise in a community sample. American Journal of Health Behavior, 37(2), 171-180. [DOI:10.5993/AJHB.37.2.4] [PMID]
Elmaleh-Sachs, A., Schwartz, J. L., Bramante, C. T., Nicklas, J. M., Gudzune, K. A., & Jay, M. (2023). Obesity management in adults: A review. JAMA, 330(20), 2000–2015. [DOI:10.1001/jama.2023.19897] [PMID]
Hajek, A., Kretzler, B., & König, H. H. (2021). The association between obesity and social isolation as well as loneliness in the adult population: A systematic review. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 14, 2765–2773. [DOI:10.2147/DMSO.S313873] [PMID]
Hemmati, M., Tizdast, T., & Jadidi, M. (2025). [The efficacy of an integrated training package based on time perspective therapy and positive therapy on the quality of life and psychological well-being of depressed patients (Persian)]. Journal of Psychological Science, 24(145), 97-118. [Link]
Hosseini, M., Arefi, M., & Sajjadian, I. (2020). [Time perspective training package on balancing time and anxiety of students (Persian)]. Middle Eastern Journal of Disability Studies, 10, 15. [Link]
Kahn, S. R., Julian, J. A., Kearon, C., Gu, C. S., Cohen, D. J., & Magnuson, E. A., et al. (2020). Quality of life after pharmacochemical catheter-directed thrombolysis for proximal deep venous thrombosis. Journal of Vascular Surgery: Venous and Lymphatic Disorders, 8(1), 8-23. [DOI:10.1016/j.jvsv.2019.03.023] [PMID]
Kern, D., Busch, A., Schneider, K. L., Miller, S. A., Appelhans, B. M., & Waring, M. E., et al. (2019). Psychosocial factors associated with treatment outcomes in women with obesity and major depressive disorder who received behavioral activation for depression. Journal of Behavioral Medicine, 42(3), 522–533. [DOI:10.1007/s10865-018-9993-9] [PMID]
Kulie, T., Slattengren, A., Redmer, J., Counts, H., Eglash, A., & Schrager, S. (2011). Obesity and women's health: An evidence-based review. Journal of the American Board of Family Medicine: JABFM, 24(1), 75–85. [DOI:10.3122/jabfm.2011.01.100076] [PMID]
Li, T. T., & Tien, H. L. S. (2024). The relationship between time perspective and life satisfaction: career adaptability as an intermediate variable1. British Journal of Guidance & Counselling, 52(3), 537-545. [DOI:10.1080/03069885.2023.2224930]
Lingvay, I., Cohen, R. V., le Roux, C. W., & Sumithran, P. (2024). Obesity in adults. The Lancet, 404(10456), 972-987. [DOI:10.1016/S0140-6736(24)01210-8] [PMID]
Maddux, J. E. (1999). Expectancies and the social-cognitive perspective: Basic principles, processes, and variables. In I. Kirsch (Ed.), How expectancies shape experience (pp. 17-39). Washington: American Psychological Association. [DOI:10.1037/10332-001]
Malekiha, M., & Moradi, B. (2019). [Effectiveness of time perspective therapy on increasing psychological well-being and happiness in veterans with PTSD (Persian)]. Iranian Journal of War and Public Health, 11(3), 153-159. [DOI:10.29252/ijwph.11.3.153]
Mohammadi, N. (2008). [The psychometric properties of the behavioral inhibition system (BIS) and behavioral activation system (BAS) scales among students of Shiraz University (Persian)]. Clinical Psychology and Personality, 6(1), 61-68. [Link]
Moon, J., Lieber, R. J., Bayazitli, I., & Mello, Z. R. (2023). An examination of multidimensional time perspective and mental health outcomes. International Journal of Environmental Research and Public Health, 20(6), 4688. [DOI:10.3390/ijerph20064688] [PMID]
Mousavi, S. N., Hasanzadeh, R., & Dousti, Y. (2019). [Effectiveness of time perspective therapy on depression and social well-being of bereaved women (Persian)]. Journal of Research in Behavioural Sciences, 17(2), 205-213. [DOI:10.52547/rbs.17.2.205]
GBD 2019 Risk Factors Collaborators (2020). Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet (London, England), 396(10258), 1223–1249. [DOI:10.1016/S0140-6736(20)30752-2] [PMID]
Nejat, S., Montazeri, A., Holakouie Naieni, K., Mohammad, K., & Majdzadeh, S. (2006). [The World Health Organization quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version (Persian)]. Journal of School of Public Health and Institute of Public Health Research, 4(4), 1-12. [Link]
Rahimpour, S., Arefi, M., & Manshaii, G. R. (2021). [The effectiveness of mixed method of time perspective and mindfulness education on resilience and wisdom (Persian)]. Positive Psychology Research, 7(1), 35-52. [DOI:10.22108/ppls.2021.118779.1798]
Remington, G. (2006). Schizophrenia, antipsychotics, and the metabolic syndrome: Is there a silver lining? American Journal of Psychiatry, 163(7), 1132-1134. [DOI:10.1176/ajp.2006.163.7.1132] [PMID]
Saruco, E., & Pleger, B. (2021). A systematic review of obesity and binge eating associated impairment of the cognitive inhibition system. Frontiers in Nutrition, 8, 609012. [DOI:10.3389/fnut.2021.609012] [PMID]
Sarwer, D. B., & Polonsky, H. M. (2016). Body image and body contouring procedures. Aesthetic Surgery Journal, 36(9), 1039-1047. [DOI:10.1093/asj/sjw127] [PMID]
Shafiee, A., Nayebirad, S., Najafi, M. S., Jalali, A., Alaeddini, F., & Saadat, S., et al. (2023). Prevalence of obesity and overweight in an adult population of Tehran metropolis. Journal of Diabetes and Metabolic Disorders, 23(1), 895–907. [DOI:10.1007/s40200-023-01365-4] [PMID]
Stout, M. E., Medlin, A. R., Gupta, R., & Tsotsoros, C. E. (2024). Time perspective and perceived social isolation: The role of social interaction anxiety. Healthcare (Basel, Switzerland), 12(17), 1736. [DOI:10.3390/healthcare12171736] [PMID]
Whoqol Group. (1995). The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Social Science & Medicine, 41(10), 1403-1409. [DOI:10.1016/0277-9536(95)00112-K] [PMID]
Witowska, J., & Zajenkowski, M. (2018). How is perception of time associated with cognitive functioning? The relationship between time perspective and executive control. Time & Society, 28(3), 1124-1147. [DOI:10.1177/0961463X18763693]
Zancu, S. A., Măirean, C., & Diaconu-Gherasim, L. R. (2022). The longitudinal relation between time perspective and preventive behaviors during the COVID-19 pandemic: The mediating role of risk perception. Current Psychology, 43, 12981-12989. [PMID]
Zimbardo, P. (2002). Just think about it: Time to take our time. Looking to the future is important and very American-but living in the present is vital. Psychology Today, 35, 62. [Link]
Zimbardo, P. G., & Boyd, J. N. (2014). Putting time in perspective: A valid, reliable individual-differences metric. In M. Stolarski, N. Fieulaine& W. van Beek (Eds), Time Perspective Theory; Review, Research and Application. Cham: Springer.[DOI:10.1007/978-3-319-07368-2_2]
Type of Study: Original Research Article |
Subject:
Family and group therapy
Received: 2025/06/2 | Accepted: 2025/07/21 | Published: 2025/10/1
Received: 2025/06/2 | Accepted: 2025/07/21 | Published: 2025/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
