

Volume 13, Issue 4 (Autumn 2025)
PCP 2025, 13(4): 333-346 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bana E, Taghvaei D, Jahangiri M M. A Causal Model of Death Anxiety in the Elderly: Emotion Regulation,Meaning in Life, and Resilience. PCP 2025; 13 (4) :333-346
URL: http://jpcp.uswr.ac.ir/article-1-1020-en.html
URL: http://jpcp.uswr.ac.ir/article-1-1020-en.html



1- Department of Psychology, Ar.C., Islamic Azad University, Arak, Iran.
2- Department of Psychology, Ar.C., Islamic Azad University, Arak, Iran. ,d_taghvaei@iau-arak.ac.ir
2- Department of Psychology, Ar.C., Islamic Azad University, Arak, Iran. ,
Full-Text [PDF 782 kb]
(1590 Downloads)
| Abstract (HTML) (1576 Views)

Full-Text: (612 Views)
Introduction
Death anxiety is a sense of worry and uneasiness related to the inevitability of death and its aftermath. Among older adults, this form of anxiety is frequently observed, largely because of increased exposure to chronic health conditions, reduced functional abilities, bereavement, and recognition of life’s limited span (Templer, 1970; Griffin, 2007). In Iranian culture, where religious and familial values play a central role in everyday life, death anxiety may be shaped by specific cultural beliefs and attitudes (Hashemi Rezini et al., 2017).
Psychological research has demonstrated that multiple factors can either exacerbate or alleviate death anxiety. Among these, coping strategies, cognitive emotion regulation styles, and the pursuit of meaning in life are particularly influential. Coping strategies, conceptualized by Lazarus and Folkman (1984) as cognitive and behavioral patterns for managing stress, significantly affect individuals’ approaches to death. For example, problem-focused coping may mitigate anxiety, whereas avoidance-oriented coping may intensify it (Endler & Parker, 1990). Similarly, cognitive emotion regulation, mental processes for managing emotional responses, can assist older adults in moderating negative feelings related to death (Garnefski et al., 2001). Prior studies have suggested that adaptive emotion regulation strategies, such as acceptance and positive reappraisal, are associated with reduced anxiety symptoms (Garnefski & Kraaij, 2006).
Emotion regulation has been recognized as a key variable in death anxiety among the older adults. It is a complex process involving the interaction of neurophysiological, behavioral-expressive, and cognitive-experiential components of emotion (Nemiah, 2000). Emotion regulation refers to the capacity to monitor, evaluate, and modify emotional reactions in ways that facilitate adaptive functioning (Garnefski & Kraaij, 2006; Gillanders et al., 2008). According to emotion regulation models, this process serves as a unique mechanism for modulating emotional experiences, with the goal of achieving social appropriateness and maintaining a state of psychological and physiological readiness to respond effectively to internal and external demands (Gross, 2013; Garnefski & Kraaij, 2006). Therefore, adaptive emotion regulation is essential for everyday functioning (Gillanders et al., 2008).
Numerous studies have examined the strategies individuals use to regulate emotions, which can be broadly categorized as adaptive or maladaptive (Garnefski & Kraaij, 2006). Within this framework, Garnefski and Kraaij identified nine distinct cognitive emotion regulation strategies: Self-blame, acceptance, rumination, positive refocusing, planning, positive reappraisal, putting into perspective, catastrophizing, and other-blame (Garnefski & Kraaij, 2006). In daily life, individuals constantly employ such strategies to adjust the intensity and quality of emotional experiences triggered by stress-inducing events (Diamond & Aspinwall, 2003). As Gyurak and Gross (2011) argue, these regulatory strategies play a crucial role in adapting to life’s stressors (Garnefski & Kraaij, 2006).
Based on these foundations, the present study seeks to address the following research question: Does a causal model of death anxiety, grounded in cognitive emotion regulation strategies and meaning in life, with resilience as a mediator, adequately fit the data collected from older adult residents of Tehran Province?
Materials and Methods
The present study employed a descriptive-correlational design in terms of method. The research design employed a causal model, which was tested through structural equation modeling (SEM). The statistical population comprised all elderly men and women residing in Tehran Province in 2024. Due to the large size of the target population, a multistage cluster sampling method was adopted. For accessibility, one park from each of the northern, eastern, northeastern, and southeastern districts of Tehran, identified by the municipality as gathering sites for older adults, was selected for sampling.
Research instruments
Templer death anxiety scale
The Templer death anxiety scale (1970) was used to measure participants’ levels of anxiety toward death. The scale includes 15 yes/no questions, with a possible score range of 0-15. Higher scores reflect greater anxiety related to death. The reliability and validity of this instrument have been confirmed in several studies. For example, Templer originally reported a test re-test reliability of 0.83, while in Iran, Rajabi et al. (2019) found an internal consistency coefficient of 0.73 and acceptable concurrent validity.
Cognitive emotion regulation questionnaire (CERQ)
Cognitive emotion regulation strategies were assessed using the CERQ (Garnefski & Kraaij, 2006). This questionnaire comprises 18 items, covering nine subscales: Self-blame, other-blame, rumination, catastrophizing, putting things into perspective, positive refocusing, positive reappraisal, acceptance, and planning. Responses are given on a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always). The subscales are divided into adaptive strategies (e.g. reappraisal, acceptance, planning) and maladaptive strategies (e.g. catastrophizing, blame, rumination). The reported internal consistency is high, with Cronbach’s α values ranging from 0.87 to 0.93. The Persian version of the CERQ has also demonstrated acceptable psychometric properties (Hasani, 2011).
Meaning in life questionnaire (MLQ)
Meaning in life was measured using the MLQ developed by Steger et al. (2006). This instrument consists of 10 items distributed across two subscales: presence of meaning (e.g. “My life has a clear purpose”) and search for meaning (e.g. “I am looking for something that makes my life meaningful”). Items are rated on a Likert-type scale, with higher scores indicating a stronger presence or search for meaning. Previous studies have reported Cronbach’s α values ranging from 0.70 to 0.82. In Iran, psychometric studies have confirmed the validity and reliability of this measure (Mesrabadi et al., 2013).
Connor–Davidson resilience scale (CD-RISC)
Resilience was assessed using the 25-item D-RISC (Connor & Davidson, 2003). Each item is scored on a 5-point scale (0=not true at all to 4=true nearly all the time), resulting in a total score between 0 and 100, with higher scores indicating greater resilience. The scale measures dimensions, such as competence, trust in instincts, adaptability to change, control, and spirituality. Connor and Davidson reported high internal consistency (α=0.89) and test re-test reliability (0.87). Several studies in Iran (Jowkar, 2007; Rezaei et al., 2021) have also confirmed its reliability and construct validity.
Results
In the present study, 384 older adults (183 women and 201 men) participated. Among them, 138 individuals (36.9%) were <70 years old, 154 individuals (40.1%) were between 71 and 75 years old, and 92 individuals (24%) were >75 years old. Regarding educational level, 114 participants (29.7%) were literate, 108(28.1%) had completed middle school, 95(24.7%) held a high school diploma, and 67(17.5%) had an education above the diploma level. Regarding marital status, 285 participants (67.2%) were married, 39(10.1%) were divorced, and 87(22.7%) were widowed. Table 1 presents the means, standard deviations, and correlation coefficients for the study variables.

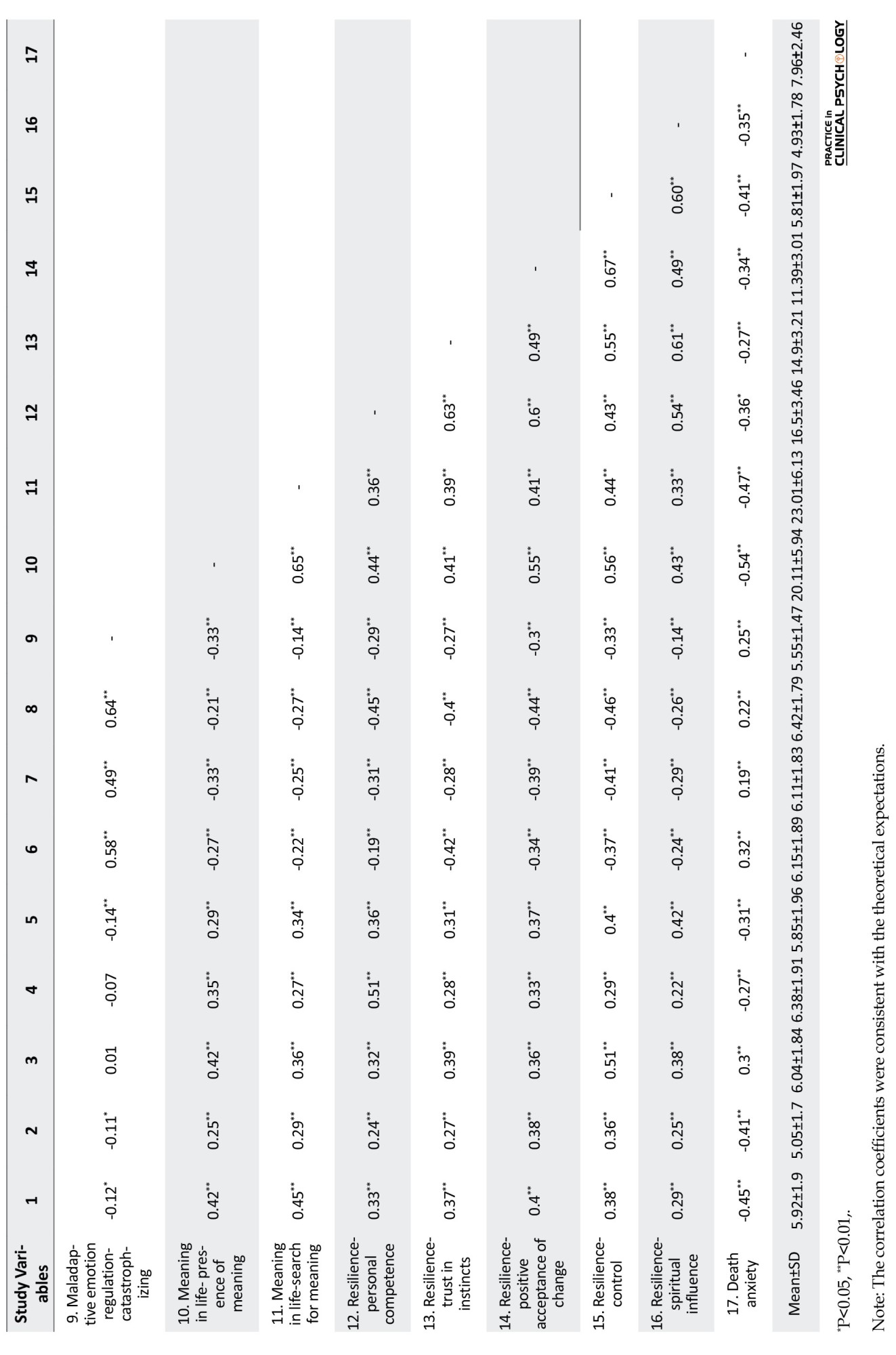
Based on the results of Table 1, the correlation coefficients between the variables were in the expected direction and consistent with the theoretical framework of the study. In this research, to evaluate the assumption of univariate normality, the skewness and kurtosis of each variable were examined. To assess the multicollinearity assumption, the variance inflation factor (VIF) and tolerance values were analyzed. The results are presented in Table 2.
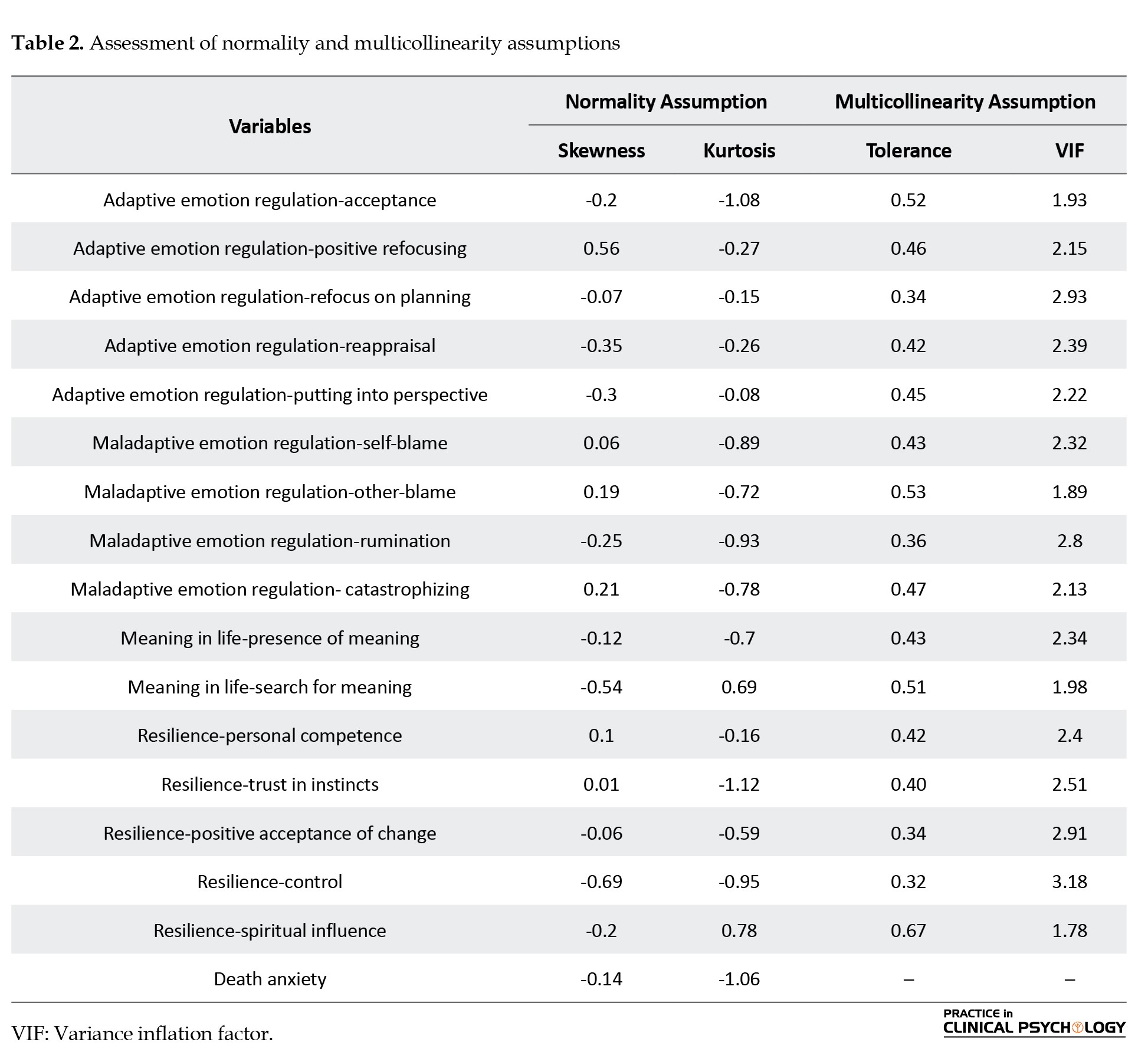
According to the findings in Table 2, the skewness and kurtosis values of all components were within the ±2 range. This indicates that the assumption of univariate normality was met for the data. Table 2 also shows that the multicollinearity assumption was satisfied in the present study, as the tolerance values of the predictor variables were greater than 0.1 and the VIF values were less than 10. According to Meyers et al. (2006), a tolerance value below 0.1 and a VIF above 10 indicate a violation of the multicollinearity assumption. In this study, the assumption of multivariate normality was assessed using Mahalanobis distance. The skewness and kurtosis values of the Mahalanobis distances were 0.97 and 0.69, respectively, indicating that this assumption was met. Finally, to evaluate the assumption of homogeneity of variances, a scatter plot of standardized residual variances was examined, and the results showed that this assumption was also satisfied among the data.
Model analysis
In the present study, adaptive emotion regulation strategies, maladaptive emotion regulation strategies, meaning in life, and resilience were latent variables that constituted the measurement model of the research. It was hypothesized that the latent variable of adaptive emotion regulation would be measured through the indicators of acceptance, positive refocusing, refocus on planning, reappraisal, and trivialization; the latent variable of maladaptive emotion regulation would be measured through the indicators of self-blame, blaming others, rumination, and catastrophizing; the latent variable of meaning in life would be measured through the indicators of presence of meaning and search for meaning; and the latent variable of resilience would be measured through the indicators of personal competence, trust in instincts, positive acceptance of change, control, and spiritual influences.
The fit of the measurement model was evaluated using confirmatory factor analysis (CFA) in AMOS software, version 24.0, employing the maximum likelihood estimation method. Table 3 presents the fit indices for the measurement and structural models.

Table 3 shows that the fit indices obtained from CFA support the acceptable fit of the measurement model to the collected data. In the measurement model, the highest factor loading belonged to the reappraisal indicator (β=0.927), and the lowest factor loading belonged to the spiritual influence indicator (β=0.659). Therefore, given that all factor loadings exceeded 0.32, it can be concluded that all indicators possessed sufficient capability to measure the latent variables in this study.
After assessing the measurement model fit, in the second stage, the fit indices of the structural model (Figure 1) were estimated and evaluated. In the structural model, it was hypothesized that death anxiety in older adults is explained by cognitive emotion regulation strategies and meaning in life, mediated by resilience.
Death anxiety is a sense of worry and uneasiness related to the inevitability of death and its aftermath. Among older adults, this form of anxiety is frequently observed, largely because of increased exposure to chronic health conditions, reduced functional abilities, bereavement, and recognition of life’s limited span (Templer, 1970; Griffin, 2007). In Iranian culture, where religious and familial values play a central role in everyday life, death anxiety may be shaped by specific cultural beliefs and attitudes (Hashemi Rezini et al., 2017).
Psychological research has demonstrated that multiple factors can either exacerbate or alleviate death anxiety. Among these, coping strategies, cognitive emotion regulation styles, and the pursuit of meaning in life are particularly influential. Coping strategies, conceptualized by Lazarus and Folkman (1984) as cognitive and behavioral patterns for managing stress, significantly affect individuals’ approaches to death. For example, problem-focused coping may mitigate anxiety, whereas avoidance-oriented coping may intensify it (Endler & Parker, 1990). Similarly, cognitive emotion regulation, mental processes for managing emotional responses, can assist older adults in moderating negative feelings related to death (Garnefski et al., 2001). Prior studies have suggested that adaptive emotion regulation strategies, such as acceptance and positive reappraisal, are associated with reduced anxiety symptoms (Garnefski & Kraaij, 2006).
Emotion regulation has been recognized as a key variable in death anxiety among the older adults. It is a complex process involving the interaction of neurophysiological, behavioral-expressive, and cognitive-experiential components of emotion (Nemiah, 2000). Emotion regulation refers to the capacity to monitor, evaluate, and modify emotional reactions in ways that facilitate adaptive functioning (Garnefski & Kraaij, 2006; Gillanders et al., 2008). According to emotion regulation models, this process serves as a unique mechanism for modulating emotional experiences, with the goal of achieving social appropriateness and maintaining a state of psychological and physiological readiness to respond effectively to internal and external demands (Gross, 2013; Garnefski & Kraaij, 2006). Therefore, adaptive emotion regulation is essential for everyday functioning (Gillanders et al., 2008).
Numerous studies have examined the strategies individuals use to regulate emotions, which can be broadly categorized as adaptive or maladaptive (Garnefski & Kraaij, 2006). Within this framework, Garnefski and Kraaij identified nine distinct cognitive emotion regulation strategies: Self-blame, acceptance, rumination, positive refocusing, planning, positive reappraisal, putting into perspective, catastrophizing, and other-blame (Garnefski & Kraaij, 2006). In daily life, individuals constantly employ such strategies to adjust the intensity and quality of emotional experiences triggered by stress-inducing events (Diamond & Aspinwall, 2003). As Gyurak and Gross (2011) argue, these regulatory strategies play a crucial role in adapting to life’s stressors (Garnefski & Kraaij, 2006).
Based on these foundations, the present study seeks to address the following research question: Does a causal model of death anxiety, grounded in cognitive emotion regulation strategies and meaning in life, with resilience as a mediator, adequately fit the data collected from older adult residents of Tehran Province?
Materials and Methods
The present study employed a descriptive-correlational design in terms of method. The research design employed a causal model, which was tested through structural equation modeling (SEM). The statistical population comprised all elderly men and women residing in Tehran Province in 2024. Due to the large size of the target population, a multistage cluster sampling method was adopted. For accessibility, one park from each of the northern, eastern, northeastern, and southeastern districts of Tehran, identified by the municipality as gathering sites for older adults, was selected for sampling.
Research instruments
Templer death anxiety scale
The Templer death anxiety scale (1970) was used to measure participants’ levels of anxiety toward death. The scale includes 15 yes/no questions, with a possible score range of 0-15. Higher scores reflect greater anxiety related to death. The reliability and validity of this instrument have been confirmed in several studies. For example, Templer originally reported a test re-test reliability of 0.83, while in Iran, Rajabi et al. (2019) found an internal consistency coefficient of 0.73 and acceptable concurrent validity.
Cognitive emotion regulation questionnaire (CERQ)
Cognitive emotion regulation strategies were assessed using the CERQ (Garnefski & Kraaij, 2006). This questionnaire comprises 18 items, covering nine subscales: Self-blame, other-blame, rumination, catastrophizing, putting things into perspective, positive refocusing, positive reappraisal, acceptance, and planning. Responses are given on a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always). The subscales are divided into adaptive strategies (e.g. reappraisal, acceptance, planning) and maladaptive strategies (e.g. catastrophizing, blame, rumination). The reported internal consistency is high, with Cronbach’s α values ranging from 0.87 to 0.93. The Persian version of the CERQ has also demonstrated acceptable psychometric properties (Hasani, 2011).
Meaning in life questionnaire (MLQ)
Meaning in life was measured using the MLQ developed by Steger et al. (2006). This instrument consists of 10 items distributed across two subscales: presence of meaning (e.g. “My life has a clear purpose”) and search for meaning (e.g. “I am looking for something that makes my life meaningful”). Items are rated on a Likert-type scale, with higher scores indicating a stronger presence or search for meaning. Previous studies have reported Cronbach’s α values ranging from 0.70 to 0.82. In Iran, psychometric studies have confirmed the validity and reliability of this measure (Mesrabadi et al., 2013).
Connor–Davidson resilience scale (CD-RISC)
Resilience was assessed using the 25-item D-RISC (Connor & Davidson, 2003). Each item is scored on a 5-point scale (0=not true at all to 4=true nearly all the time), resulting in a total score between 0 and 100, with higher scores indicating greater resilience. The scale measures dimensions, such as competence, trust in instincts, adaptability to change, control, and spirituality. Connor and Davidson reported high internal consistency (α=0.89) and test re-test reliability (0.87). Several studies in Iran (Jowkar, 2007; Rezaei et al., 2021) have also confirmed its reliability and construct validity.
Results
In the present study, 384 older adults (183 women and 201 men) participated. Among them, 138 individuals (36.9%) were <70 years old, 154 individuals (40.1%) were between 71 and 75 years old, and 92 individuals (24%) were >75 years old. Regarding educational level, 114 participants (29.7%) were literate, 108(28.1%) had completed middle school, 95(24.7%) held a high school diploma, and 67(17.5%) had an education above the diploma level. Regarding marital status, 285 participants (67.2%) were married, 39(10.1%) were divorced, and 87(22.7%) were widowed. Table 1 presents the means, standard deviations, and correlation coefficients for the study variables.
Based on the results of Table 1, the correlation coefficients between the variables were in the expected direction and consistent with the theoretical framework of the study. In this research, to evaluate the assumption of univariate normality, the skewness and kurtosis of each variable were examined. To assess the multicollinearity assumption, the variance inflation factor (VIF) and tolerance values were analyzed. The results are presented in Table 2.
According to the findings in Table 2, the skewness and kurtosis values of all components were within the ±2 range. This indicates that the assumption of univariate normality was met for the data. Table 2 also shows that the multicollinearity assumption was satisfied in the present study, as the tolerance values of the predictor variables were greater than 0.1 and the VIF values were less than 10. According to Meyers et al. (2006), a tolerance value below 0.1 and a VIF above 10 indicate a violation of the multicollinearity assumption. In this study, the assumption of multivariate normality was assessed using Mahalanobis distance. The skewness and kurtosis values of the Mahalanobis distances were 0.97 and 0.69, respectively, indicating that this assumption was met. Finally, to evaluate the assumption of homogeneity of variances, a scatter plot of standardized residual variances was examined, and the results showed that this assumption was also satisfied among the data.
Model analysis
In the present study, adaptive emotion regulation strategies, maladaptive emotion regulation strategies, meaning in life, and resilience were latent variables that constituted the measurement model of the research. It was hypothesized that the latent variable of adaptive emotion regulation would be measured through the indicators of acceptance, positive refocusing, refocus on planning, reappraisal, and trivialization; the latent variable of maladaptive emotion regulation would be measured through the indicators of self-blame, blaming others, rumination, and catastrophizing; the latent variable of meaning in life would be measured through the indicators of presence of meaning and search for meaning; and the latent variable of resilience would be measured through the indicators of personal competence, trust in instincts, positive acceptance of change, control, and spiritual influences.
The fit of the measurement model was evaluated using confirmatory factor analysis (CFA) in AMOS software, version 24.0, employing the maximum likelihood estimation method. Table 3 presents the fit indices for the measurement and structural models.
Table 3 shows that the fit indices obtained from CFA support the acceptable fit of the measurement model to the collected data. In the measurement model, the highest factor loading belonged to the reappraisal indicator (β=0.927), and the lowest factor loading belonged to the spiritual influence indicator (β=0.659). Therefore, given that all factor loadings exceeded 0.32, it can be concluded that all indicators possessed sufficient capability to measure the latent variables in this study.
After assessing the measurement model fit, in the second stage, the fit indices of the structural model (Figure 1) were estimated and evaluated. In the structural model, it was hypothesized that death anxiety in older adults is explained by cognitive emotion regulation strategies and meaning in life, mediated by resilience.
Table 3 indicates that the fit indices support the acceptable fit of the structural model to the collected data. Table 4 presents the path coefficients of the structural model.

Table 4 shows that the total path coefficient between adaptive cognitive emotion regulation strategies and death anxiety (β=-0.380, P=0.001) was negative and significant, whereas the total path coefficient between maladaptive cognitive emotion regulation strategies and death anxiety (β=0.213, P=0.001) was positive and significant. The table also indicates that the total path coefficient between meaning in life and death anxiety (β=-0.308, P=0.001) and the path coefficient between resilience and death anxiety (β=-0.527, P=0.001) were both negative and significant.
According to Table 4, the indirect path coefficient between adaptive cognitive emotion regulation strategies and death anxiety (β=-0.242, P=0.001) was negative and significant, while the indirect path coefficient between maladaptive cognitive emotion regulation strategies and death anxiety (β=0.175, P=0.001) was positive and significant. Additionally, the indirect path coefficient between meaning in life and death anxiety was negative and significant (β=-0.158, P=0.001).
Based on these findings, it can be concluded that resilience negatively mediates the relationship between adaptive cognitive emotion regulation strategies and meaning in life with death anxiety, while it positively and significantly mediates the relationship between maladaptive cognitive emotion regulation strategies and death anxiety among older adults. Figure 1 illustrates the structural model of this study using standardized data.
Parameters of the structural model in the study
According to Figure 1, the coefficient of determination (R²) for death anxiety was 0.60, indicating that cognitive emotion regulation strategies, meaning in life, and resilience together accounted for 60% of the variance in death anxiety among older adults.
Discussion
Hypothesis 1: Cognitive emotion regulation is related to death anxiety in the elderly.
The results of the present study indicated a significant relationship between cognitive emotion regulation and death anxiety among older adults. Specifically, individuals who employ adaptive emotion regulation strategies, such as positive reappraisal, acceptance, and planning, experience lower levels of death anxiety. This finding aligns with cognitive–emotional theories, which posit that the way emotions are managed plays a fundamental role in shaping the quality of emotional and psychological experiences (Garnefski & Kraaij, 2006).
Cognitive emotion regulation, as part of regulatory process, refers to how individuals interpret and assign meaning to emotionally triggering situations. In circumstances, such as confronting death, people inevitably encounter fear, hopelessness, feelings of helplessness, and anxiety. Those who can assess the situation logically and purposefully, using strategies like positive reappraisal, are able to reduce the intensity of negative emotions and experience greater psychological calm. In other words, effective emotion regulation can be a key factor in mitigating death anxiety.
Brown and Ryan (2003) demonstrated that the use of adaptive cognitive strategies, particularly during late adulthood, plays a predictive role in psychological well-being. Elderly individuals who manage their emotions efficiently are less likely to experience chronic anxiety, including death-related anxiety. Similar findings were reported by Rezaei et al. (2019), who showed that the mean death anxiety scores were significantly higher among older adults employing maladaptive strategies, such as rumination or self/other-blame.
From a theoretical perspective, Gross’s process model of emotion regulation outlines the stages of emotion regulation, from situation selection to cognitive reappraisal and response modulation. Within this model, cognitive reappraisal is considered one of the most effective strategies for attenuating negative emotional responses. In the context of death anxiety, elderly individuals who can attribute positive meaning to death not only experience less anxiety but also demonstrate higher resilience (Grross, 1988).
Conversely, maladaptive strategies, such as rumination, catastrophizing, or blame, are associated with increased anxiety levels. These strategies are inefficient and exacerbate negative thoughts, depression, and hopelessness. Such individuals may feel a lack of control over their future and perceive death as an unavoidable and terrifying threat.
The findings of this study have practical implications. Enhancing emotion regulation skills through psychological interventions, such as cognitive-behavioral therapy or mindfulness training, can help older adults cope better with daily emotions and reduce their death anxiety. Techniques such as cognitive reappraisal training, emotional acceptance, and interruption of rumination can be effectively employed.
Overall, cognitive emotion regulation plays a fundamental role in reducing death anxiety among the elderly. Older adults who utilize adaptive strategies have a more positive perception of life, death, and aging and experience less severe and debilitating anxiety. These findings underscore the importance of teaching emotion regulation skills as part of programs designed to promote mental health in the elderly.
Hypothesis 2: Meaning in life is related to death anxiety in the elderly.
The results revealed that meaning in life is inversely associated with death anxiety in the elderly. Older individuals who recognize their lives as purposeful and significant reported less fear and distress regarding death compared to those who lacked such a sense of meaning. This result aligns closely with Frankl’s logotherapy framework and the positive-psychology perspective. According to Frankl, individuals can endure suffering and confront death more tolerably when they find meaning in their experiences. Therefore, meaning in life not only affects the quality of living but also plays a crucial role in coping with death.
During late adulthood, which is often accompanied by retirement, reduced social roles, illnesses, and decreased social interactions, finding meaning in life can be a vital factor in maintaining mental health. Elderly individuals who perceive their lives as valuable and purposeful tend to view death not as an end, but as a stage in a meaningful process. This perspective reduces fear and anxiety related to death.
Several empirical studies have supported this relationship. For instance, Steger et al. (2006) found that individuals with higher scores on the meaning in life scale reported lower levels of existential and death anxiety. Similarly, Wong demonstrated within the framework of positive psychology of death that a sense of meaning in life is inversely related to death anxiety, emphasizing that meaning equips individuals to face fundamental fears, such as death, with greater composure.
An Iranian study by Rahmani et al. (2020) confirmed these findings, showing that aspects of meaning in life, such as having goals, perceiving life as valuable, and feeling useful, were significantly associated with reduced death anxiety in the elderly. The logotherapy interventions in this study significantly decreased death anxiety in the experimental group.
From an existential psychological perspective, death anxiety intensifies when individuals experience meaninglessness, emptiness, or disorientation. Elderly individuals who perceive their past as unfulfilled or cannot envision a future are more vulnerable to death-related anxieties (Osborne, 2017). Conversely, those who maintain a sense of meaning and inner direction, even under challenging physical conditions, cope with death more adaptively. This mindset not only reduces anxiety but also enhances overall quality of life (Dursun et al., 2022).
Practically, enhancing the sense of meaning in life can be an effective strategy to mitigate death anxiety. Interventions, such as logotherapy, narrative therapy, and intergenerational dialogues, can help older adults reinterpret past experiences, reinforce feelings of usefulness, and envision a valuable future (Gholcheshmeh et al., 2025).
In conclusion, meaning in life plays a key role in the mental health of older adults and serves as a protective factor against death anxiety. Incorporating this factor into psychological interventions, especially for the elderly facing multiple life challenges, is essential.
Hypothesis 3: Resilience is related to death anxiety in the elderly.
The findings demonstrated that resilience and death anxiety are inversely related in the elderly population. In other words, individuals with stronger resilience skills tend to report lower levels of fear and concern about death.
This finding is consistent with existing theoretical and empirical literature, highlighting the protective role of resilience in facing psychological challenges, particularly existential anxieties such as fear of death.
Resilience, defined as the psychological capacity to recover from stressful and challenging situations, is a crucial coping resource in late adulthood. Elderly individuals with high resilience tend to have a more realistic understanding of death and, by accepting it as part of the natural life cycle, experience less severe anxiety and feelings of helplessness. Within the framework of positive psychology, Seligman identifies resilience as a core psychological strength that enables individuals to confront existential threats.
Azami et al. (2012) demonstrated that resilience plays a significant mediating role between psychological resources and reduced death anxiety.
From a cognitive–emotional perspective, resilience encompasses traits, such as optimism, acceptance, cognitive flexibility, and the ability to find meaning in negative events, which can protect individuals against anxiety. In older adults, these capacities contribute to a more positive attitude toward aging, disabilities, and death. According to Connor and Davidson, resilient individuals typically have stronger social support, firmer spiritual beliefs, and more effective emotion-regulation skills.
Conversely, older adults lacking sufficient resilience are more likely to perceive death as an imminent, unfair, and terrifying threat. This negative perception sharply increases death anxiety and may even lead to disorders such as depression, generalized anxiety, and post-traumatic stress disorder (PTSD). Thus, psychological interventions aimed at enhancing resilience play a crucial role in improving the mental health of the elderly.
Practically, resilience is not a fixed trait; it can be strengthened through training, practice, and group interventions. Mindfulness-based programs, acceptance and commitment therapy, and logotherapy can enhance resilience and, consequently, reduce death anxiety. Providing social support, promoting intergenerational activities, and fostering a sense of usefulness can also increase resilience in the elderly.
In conclusion, resilience is a key factor in understanding, accepting, and managing death anxiety among older adults. Considering the growing elderly population, interventions targeting this psychological capacity should be prioritized in mental health policies for the elderly.
Hypothesis 4: Resilience mediates the relationship between cognitive emotion regulation and death anxiety in the elderly
Path analysis results indicated that resilience plays a significant mediating role in the relationship between cognitive emotion regulation and death anxiety. In other words, the effect of emotion regulation strategies on death anxiety can be explained through the enhancement or reduction of resilience. This finding suggests that elderly individuals who regulate their emotions adaptively tend to possess higher resilience, which, in turn, reduces their death anxiety.
Theoretical models, such as Garnefski and Kraaij’s emotion regulation framework, suggest that strategies, such as positive reappraisal, acceptance, planning, and perspective-taking have a lasting positive impact on psychological resilience (Garnefski & Kraaij, 2001).
Brown and Ryan (2003) confirmed that adaptive emotion regulation strategies increase resilience capacity and, consequently, decrease death anxiety in older adults. Older adults who can understand, accept, and positively reinterpret negative emotions related to death experience less distress. Conversely, maladaptive strategies such as rumination, catastrophizing, and self/other-blame reduce resilience and increase anxiety.
Dubey et al. (2015) concluded that resilience significantly mediates the relationship between cognitive-emotional styles and psychological outcomes. Their study emphasized that without enhancing resilience, adaptive strategies may fail to achieve their full effectiveness in reducing anxiety. Therefore, resilience not only regulates emotional responses but also facilitates the transmission of the effects of emotion regulation on death anxiety.
Functionally, resilience serves as an internal resource in the elderly, enabling them to modify their responses to existential threats. Emotion regulation without sufficient resilience may be temporary or superficial. However, when emotion regulation strategies are combined with resilience, older adults can transform the threat of death into an opportunity for spiritual growth, acceptance, and inner peace.
Practically, these findings underscore the need for integrated interventions. Programs focusing solely on cognitive emotion regulation, without simultaneously enhancing resilience, may fail to achieve lasting reductions in death anxiety. Thus, interventions, such as positive-psychology cognitive-behavioral therapy, logotherapy, and mindfulness, targeting both emotional strategies and resilience, are likely to be more effective.
In summary, resilience is a crucial intermediary between cognitive emotion regulation and death anxiety in the elderly. Understanding this relationship can inform the development of effective psychological programs to enhance quality of life and mitigate existential concerns in older adults.
Hypothesis 5: Resilience mediates the relationship between meaning in life and death anxiety in the elderly.
Path analysis results indicated that resilience significantly mediates the relationship between meaning in life and death anxiety. In other words, older adults who perceive their lives as meaningful, purposeful, and valuable experience lower death anxiety through enhanced resilience. This finding is statistically significant and supported by robust theoretical and empirical evidence.
From Frankl’s logotherapy perspective, even under the most challenging life conditions, individuals can find meaning in negative experiences. This meaningful interpretation of life is a key factor in strengthening resilience. Older adults with a sense of purpose and value in life tend to exhibit greater psychological flexibility, which enables them to accept challenges such as aging, illness, and death as part of the natural course of life (Frankl, 1963).
Wong (2008), in his theory of positive death psychology, stated that “healthy acceptance of death” is possible through a meaningful life. Resilient individuals draw on life’s meaningful resources, and in the face of death, they experience acceptance, peace, and even a sense of liberation, rather than anxiety.
Steger et al. (2006) demonstrated that meaning in life is one of the strongest predictors of psychological resilience. Older adults with clear life goals and meaning show higher mental health indices and lower existential anxiety, particularly death anxiety.
Practically, research evidence suggests that interventions focused on helping older adults discover or reconstruct meaning in life can effectively increase resilience. For instance, Ahmadi et al. (2017) implemented group logotherapy with elderly participants and found that this intervention not only reduced death anxiety but also significantly enhanced psychological resilience.
Resilience, as a mediating construct, facilitates the transmission of the positive effects of meaning in life on reducing death anxiety. Individuals with meaningful life frameworks are more resistant to existential threats. They employ more effective coping strategies, regulate negative emotions better, and are less prone to excessive worry about death.
In conclusion, combining meaning in life with resilience-enhancing strategies can provide a framework for effective psychological interventions for the elderly. Activities, such as life review, volunteering, religious or spiritual practices, and role redefinition, can help older adults cultivate both meaning and resilience, ultimately alleviating death anxiety.
The present study proposed and tested a causal framework explaining death anxiety in the elderly, emphasizing the roles of cognitive emotion regulation and meaning in life, with resilience as a mediating mechanism. The results indicated that adaptive regulatory strategies and a stronger sense of meaning in life were linked to lower death anxiety, whereas maladaptive strategies contributed to higher fear levels. Moreover, resilience emerged as a critical factor that directly reduced death anxiety and mediated the relationships between the studied psychological variables.
Conclusion
These findings suggest that resilience acts as a psychological shield, enabling older adults to derive greater benefits from adaptive coping and meaning-making processes. Therefore, interventions that simultaneously strengthen resilience, promote adaptive emotion regulation skills, and enhance life meaning could be particularly effective in reducing existential distress in late adulthood. Approaches, such as mindfulness training, logotherapy, and resilience-based group interventions, are recommended for practical application.
Although the model accounted for a substantial portion of the variance in death anxiety, future research should expand its scope by including additional predictors, such as spirituality, physical health, and social support. Furthermore, conducting longitudinal and cross-cultural studies would provide a more comprehensive understanding of how these factors interact over time and across different societies.
Overall, this study contributes to the growing body of knowledge on aging and mental health by highlighting the intertwined roles of emotion regulation, life meaning, and resilience in shaping death anxiety. These insights have valuable implications for clinical practice, social policy, and the development of targeted psychological interventions for elderly populations.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Department of Psychology, Arak Branch, Islamic Azad University, Arak, Iran (Code: IR.IAU.ARAK.REC.1403.114).
Funding
This study was extracted from the PhD dissertation of Esmaeil Bana, approved by the Department of Psychology, Arak Branch, Islamic Azad University, Arak, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their gratitude to all the elderly participants for their cooperation.
References
Ahmadi, S., Bagheriyan, F., Heidari, M., & Kashfi, A. (2017). [Elderly and meaning in life: Field study of sources and dimensions of meaning in old women and men (Persian)]. Psychological Achievements, 24(1):1-22. [DOI: 10.22055/ psy.2017.17833.1531]
A'zami, Y., Mo'tamedi, A., Doostian, U., Jalalvand, M., & Farzanwgan, M. (2012). [The role of resiliency, spirituality, and religiosity in predicting satisfaction with life in the elderly (Persian)]. Counseling Culture and Psycotherapy, 3(12), 1-20. [DOI:10.22054/qccpc.2011.5906]
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of personality and social psychology, 84(4), 822–848 [DOI: 10.1037/0022-3514.84.4.822] [PMID]
Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson resilience scale (CDRISC). Depression and Anxiety, 18(2), 76–82. [DOI:10.1002/ da.10113] [PMID]
Diamond, L. M., & Aspinwall, L. G. (2003). Emotion regulation across the life span: An integrative perspective emphasizing self-regulation, positive affect, and dyadic processes. Motivation and Emotion, 27(2), 125-156. [DOI:10.1023/A:1024521920068]
Dubey, C., De Maria, J., Hoeppli, C., Betticher, D. C., & Eicher, M. (2015). Resilience and unmet supportive care needs in patients with cancer during early treatment: A descriptive study. European journal of oncology nursing: The official journal of European Oncology Nursing Society, 19(5), 582–588. [DOI:10.1016/j. ejon.2015.03.004] [PMID]
Dursun, P., Alyagut, P., & Yılmaz, I. (2022). Meaning in life, psychological hardiness and death anxiety: individuals with or without generalized anxiety disorder (GAD). Current Psychology, 41(6), 3299-3317. [DOI: 10.1007/s12144-021-02695-3] [PMID]
Endler, N. S., & Parker, J. D. A. (1990). Multidimensional assessment of coping: A critical evaluation. Journal of Personality and Social Psychology, 58(5), 844–854. [DOI: 10.1037/0022- 3514.58.5.844]
Frankl, V. E. (1963). Man’s search for meaning. Boston: Beacon Press. [Link]
Griffin, L. K. (2007). Compelled cooperation and the new corporate criminal procedure. New York University Law Review 82, 311. [Link]
Garnefski, N., & Kraaij, V. (2006). Cognitive emotion regulation questionnaire-development of a short 18-item version (CERQ-short). Personality and Individual Differences, 41(6), 1045-1053. [DOI:10.1016/j.paid.2006.04.010]
Garnefski, N., Kraaij, V., & Spinhoven, P. (2001). Negative life events, cognitive emotion regulation and emotional problems. Personality and Individual differences, 30(8), 1311-1327. [DOI:10.1016/S0191-8869(00)00113-6]
Gholcheshmeh, F. Z., Khoshli, A. K., & Mirani, A. (2025). The effectiveness of narrative therapy on death anxiety and sense of coherence in older women. Aging, 11(1), 77-92. [DOI:10.22126/ jap.2024.10521.1771]
Gillanders, S., Wild, M., Deighan, C., & Gillanders, D. (2008). Emotion regulation, affect, psychosocial functioning, and well-being in hemodialysis patients. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation, 51(4), 651–662. [DOI:10.1053/j.ajkd.2007.12.023] [PMID]
Gross, J. J. (2013). Handbook of emotion regulation. New York: Guilford Publications. [Link]
Gross, J. J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271-299. [DOI:10.1037/1089-2680.2.3.271]
Gyurak, A., Gross, J. J., & Etkin, A. (2011). Explicit and implicit emotion regulation: A dual-process framework. Cognition and emotion, 25(3), 400-412. [DOI: bs/10.1080/02699931.2010.544160]
Hasani, J. (2011). [Examining the reliability and validity of the short form of the cognitive emotion regulation questionnaire (Persian)]. Journal of Behavioral Science Research, 4(9), 229-240. [Link]
Hashemi Rezini, H., Bahashmat Joibari, S., & Rameshni, M. (2017). [Relationship between coping strategies and locus of control with the anxiety of death in old people.(Persian)]. Salmand: Iranian Journal of Ageing, 12(2), 232-241. [DOI:10.21859/ sija-1202232]
Jowkar, B. (2007). [The mediating role of resilience in the relationship between general and emotional intelligence and life satisfaction (Persian)]. Contemporary Psychology, 2(2 (4)), 3-12. [Link]Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer Press. [Link]
Mesraabadi J., Jafarian, S., & Ostovar, N. (2013). [Construct and diagnostic validity of the meaning in life questionnaire among university students (Persian)]. Journal of Behavioral Sciences, 7(1), 83-90. [Link]
Meyers,L.S , Gamest.G., & Goarin,A.J. (2006). Applied multivariate research, design and interpretation. London: Sage publication. [Link]
Nemiah, J. C. (2000). A psychodynamic view of psychosomatic medicine. Psychosomatic Medicine, 62(3), 299-303. [DOI:10.1097/00006842-200005000-00001] [PMID]
Osborne, J. W. (2017). An existential perspective on death anxiety, retirement, and related research problems. Canadian Journal on Aging/La Revue Canadienne du Vieillissement, 36(2), 246-255. [DOI: 10.1017/S0714980816000465]
Rajabi, G., Maghami, E., & Karami, J. (2019). [The role of proactive coping in psychological well-being: A study of Iranian students (Persian)]. Journal of Psychological Studies, 15(3), 45-60. [Link]
Rahmani, M., Darvishpour, A., & Pourghane, P. (2020). Application of MoCA, MMSE and AMTs tests in diagnosing the cognitive status of the elderly under hemodialysis in Medical centers of Guilan University of Medical Sciences in 2019. Journal of Gerontology, 5(3), 64-76. [Link]
Rezaei, S., Ahmadi, S., Rahmati, J., Hosseinifard, H., Dehnad, A., & Aryankhesal, A., et al. (2019). Global prevalence of depression in HIV/AIDS: A systematic review and meta-analysis. BMJ supportive & palliative care, 9(4), 404–412. [DOI:10.1136/bmjspcare-2019-001952] [PMID]
Rezaei, M., Karimi, F., & Ghasemi, A. (2021). Cultural influences on coping strategies among Iranian adults. Journal of Cross-Cultural Psychology, 52(4), 567–582.
Steger, M. F., Frazier, P., Oishi, S., & Kaler, M. (2006). The meaning in life questionnaire: assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53(1), 80-93. [DOI:10.1037/0022-0167.53.1.80]
Templer, D. I. (1970). The construction and validation of a death anxiety scale. The Journal of General Psychology, 82(2), 165-177. [DOI:10.1080/00221309.1970.9920634] [PMID]
Wong, P. T. P. (2008). Meaning management theory and death acceptance. In A. Tomer, G. T. Eliason, & P. T. P. Wong (Eds.), Existential and spiritual issues in death attitudes. New York: Psychology Press. [Link]
Table 4 shows that the total path coefficient between adaptive cognitive emotion regulation strategies and death anxiety (β=-0.380, P=0.001) was negative and significant, whereas the total path coefficient between maladaptive cognitive emotion regulation strategies and death anxiety (β=0.213, P=0.001) was positive and significant. The table also indicates that the total path coefficient between meaning in life and death anxiety (β=-0.308, P=0.001) and the path coefficient between resilience and death anxiety (β=-0.527, P=0.001) were both negative and significant.
According to Table 4, the indirect path coefficient between adaptive cognitive emotion regulation strategies and death anxiety (β=-0.242, P=0.001) was negative and significant, while the indirect path coefficient between maladaptive cognitive emotion regulation strategies and death anxiety (β=0.175, P=0.001) was positive and significant. Additionally, the indirect path coefficient between meaning in life and death anxiety was negative and significant (β=-0.158, P=0.001).
Based on these findings, it can be concluded that resilience negatively mediates the relationship between adaptive cognitive emotion regulation strategies and meaning in life with death anxiety, while it positively and significantly mediates the relationship between maladaptive cognitive emotion regulation strategies and death anxiety among older adults. Figure 1 illustrates the structural model of this study using standardized data.
Parameters of the structural model in the study
According to Figure 1, the coefficient of determination (R²) for death anxiety was 0.60, indicating that cognitive emotion regulation strategies, meaning in life, and resilience together accounted for 60% of the variance in death anxiety among older adults.
Discussion
Hypothesis 1: Cognitive emotion regulation is related to death anxiety in the elderly.
The results of the present study indicated a significant relationship between cognitive emotion regulation and death anxiety among older adults. Specifically, individuals who employ adaptive emotion regulation strategies, such as positive reappraisal, acceptance, and planning, experience lower levels of death anxiety. This finding aligns with cognitive–emotional theories, which posit that the way emotions are managed plays a fundamental role in shaping the quality of emotional and psychological experiences (Garnefski & Kraaij, 2006).
Cognitive emotion regulation, as part of regulatory process, refers to how individuals interpret and assign meaning to emotionally triggering situations. In circumstances, such as confronting death, people inevitably encounter fear, hopelessness, feelings of helplessness, and anxiety. Those who can assess the situation logically and purposefully, using strategies like positive reappraisal, are able to reduce the intensity of negative emotions and experience greater psychological calm. In other words, effective emotion regulation can be a key factor in mitigating death anxiety.
Brown and Ryan (2003) demonstrated that the use of adaptive cognitive strategies, particularly during late adulthood, plays a predictive role in psychological well-being. Elderly individuals who manage their emotions efficiently are less likely to experience chronic anxiety, including death-related anxiety. Similar findings were reported by Rezaei et al. (2019), who showed that the mean death anxiety scores were significantly higher among older adults employing maladaptive strategies, such as rumination or self/other-blame.
From a theoretical perspective, Gross’s process model of emotion regulation outlines the stages of emotion regulation, from situation selection to cognitive reappraisal and response modulation. Within this model, cognitive reappraisal is considered one of the most effective strategies for attenuating negative emotional responses. In the context of death anxiety, elderly individuals who can attribute positive meaning to death not only experience less anxiety but also demonstrate higher resilience (Grross, 1988).
Conversely, maladaptive strategies, such as rumination, catastrophizing, or blame, are associated with increased anxiety levels. These strategies are inefficient and exacerbate negative thoughts, depression, and hopelessness. Such individuals may feel a lack of control over their future and perceive death as an unavoidable and terrifying threat.
The findings of this study have practical implications. Enhancing emotion regulation skills through psychological interventions, such as cognitive-behavioral therapy or mindfulness training, can help older adults cope better with daily emotions and reduce their death anxiety. Techniques such as cognitive reappraisal training, emotional acceptance, and interruption of rumination can be effectively employed.
Overall, cognitive emotion regulation plays a fundamental role in reducing death anxiety among the elderly. Older adults who utilize adaptive strategies have a more positive perception of life, death, and aging and experience less severe and debilitating anxiety. These findings underscore the importance of teaching emotion regulation skills as part of programs designed to promote mental health in the elderly.
Hypothesis 2: Meaning in life is related to death anxiety in the elderly.
The results revealed that meaning in life is inversely associated with death anxiety in the elderly. Older individuals who recognize their lives as purposeful and significant reported less fear and distress regarding death compared to those who lacked such a sense of meaning. This result aligns closely with Frankl’s logotherapy framework and the positive-psychology perspective. According to Frankl, individuals can endure suffering and confront death more tolerably when they find meaning in their experiences. Therefore, meaning in life not only affects the quality of living but also plays a crucial role in coping with death.
During late adulthood, which is often accompanied by retirement, reduced social roles, illnesses, and decreased social interactions, finding meaning in life can be a vital factor in maintaining mental health. Elderly individuals who perceive their lives as valuable and purposeful tend to view death not as an end, but as a stage in a meaningful process. This perspective reduces fear and anxiety related to death.
Several empirical studies have supported this relationship. For instance, Steger et al. (2006) found that individuals with higher scores on the meaning in life scale reported lower levels of existential and death anxiety. Similarly, Wong demonstrated within the framework of positive psychology of death that a sense of meaning in life is inversely related to death anxiety, emphasizing that meaning equips individuals to face fundamental fears, such as death, with greater composure.
An Iranian study by Rahmani et al. (2020) confirmed these findings, showing that aspects of meaning in life, such as having goals, perceiving life as valuable, and feeling useful, were significantly associated with reduced death anxiety in the elderly. The logotherapy interventions in this study significantly decreased death anxiety in the experimental group.
From an existential psychological perspective, death anxiety intensifies when individuals experience meaninglessness, emptiness, or disorientation. Elderly individuals who perceive their past as unfulfilled or cannot envision a future are more vulnerable to death-related anxieties (Osborne, 2017). Conversely, those who maintain a sense of meaning and inner direction, even under challenging physical conditions, cope with death more adaptively. This mindset not only reduces anxiety but also enhances overall quality of life (Dursun et al., 2022).
Practically, enhancing the sense of meaning in life can be an effective strategy to mitigate death anxiety. Interventions, such as logotherapy, narrative therapy, and intergenerational dialogues, can help older adults reinterpret past experiences, reinforce feelings of usefulness, and envision a valuable future (Gholcheshmeh et al., 2025).
In conclusion, meaning in life plays a key role in the mental health of older adults and serves as a protective factor against death anxiety. Incorporating this factor into psychological interventions, especially for the elderly facing multiple life challenges, is essential.
Hypothesis 3: Resilience is related to death anxiety in the elderly.
The findings demonstrated that resilience and death anxiety are inversely related in the elderly population. In other words, individuals with stronger resilience skills tend to report lower levels of fear and concern about death.
This finding is consistent with existing theoretical and empirical literature, highlighting the protective role of resilience in facing psychological challenges, particularly existential anxieties such as fear of death.
Resilience, defined as the psychological capacity to recover from stressful and challenging situations, is a crucial coping resource in late adulthood. Elderly individuals with high resilience tend to have a more realistic understanding of death and, by accepting it as part of the natural life cycle, experience less severe anxiety and feelings of helplessness. Within the framework of positive psychology, Seligman identifies resilience as a core psychological strength that enables individuals to confront existential threats.
Azami et al. (2012) demonstrated that resilience plays a significant mediating role between psychological resources and reduced death anxiety.
From a cognitive–emotional perspective, resilience encompasses traits, such as optimism, acceptance, cognitive flexibility, and the ability to find meaning in negative events, which can protect individuals against anxiety. In older adults, these capacities contribute to a more positive attitude toward aging, disabilities, and death. According to Connor and Davidson, resilient individuals typically have stronger social support, firmer spiritual beliefs, and more effective emotion-regulation skills.
Conversely, older adults lacking sufficient resilience are more likely to perceive death as an imminent, unfair, and terrifying threat. This negative perception sharply increases death anxiety and may even lead to disorders such as depression, generalized anxiety, and post-traumatic stress disorder (PTSD). Thus, psychological interventions aimed at enhancing resilience play a crucial role in improving the mental health of the elderly.
Practically, resilience is not a fixed trait; it can be strengthened through training, practice, and group interventions. Mindfulness-based programs, acceptance and commitment therapy, and logotherapy can enhance resilience and, consequently, reduce death anxiety. Providing social support, promoting intergenerational activities, and fostering a sense of usefulness can also increase resilience in the elderly.
In conclusion, resilience is a key factor in understanding, accepting, and managing death anxiety among older adults. Considering the growing elderly population, interventions targeting this psychological capacity should be prioritized in mental health policies for the elderly.
Hypothesis 4: Resilience mediates the relationship between cognitive emotion regulation and death anxiety in the elderly
Path analysis results indicated that resilience plays a significant mediating role in the relationship between cognitive emotion regulation and death anxiety. In other words, the effect of emotion regulation strategies on death anxiety can be explained through the enhancement or reduction of resilience. This finding suggests that elderly individuals who regulate their emotions adaptively tend to possess higher resilience, which, in turn, reduces their death anxiety.
Theoretical models, such as Garnefski and Kraaij’s emotion regulation framework, suggest that strategies, such as positive reappraisal, acceptance, planning, and perspective-taking have a lasting positive impact on psychological resilience (Garnefski & Kraaij, 2001).
Brown and Ryan (2003) confirmed that adaptive emotion regulation strategies increase resilience capacity and, consequently, decrease death anxiety in older adults. Older adults who can understand, accept, and positively reinterpret negative emotions related to death experience less distress. Conversely, maladaptive strategies such as rumination, catastrophizing, and self/other-blame reduce resilience and increase anxiety.
Dubey et al. (2015) concluded that resilience significantly mediates the relationship between cognitive-emotional styles and psychological outcomes. Their study emphasized that without enhancing resilience, adaptive strategies may fail to achieve their full effectiveness in reducing anxiety. Therefore, resilience not only regulates emotional responses but also facilitates the transmission of the effects of emotion regulation on death anxiety.
Functionally, resilience serves as an internal resource in the elderly, enabling them to modify their responses to existential threats. Emotion regulation without sufficient resilience may be temporary or superficial. However, when emotion regulation strategies are combined with resilience, older adults can transform the threat of death into an opportunity for spiritual growth, acceptance, and inner peace.
Practically, these findings underscore the need for integrated interventions. Programs focusing solely on cognitive emotion regulation, without simultaneously enhancing resilience, may fail to achieve lasting reductions in death anxiety. Thus, interventions, such as positive-psychology cognitive-behavioral therapy, logotherapy, and mindfulness, targeting both emotional strategies and resilience, are likely to be more effective.
In summary, resilience is a crucial intermediary between cognitive emotion regulation and death anxiety in the elderly. Understanding this relationship can inform the development of effective psychological programs to enhance quality of life and mitigate existential concerns in older adults.
Hypothesis 5: Resilience mediates the relationship between meaning in life and death anxiety in the elderly.
Path analysis results indicated that resilience significantly mediates the relationship between meaning in life and death anxiety. In other words, older adults who perceive their lives as meaningful, purposeful, and valuable experience lower death anxiety through enhanced resilience. This finding is statistically significant and supported by robust theoretical and empirical evidence.
From Frankl’s logotherapy perspective, even under the most challenging life conditions, individuals can find meaning in negative experiences. This meaningful interpretation of life is a key factor in strengthening resilience. Older adults with a sense of purpose and value in life tend to exhibit greater psychological flexibility, which enables them to accept challenges such as aging, illness, and death as part of the natural course of life (Frankl, 1963).
Wong (2008), in his theory of positive death psychology, stated that “healthy acceptance of death” is possible through a meaningful life. Resilient individuals draw on life’s meaningful resources, and in the face of death, they experience acceptance, peace, and even a sense of liberation, rather than anxiety.
Steger et al. (2006) demonstrated that meaning in life is one of the strongest predictors of psychological resilience. Older adults with clear life goals and meaning show higher mental health indices and lower existential anxiety, particularly death anxiety.
Practically, research evidence suggests that interventions focused on helping older adults discover or reconstruct meaning in life can effectively increase resilience. For instance, Ahmadi et al. (2017) implemented group logotherapy with elderly participants and found that this intervention not only reduced death anxiety but also significantly enhanced psychological resilience.
Resilience, as a mediating construct, facilitates the transmission of the positive effects of meaning in life on reducing death anxiety. Individuals with meaningful life frameworks are more resistant to existential threats. They employ more effective coping strategies, regulate negative emotions better, and are less prone to excessive worry about death.
In conclusion, combining meaning in life with resilience-enhancing strategies can provide a framework for effective psychological interventions for the elderly. Activities, such as life review, volunteering, religious or spiritual practices, and role redefinition, can help older adults cultivate both meaning and resilience, ultimately alleviating death anxiety.
The present study proposed and tested a causal framework explaining death anxiety in the elderly, emphasizing the roles of cognitive emotion regulation and meaning in life, with resilience as a mediating mechanism. The results indicated that adaptive regulatory strategies and a stronger sense of meaning in life were linked to lower death anxiety, whereas maladaptive strategies contributed to higher fear levels. Moreover, resilience emerged as a critical factor that directly reduced death anxiety and mediated the relationships between the studied psychological variables.
Conclusion
These findings suggest that resilience acts as a psychological shield, enabling older adults to derive greater benefits from adaptive coping and meaning-making processes. Therefore, interventions that simultaneously strengthen resilience, promote adaptive emotion regulation skills, and enhance life meaning could be particularly effective in reducing existential distress in late adulthood. Approaches, such as mindfulness training, logotherapy, and resilience-based group interventions, are recommended for practical application.
Although the model accounted for a substantial portion of the variance in death anxiety, future research should expand its scope by including additional predictors, such as spirituality, physical health, and social support. Furthermore, conducting longitudinal and cross-cultural studies would provide a more comprehensive understanding of how these factors interact over time and across different societies.
Overall, this study contributes to the growing body of knowledge on aging and mental health by highlighting the intertwined roles of emotion regulation, life meaning, and resilience in shaping death anxiety. These insights have valuable implications for clinical practice, social policy, and the development of targeted psychological interventions for elderly populations.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Department of Psychology, Arak Branch, Islamic Azad University, Arak, Iran (Code: IR.IAU.ARAK.REC.1403.114).
Funding
This study was extracted from the PhD dissertation of Esmaeil Bana, approved by the Department of Psychology, Arak Branch, Islamic Azad University, Arak, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their gratitude to all the elderly participants for their cooperation.
References
Ahmadi, S., Bagheriyan, F., Heidari, M., & Kashfi, A. (2017). [Elderly and meaning in life: Field study of sources and dimensions of meaning in old women and men (Persian)]. Psychological Achievements, 24(1):1-22. [DOI: 10.22055/ psy.2017.17833.1531]
A'zami, Y., Mo'tamedi, A., Doostian, U., Jalalvand, M., & Farzanwgan, M. (2012). [The role of resiliency, spirituality, and religiosity in predicting satisfaction with life in the elderly (Persian)]. Counseling Culture and Psycotherapy, 3(12), 1-20. [DOI:10.22054/qccpc.2011.5906]
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of personality and social psychology, 84(4), 822–848 [DOI: 10.1037/0022-3514.84.4.822] [PMID]
Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor-Davidson resilience scale (CDRISC). Depression and Anxiety, 18(2), 76–82. [DOI:10.1002/ da.10113] [PMID]
Diamond, L. M., & Aspinwall, L. G. (2003). Emotion regulation across the life span: An integrative perspective emphasizing self-regulation, positive affect, and dyadic processes. Motivation and Emotion, 27(2), 125-156. [DOI:10.1023/A:1024521920068]
Dubey, C., De Maria, J., Hoeppli, C., Betticher, D. C., & Eicher, M. (2015). Resilience and unmet supportive care needs in patients with cancer during early treatment: A descriptive study. European journal of oncology nursing: The official journal of European Oncology Nursing Society, 19(5), 582–588. [DOI:10.1016/j. ejon.2015.03.004] [PMID]
Dursun, P., Alyagut, P., & Yılmaz, I. (2022). Meaning in life, psychological hardiness and death anxiety: individuals with or without generalized anxiety disorder (GAD). Current Psychology, 41(6), 3299-3317. [DOI: 10.1007/s12144-021-02695-3] [PMID]
Endler, N. S., & Parker, J. D. A. (1990). Multidimensional assessment of coping: A critical evaluation. Journal of Personality and Social Psychology, 58(5), 844–854. [DOI: 10.1037/0022- 3514.58.5.844]
Frankl, V. E. (1963). Man’s search for meaning. Boston: Beacon Press. [Link]
Griffin, L. K. (2007). Compelled cooperation and the new corporate criminal procedure. New York University Law Review 82, 311. [Link]
Garnefski, N., & Kraaij, V. (2006). Cognitive emotion regulation questionnaire-development of a short 18-item version (CERQ-short). Personality and Individual Differences, 41(6), 1045-1053. [DOI:10.1016/j.paid.2006.04.010]
Garnefski, N., Kraaij, V., & Spinhoven, P. (2001). Negative life events, cognitive emotion regulation and emotional problems. Personality and Individual differences, 30(8), 1311-1327. [DOI:10.1016/S0191-8869(00)00113-6]
Gholcheshmeh, F. Z., Khoshli, A. K., & Mirani, A. (2025). The effectiveness of narrative therapy on death anxiety and sense of coherence in older women. Aging, 11(1), 77-92. [DOI:10.22126/ jap.2024.10521.1771]
Gillanders, S., Wild, M., Deighan, C., & Gillanders, D. (2008). Emotion regulation, affect, psychosocial functioning, and well-being in hemodialysis patients. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation, 51(4), 651–662. [DOI:10.1053/j.ajkd.2007.12.023] [PMID]
Gross, J. J. (2013). Handbook of emotion regulation. New York: Guilford Publications. [Link]
Gross, J. J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271-299. [DOI:10.1037/1089-2680.2.3.271]
Gyurak, A., Gross, J. J., & Etkin, A. (2011). Explicit and implicit emotion regulation: A dual-process framework. Cognition and emotion, 25(3), 400-412. [DOI: bs/10.1080/02699931.2010.544160]
Hasani, J. (2011). [Examining the reliability and validity of the short form of the cognitive emotion regulation questionnaire (Persian)]. Journal of Behavioral Science Research, 4(9), 229-240. [Link]
Hashemi Rezini, H., Bahashmat Joibari, S., & Rameshni, M. (2017). [Relationship between coping strategies and locus of control with the anxiety of death in old people.(Persian)]. Salmand: Iranian Journal of Ageing, 12(2), 232-241. [DOI:10.21859/ sija-1202232]
Jowkar, B. (2007). [The mediating role of resilience in the relationship between general and emotional intelligence and life satisfaction (Persian)]. Contemporary Psychology, 2(2 (4)), 3-12. [Link]Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer Press. [Link]
Mesraabadi J., Jafarian, S., & Ostovar, N. (2013). [Construct and diagnostic validity of the meaning in life questionnaire among university students (Persian)]. Journal of Behavioral Sciences, 7(1), 83-90. [Link]
Meyers,L.S , Gamest.G., & Goarin,A.J. (2006). Applied multivariate research, design and interpretation. London: Sage publication. [Link]
Nemiah, J. C. (2000). A psychodynamic view of psychosomatic medicine. Psychosomatic Medicine, 62(3), 299-303. [DOI:10.1097/00006842-200005000-00001] [PMID]
Osborne, J. W. (2017). An existential perspective on death anxiety, retirement, and related research problems. Canadian Journal on Aging/La Revue Canadienne du Vieillissement, 36(2), 246-255. [DOI: 10.1017/S0714980816000465]
Rajabi, G., Maghami, E., & Karami, J. (2019). [The role of proactive coping in psychological well-being: A study of Iranian students (Persian)]. Journal of Psychological Studies, 15(3), 45-60. [Link]
Rahmani, M., Darvishpour, A., & Pourghane, P. (2020). Application of MoCA, MMSE and AMTs tests in diagnosing the cognitive status of the elderly under hemodialysis in Medical centers of Guilan University of Medical Sciences in 2019. Journal of Gerontology, 5(3), 64-76. [Link]
Rezaei, S., Ahmadi, S., Rahmati, J., Hosseinifard, H., Dehnad, A., & Aryankhesal, A., et al. (2019). Global prevalence of depression in HIV/AIDS: A systematic review and meta-analysis. BMJ supportive & palliative care, 9(4), 404–412. [DOI:10.1136/bmjspcare-2019-001952] [PMID]
Rezaei, M., Karimi, F., & Ghasemi, A. (2021). Cultural influences on coping strategies among Iranian adults. Journal of Cross-Cultural Psychology, 52(4), 567–582.
Steger, M. F., Frazier, P., Oishi, S., & Kaler, M. (2006). The meaning in life questionnaire: assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53(1), 80-93. [DOI:10.1037/0022-0167.53.1.80]
Templer, D. I. (1970). The construction and validation of a death anxiety scale. The Journal of General Psychology, 82(2), 165-177. [DOI:10.1080/00221309.1970.9920634] [PMID]
Wong, P. T. P. (2008). Meaning management theory and death acceptance. In A. Tomer, G. T. Eliason, & P. T. P. Wong (Eds.), Existential and spiritual issues in death attitudes. New York: Psychology Press. [Link]
Type of Study: Original Research Article |
Subject:
Rehabilitation
Received: 2025/07/21 | Accepted: 2025/09/1 | Published: 2025/10/1
Received: 2025/07/21 | Accepted: 2025/09/1 | Published: 2025/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
