

Volume 12, Issue 1 (Winter 2024)
PCP 2024, 12(1): 81-94 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ebrahimi S, Moheb N, Alivani Vafa M. Comparison of the Effectiveness of Cognitive-behavioral Therapy and Acceptance and Commitment Therapy on Cognitive Distortions and Rumination in Adolescents With Social Anxiety Disorder. PCP 2024; 12 (1) :81-94
URL: http://jpcp.uswr.ac.ir/article-1-903-en.html
URL: http://jpcp.uswr.ac.ir/article-1-903-en.html



1- Department of Psychology, Faculty of Education and Humanities, Tabriz Branch, Islamic Azad University, Tabriz, Iran.
2- Department of Clinical Psychology, Faculty of Medical Sciences, Tabriz Branch, Islamic Azad University, Tabriz, Iran. ,nmoheb36@gmail.com
2- Department of Clinical Psychology, Faculty of Medical Sciences, Tabriz Branch, Islamic Azad University, Tabriz, Iran. ,
Keywords: Cognitive behavioral therapy, Acceptance, and commitment therapy, Cognitive distortion, Rumination, Social anxiety disorder
Full-Text [PDF 608 kb]
(3750 Downloads)
| Abstract (HTML) (5949 Views)
Full-Text: (2665 Views)
Introduction
Adolescence is a vulnerable period where many psychiatric conditions can develop, including social anxiety disorder (SAD) (Hyett & McEvoy, 2018). SAD is a debilitating condition characterized by an intense fear of negative judgment from others (Hyett & McEvoy, 2018). Avoiding social interactions, which is often used as a coping mechanism for social anxiety, can be particularly damaging during adolescence as it hinders important learning experiences from peer interactions. Social anxiety can be considered an “adolescent disorder” since the majority of severe and long-lasting cases tend to begin during mid-adolescence, with an average age of onset at 13 years old (Jefferies & Ungar, 2020). It is worth noting that this disorder ranks as the third most prevalent mental health condition, following depression and substance abuse, with approximately 12% of people experiencing it at some point in their lives. It can cause significant issues for the people unless treatment is not provided. Studies showed that SAD is perpetuated by cognitive distortion and rumination. Patterns of thoughts, beliefs, and cognitions play an important role in social anxiety. These patterns of thinking tend to lead them to avoid social interactions. In this regard, one of the most widely accepted models is the cognitive behavioral model which is used in explaining social anxiety (Mohammadi et al., 2020).
Cognitive models of anxiety disorders operate by focusing on key aspects such as cognitive schema or beliefs that lead individuals to process information with bias, concentrate solely on threats, and interpret ambiguous stimuli in a catastrophizing manner. In dynamic environments, various clinical presentations may emerge due to dysfunctional beliefs and distorted thinking patterns (Cuijpers et al., 2019). According to the cognitive model of social anxiety disorder (SAD), the core of social anxiety seems to stem from a strong desire to present oneself favorably to others and a deep insecurity about one’s ability to do so. Individuals with high social anxiety possess maladaptive thoughts and beliefs about their actions and how others judge them, leading to cognitive errors through consistent misinterpretation of their experiences (Stein, 2015). Additionally, cognitive models suggest that similar unproductive cognitive processes occur during social situations, as well as when an individual anticipates or reflects on the situation afterward (Takishima-Lacasa et al., 2014). This means that the processes that contribute to ongoing social anxiety should also be present when someone with SAD engages in pre- and post-event rumination. Researchers have developed structural equation models that generally support the connection between cognitive processes proposed by models of SAD for immediate anxiety and post-event rumination (Hovenkamp-Hermelink et al., 2019).
Several effective treatments are used for SAD, such as cognitive behavioral therapy (CBP), drug therapy, and social skills training (Karimpour-Vazifehkhorani et al., 2020). A meta-analysis of the effectiveness of drug treatments on SAD has provided little empirical support for these treatments (Mallorquí-Bagué et al., 2016). The main focus in treating this disorder is (CBT). Cognitive-behavioral models in treating SAD emphasize the role of negative cognitions, bias in the information-processing process, and avoidance behaviors in maintaining this disorder (Weiner et al., 2015). Several evidence-based CBT treatments for SAD have been proposed (Aderka et al., 2013; Kuru et al., 2018; Smith et al., 1994). Aderka et al (2013) showed that CBT could significantly affect fear, avoidance, and physiological symptoms in patients with SAD. Based on CBT can reduce anxiety symptoms (AS) and social anxiety symptoms in students with social anxiety. Some studies (Beck, 1993; Smith et al., 1994) indicate the effectiveness of CBT on SAD symptoms in general and cognitive distortions, rumination specifically. Although many of these treatments do not directly target AS, they have positively affected various aspects of this construct. However, some studies report the slight effectiveness of CBT in reducing SAD symptoms, particularly in adolescents (Karimpour Vazifehkhorani et al., 2023). Even though the effectiveness of these treatments has been shown, between 40 and 50% of these patients have not responded to treatment or symptoms remain, and people continue to experience symptoms after cognitive-behavioral interventions (Karimpour Vazifehkhorani et al., 2017). Acceptance and commitment therapy (ACT) has emerged as a promising treatment for anxiety disorders due to its effectiveness in reducing AS (Sharp, 2012). The therapeutic approach of ACT comprises six central processes that aim to promote psychological flexibility. These processes include acceptance, cognitive dissonance, present moment awareness, self-as-context, values clarification, and committed action (Sharp, 2012). The core principle of ACT is that people tend to experience distressing thoughts, emotions, and feelings, and their attempts to control or eliminate these experiences are often ineffective, leading to increased frustration and avoidance behaviors. (Sharp, 2012). The goal of this treatment is to reduce experiential avoidance along with increasing psychological flexibility. Also, therapy based on acceptance and commitment helps clients to create a rich, complete, and meaningful life (Beck, 1993). A meta-analysis (Swain et al., 2013) indicates higher-than-average effectiveness of the treatment based on acceptance and commitment to the symptoms of anxiety disorders in general and SAD in particular. Khoramnia et al. (2020) indicated the positive effects of ACT on a random group of social anxiety sufferers. Patients showed a significant reduction in externalized shame and emotion regulation. Wong (2008) concluded that treatment based on acceptance and commitment plays an important and influential role in improving the quality of life of SAD patients.
Despite the many types of research conducted in the field of SAD treatment, there are many ambiguities and shortcomings in these studies. The research about the effectiveness of CBT in reducing SAD symptoms has contradictions, and the results in this area must be more consistent. Effectiveness studies targeting symptoms of cognitive distortions, rumination, and anxiety sensitivity in adolescents are very few and insufficient. On the other hand, the effect of ACT on these symptoms in SAD has no research history. Further, only a few studies compare the effectiveness of CBT, and ACT treatment approaches in reducing these symptoms. Moreover, a few studies (Arch et al., 2012; Jiménez, 2012; Karimpour Vazifehkhorani et al., 2023) conducted in this area have considered the comparison in reducing SAD symptoms in general. According to these studies, answering these questions, such as Can CBT and ACT treatment effectively reduce the symptoms of cognitive distortions, rumination, and anxiety sensitivity in adolescents? Is inevitable. Moreover, in this regard, the question raised after answering this question and the central question of the present study is whether there is a difference between CBT and therapy based on acceptance and commitment in reducing cognitive distortions, rumination, and anxiety sensitivity. Is there a difference in adolescents with clinical symptoms of social anxiety?
Materials and Methods
Model and study group
The present study was semi-experimental including pre-test and post-test with a control group design. The statistical population was 15- to 18-year-old adolescents. They were identified and recruited through psychological service offices in Bukan City, Iran, between April 4th, 2022, and September 6th, 2022. They were selected by the purposive sampling method and randomly assigned to experimental groups and control groups. The research sample consists of 45 adolescents with the diagnosis of SAD who contributed to the study. A total of 45 adolescents participated in the study, 15 from the first experimental group, 15 from the second experimental group, and 15 from the control group. The sample size was determined using G*Power statistical software with an effect size of 0.25, a significance level of 0.05, a test power of 0.91, and a group size of three (n=15) (Ghasemi et al., 2023). The participants were randomly assigned to three groups: Experimental group 1 (15 students) received training in (CBT), experimental group 2 (15 students) received training in acceptance and commitment therapy (ACT), and the control group (15 students) did not receive any training. The inclusion criteria were having an age range of 15 to 18; having an active medical record with a diagnosis of SAD; diagnosis of SAD based on the diagnostic and statistical manual of mental disorders, the fifth edition (DSM-5) diagnostic interview, and completing the informed consent. The exclusion criteria were having a comorbid psychological disorder based on a structured clinical interview for DSM-5, and being absent in two or more therapy sessions.
Data collection tools
Structured clinical interview for DSM-5: To diagnose SAD, a diagnostic interview based on DSM-5, i.e. a structured clinical interview for DSM-5 (SCID-5) conducted by a clinical psychologist was used. The diagnostic interview is a semi-structured interview based on the DSM-5 This interview has two main parts: A personal history and b: Mental status examination. The first part of this interview includes individual characteristics, chief complaint, current problem, previous illness, and personal and family history. The second part comprises the examination of appearance, perception, cognition, thinking, judgment, and insight. This interview is consistent with the comprehensive psychiatric interview model (Joyce-Beaulieu & Sulkowski, 2015).
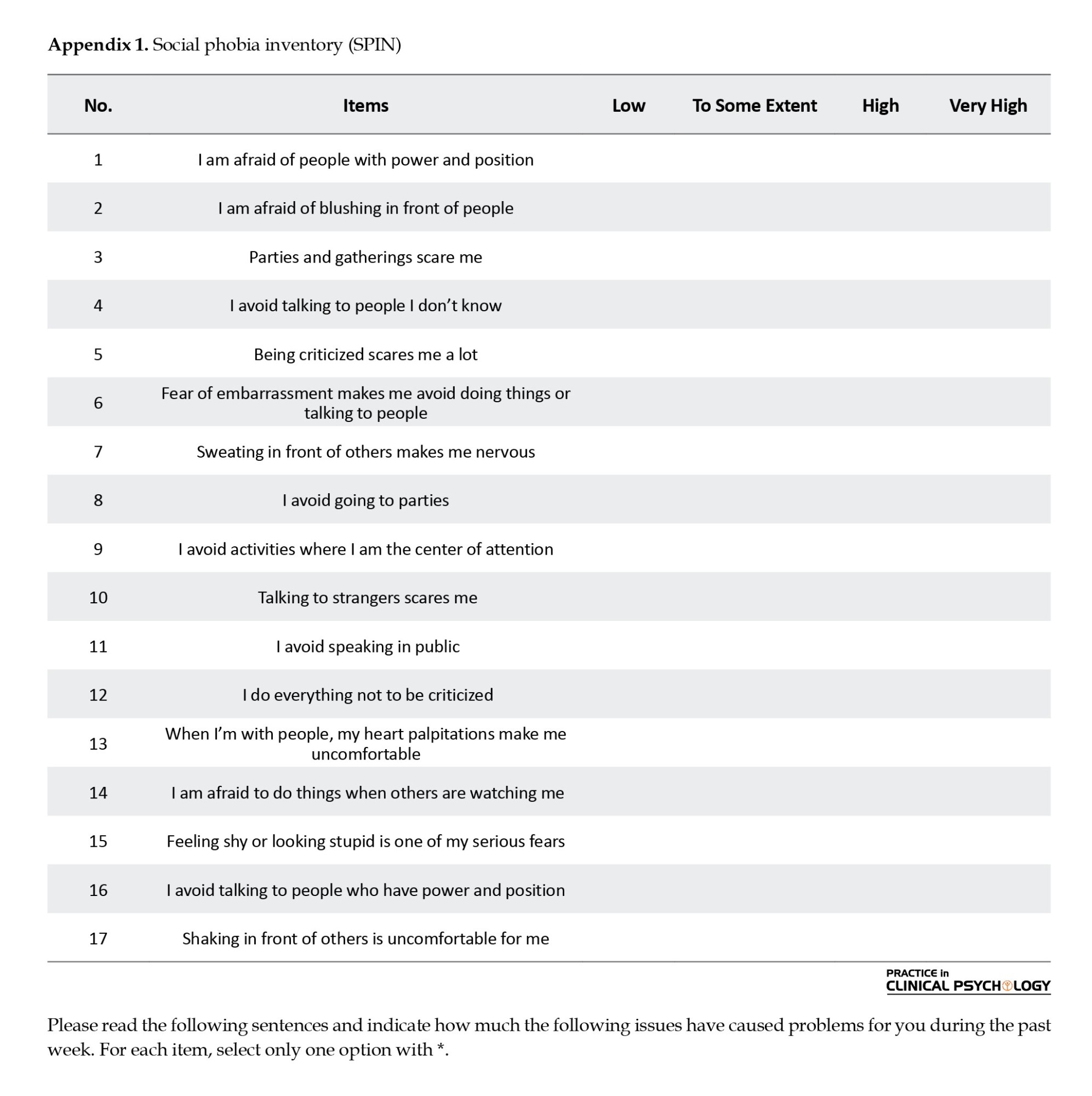
Social phobia inventory (SPIN): The amount of social anxiety was measured by the social anxiety questionnaire, which is a 17-item self-assessment scale, and its total score is in the range of 0 to 68. This questionnaire was designed in 2000 by Connor and his colleagues to evaluate social anxiety (Appendix 1). Its advantage is being sensitive to reducing social anxiety symptoms over time. One of its uses is to test the response to treatment in people with SAD. Scores above 51 indicate severe social anxiety; scores between 41 and 50 are considered moderate, 21 to 30 are considered low, and less than 20 are considered normal. A cut-off point of 40 with an efficiency of 80% and a cut-off point of 50 with an efficiency of 89% differentiates people with social anxiety from those without it (Connor et al., 2000). The validity of this questionnaire with the retest method in groups diagnosed with an SAD is equal to 0.78 to 0.89. Its internal consistency coefficient (Cronbach alpha) is 0.94 in a normal group. In Iran, this questionnaire was measured regarding psychometric characteristics in three groups suffering from social anxiety, other anxiety, and normal subjects. In a study by Tavoli et al (2012), the Cronbach alpha of the questionnaire was 0.88 with a reliability coefficient of 0.87. Also, onnor et al., (2000) reported the content validity ratio (CVR) and content validity index (CVI) at 0.77 and 0.82, respectively. In the Persian version, Rezaian et al. (2019) reported the CVR and CVI at 0.75 and 0.87, respectively.
The Ruminative Response Scale (RRS): The RRS is a self-report questionnaire, which includes 22 items describing responses to depressed mood (Treynor et al., 2003). Answers can be acting or thinking about the depressive symptoms and the possible causes and consequences of the sad/depressed mood. Items are rated on a 4-point scale (rarely to almost always). A total score can be calculated by summing all 22 item scores. The range of scores of this questionnaire varies between 22 and 88. The total score of rumination is calculated through the sum of the items. For this scale, the alpha coefficient at time 1 was 0.90 and the test-retest correlation was 0.67 (Treynor et al., 2003). Moreover, Treynor et al. (2003) reported CVR and CVI at 0.72 and 0.89, respectively. Falsafi & DashtBozorgi, (2019) found the Persian version with a CVR of 0.76 and a CVI of 0.88.
Dysfunctional attitude scale (DAS) (Falsafi & DashtBozorgi, 2019): The DAS is a 26-item instrument designed to identify and measure cognitive distortions, particularly those that may relate to or cause depression (Weissman & Beck, 1978). The items on the DAS are based on Beck’s cognitive therapy model and present seven major value systems: Approval, Love, Achievement, Perfectionism, Entitlement, Omnipotence, and Autonomy. For any missing items, a score of zero will be assigned (Appendix 2). The scores on all items (ranging from 1 to 7) are added to obtain the overall score. When no items are omitted, scores on the DAS go from 40 to 280. Lower scores represent more adaptive beliefs and fewer cognitive distortions. The DAS has good internal consistency, with alphas ranging from 0.84 to 0.92. The DAS is also reliable, with test-retest correlations over eight weeks of 0.80 to 0.84. The questionnaire has excellent concurrent validity, significantly correlating with several other measures of depression, including the Beck depression inventory (BDI). Also, Weissman & Beck, (1978) reported the CVR and CVI at 0.79 and 0.85, respectively. The DAS also significantly distinguishes between groups diagnosed as depressed or not depressed on the BDI. Toghyani (2014) reported CVR and CVI 0.78 and 0.86, respectively for the Persian version of DAS.
Procedure
After obtaining the necessary permissions for the research, the sample was divided into three groups, with each group comprising 15 adolescents. Before the research, participants provided written informed consent. The SPIN, the RRS, and the DAS (Falsafi & DashtBozorgi, 2019) were administered to all groups before the training sessions (pre-test). The CBT group received twelve 60-minute sessions, the ACT group received eight 60-minute sessions, and the control group was placed on a waiting list. All therapy sessions were conducted by a registered clinical psychologist with a PhD. After the treatment sessions, post-test assessments were conducted using the research instruments for both the intervention groups and the control group. Table 1 provides an overview of the treatment sessions. (Heimberg, 2002; Herbert et al., 2018) (Figure 1).


Data analysis
The study utilized descriptive and inferential statistics for data analysis. To examine the research hypothesis, an analysis of covariance (ANCOVA) was conducted using SPSS software,version 23. The significance level was set at 0.05. Before analysis, the data was checked to ensure that they met the basic assumptions of ANOVA. This included examining the normal distribution of scores and homogeneity of variance and covariance matrices (homoscedasticity) to confirm the assumption of a normal distribution of student engagement and academic resilience scores in the three study groups. Mauchly’s sphericity test was also used to check if the assumption of homoscedasticity was met. Levene’s and Box’s M tests were employed to validate the assumption of equivalence of covariances and student engagement and academic resilience variances. The results confirmed the homogeneity of variances, and Mauchly’s test verified the assumption of sphericity. Ultimately, the Box’s M test indicated the equivalence of covariances in the intervention and control groups, leading to the conclusion that the assumptions for conducting ANOVA were met.
Results
In the present study, there were 45 subjects in two experimental groups and one control group. Based on the demographic findings, the mean age in the CBT group was 15.99±3.16, in the ACT group it was 16.12±3.14, and in the control group, it was 16.16±3.19 with no significant difference between them (P=0.48). Also, 65% (n=29) of participants were female and 30% (n=16) were male. Moreover, 48% (n=21) of participants reported an average socioeconomic status (SES), 30% (n=14) of the participants announced a low SES, and 22% (n=10) declared a good SES.
Comparison of mean and standard deviation in research variables showed that the implementation of CBT in the first experimental group made significant differences between the pre-test and post-test in success-perfectionism (33.21±2.90, 28.76±3.48, P<0.001), need for others’ approval (28.30±2.80, 24.99±2.99, P<0.001), need to satisfy others (17.92±2.30, 14.68±2.71, P<0.001), vulnerability-function evaluation (18.88±3.72, 15.49±3.61, P<0.001), total score of the cognitive distortions (98.32±7.44, 83.90±7.77, P<0.001), and rumination (54.76±13.88, 49.51±13.42, P<0.001) (Table 2).

Also, the implementation of ACT on second experimental group made significant differences between pre-test and post-test in success-perfectionism (32.90±2.76, 29.77±3.40, P<0.001), need for others’ approval (28.44±3.04, 24.24±3.13, P<0.001), need to satisfy others (18.20±2.04, 15.26±2.18, P<0.001), vulnerability-function evaluation (18.91±3.68, 15.86±3.61, P<0.001), total score of the cognitive distortions (98.70±7.02, 85.13±6.83, P<0.001), and rumination (52.33±17.78, 47.73±14.23, P<0.001).
Moreover, there were no significant differences between the pre-test and post-test in the control group in success-perfectionism (33.21±2.57, 33.36±2.48, P>0.05), need for others’ approval (28.02±2.83, 27.84±3.13, P>0.05), need to satisfy others (17.51±2.65, 17.59±2.63, P=0.28), vulnerability-function evaluation (19.08±3.36, 18.89±3.59, P>0.05), total score of the cognitive distortions (97.83±6.98, 97.69±7.20, P>0.05), and rumination (54.75±13.65, 54.71±13.60, P>0.05) (Table 2). A pairwise comparison was used to determine the nature of the changes made, as reported in Table 3.

The results in Table 3 showed that in the post-test stage, there is no statistically significant difference between the groups of CBT and ACT; however, there is a statistically significant difference between these two experimental groups and the control group (P<0.001). There was no significant difference between the effectiveness of CBT and ACT in success-perfectionism (MD=-0.853, P>0.05), need for others’ approval (MD=0.890, P>0.05), need to satisfy others (MD=-0.323, P>0.05), vulnerability-function evaluation (MD=-0.654, P>0.05), the total score of the cognitive distortions (MD=-0.981, P>0.05), and rumination (MD=-0.601, P>0.05). Furthermore, there was a significant difference between CBT and control group in success-perfectionism (MD=4.860, P<0.001), need for others’ approval (MD=3.355, P<0.001), Need to satisfy others (MD=3.301, P<0.001), vulnerability-function evaluation (MD=3.361, P<0.001), total score of the cognitive distortions (MD=14.911, P<0.001) and rumination (MD=5.261, P<0.001). Moreover, there was a significant difference between ACT and the control group in success-perfectionism (MD=4.007, P<0.001), need for others’ approval (MD=4.244, P<0.001), need to satisfy others (MD=2.978, P<0.001), vulnerability-function evaluation (MD=2.707, P<0.001), total score of the cognitive distortions (MD=13.931, P<0.001) and rumination (MD=4.660, P<0.001).
Discussion
The current study compared the effectiveness of cognitive-behavioral and acceptance and commitment therapy on SAD symptoms, including cognitive distortions and rumination among adolescents with SAD. Although results showed that CBT and ACT treatments had a significant effect on the dependent variables, there is no significant difference between CBT and ACT treatments in influencing the mentioned dependent variables. In this regard, several studies (Rahmanian et al., 2020; Rezayi et al., 2017; Soltanizadeh et al., 2019) showed that CBT has a significant effect on social anxiety symptoms in adolescents with SAD. Herbert et al., (2018) showed that those who received CBT evidenced greater improvements in self-reported social anxiety symptoms and overall functioning. Also, some studies (Azar et al.; Esmaeili et al., 2018; Pourfarahani et al., 2020) showed that ACT has been effective on social anxiety and its components in adolescents.
Previous studies (Herbert et al., 2018; Zohdi et al., 2022) showed that there is no difference between CBT and ACT in the treatment of social anxiety. In a study conducted by Herbert et al., 2018, it was found that although the difference was not statistically significant, the ACT participants showed greater improvements in observer-rated social behavior in comparison to the CBT participants with a medium effect size. This disparity in the symptoms and behavioral outcomes, which is consistent with prior research, highlights the need for further investigation to examine the variations between CBT and ACT treatments regarding behavioral domains.
The present study found that cognitive distortions and rumination were significantly reduced in adolescents with SAD after undergoing CBT and ACT. CBT helps individuals with social anxiety by modifying cognitive distortions through restructuring, social skills training, and confronting their avoidance (Leigh & Clark, 2018). CBT can help those with social anxiety by altering their dysfunctional and distorted beliefs. Anxiety disorder patients commonly have 3 types of beliefs: Setting very high standards for themselves, conditional beliefs, and irrational beliefs about themselves. These beliefs lead to viewing the world as dangerous and avoiding social situations. Cognitive distortions in those with social anxiety disorder can significantly affect their interpretation of social situations and their solutions to social problems. These cognitive errors can lead to the growth and sustainability of their social anxiety. (Leigh & Clark, 2018).
CBT reduces cognitive distortions in SAD patients by preparing a hierarchical list of anxiety-causing situations, regular exercises to confront those situations, evaluating their cognitive distortions, and changing those maladaptive distorted thoughts into more adaptive ones (Leichsenring et al., 2013). Cognitive behavioral therapy is designed to engage and replace negative biases in information processing, negative self-evaluations of social functioning, and the need for other people’s affirmation. It also reduces pathological self-focused attention (Heimberg, 2002). Also, self-focused attention makes SAD individuals perceive their internal physical states, such as heartbeat, thoughts, and feelings, to have a direct representation outside. Therefore, this therapy prevents objective information processing in social situations and emphasizes facing social problems despite having feelings of anxiety by helping them understand its symptoms and encouraging them to increase their social function in social environments and reduce their avoidant lifestyles, protective behaviors, and distortions. Therefore, facing social situations acts as a behavioral test to prove or reject the cognitive hypotheses of people suffering from social anxiety, eventually leading to cognitive distortion modification (Heimberg, 2002).
On the other hand, ACT draws people’s attention to two fundamental aspects of their inner reality: 1) Trying to get close to people and pursuing life’s core values, and 2) Trying to get away from maladaptive thoughts and emotions. In other words, recognizing values and moving in the path of values promotes their psychological flexibility, and experiencing new committed behaviors that even can be against their will encourages them to move in a direction that continues to challenge their maladaptive beliefs and pulls them away from having those thoughts and emotions by gradual modification of them (Otte, 2022).
The fundamental belief in acceptance and commitment therapy for SAD individuals is that psychological distress is caused by experience avoidance, cognitive fusion, failure to meet behavioral needs, and incongruence with one’s core values (Khoramnia et al., 2020). Reducing symptoms is not the therapist’s goal but a byproduct of the treatment process. ACT changes the relationship between irrational thoughts and emotions so that the individual understands them as pathological symptoms and even learns to change them if they are uncomfortable and unpleasant. The general goal of ACT is to reduce the literal perception of the cognitive content that prevents behavior and to increase the probability of positive events by replacing correct cognitions (Sharp, 2012). Therefore, treatment based on acceptance and commitment can be used as one of the effective psychological treatments to reduce cognitive distortions by increasing a person’s psychological flexibility and connection with the present and encouraging him to move toward his values. The reason for the effect of treatment based on acceptance and commitment to cognitive distortions is that this approach targets the function of cognitions and emotions instead of changing the frequency or situational sensitivity. Changing the function of cognition and emotion seems more manageable than changing their form and content. The change in function is more objective than the change in the form and content of cognition and emotions, and the person has a sense of control over the function of cognition and emotions (Niles et al., 2014).
The results of the present study showed that cognitive behavioral therapy and acceptance and commitment-based therapy effectively reduce rumination in adolescents with SAD. In the explanation of the findings, rumination can be one of the characteristics of people with symptoms of anxiety disorders, and this issue continuously increases anxiety; On the other hand, CBT helps to change the content of mental rumination through the detection of cognitive errors, challenging them and conducting behavioral tests (Leichsenring et al., 2013). Also, CBT modifies the cognitive schemas that cause the continuation of negative emotions and strengthens negative beliefs in these individuals through organizing thought processes, emotional problems, and concerns associated with anxiety (avoidance, dependency, helplessness towards change, and rumination responses).
According to Ghasemi et al., (2023), psychological disorders can result from a lack of psychological flexibility, which is the central premise of ACT. ACT posits that individuals often view certain emotions and inner thoughts as distressing and attempt to eliminate or alter them. However, such efforts at emotional control are counterproductive, as they exacerbate the very emotions and thoughts that the individual is attempting to avoid. Consequently, the primary issue for patients in ACT is avoidance. The central process of ACT teaches people how to stop inhibiting thoughts, not to confuse them with disturbing thoughts, and makes them more tolerant of unpleasant emotions (Esmaeili et al., 2018). ACT therapy is based on pervasive awareness or mindfulness. In this method, mindfulness means consciously bringing awareness to the experience of the here and now with openness, interest, acceptance, and not being distracted by thoughts. During the research, Yabandeh et al. (2019) showed that conscious attention to the present moment and the ability to control attention effectively prevent rumination. In general, the main goal of the ACT approach is for the person to create a productive and meaningful life by achieving psychological flexibility and effectively controlling the pains, sufferings, and tensions that life has inevitably caused him, which will reduce rumination. People who are cognitively inflexible turn to rumination when upset and focus their energy and thoughts on rumination, which brings a repetitive and unhelpful response to the person (Yabandeh et al., 2019).
Conclusion
ACT is an effective treatment for anxiety and cognitive distortions. This therapy approach helps in developing psychological flexibility by combining mindfulness skills with self-acceptance, which makes it a form of behavioral therapy. ACT encourages people to open up to unpleasant feelings, learn to avoid overreacting, and not avoid situations that may trigger them. On the other hand, CBT targets the cognitive, behavioral, and physiological mechanisms. It helps in restructuring maladaptive thought patterns, correcting misinterpretations, changing attentional focus, and developing adaptive coping thoughts, which can lead to an increase in adaptive cognitions. Additionally, CBT can help in habituation, extinction of maladaptive responses, behavioral activation, associative learning, and reinforcement of adaptive responding for an increase in adaptive behavioral responses. Normalization of physiological arousal is also possible with CBT through habituation, incompatible response training, and changes in autonomic nervous system activity.
Limitations
Although the psychology centers initially offered their full and free cooperation, they later requested a fee to continue the research process during the intervention and our budget constraints posed challenges for us in this regard. Moreover, the parents of some adolescents disagreed with continuing to participate in the research.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the regional ethics committee (Code: IR.IAU.TABRIZ.REC.1401.239).
Funding
The paper was extracted from thePhD. thesis of Shirin Ebrahimi, Department of Psychology, Faculty of Human Science, Tabriz Branch, Islamic Azad University, Tabriz, East Azerbaijan, Iran.
Authors' contributions
All authors equally contributed to all parts of the study.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to thank all the participants who participated in this study.
References
Aderka, I. M., McLean, C. P., Huppert, J. D., Davidson, J. R., & Foa, E. B. (2013). Fear, avoidance and physiological symptoms during cognitive-behavioral therapy for social anxiety disorder. Behaviour Research and Therapy, 51(7), 352–358.[DOI:10.1016/j.brat.2013.03.007] [PMID]
Arch, J. J., Eifert, G. H., Davies, C., Plumb Vilardaga, J. C., Rose, R. D., & Craske, M. G. (2012). Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders. Journal of Consulting and Clinical Psychology, 80(5), 750–765. [DOI:10.1037/a0028310] [PMID]
karimiazar, F., Saken Azari, R., Abdoltajedini, P., & Azmoudeh, M. (2022). [The effect of acceptance and commitment based therapy on the symptoms of social anxiety in shy girls adolescents (Persian)]. Nursing Psychiatric of Journal Iranian, 10(1), 46-54
Beck A. T. (1993). Cognitive therapy: Past, present, and future. Journal of Consulting and Clinical Psychology, 61(2), 194–198.[DOI:10.1037/0022-006X.61.2.194] [PMID]
Connor, K. M., Davidson, J. R., Churchill, L. E., Sherwood, A., Weisler, R. H., & Foa, E. (2000). Psychometric properties of the Social Phobia Inventory (SPIN): New self-rating scale. The British Journal of Psychiatry, 176(4), 379-386. [DOI:10.1192/bjp.176.4.379] [PMID]
Cuijpers, P., Auerbach, R. P., Benjet, C., Bruffaerts, R., Ebert, D., & Karyotaki, E., et al. (2019). The world health organization world mental health international college student initiative: an overview. International Journal of Methods in Psychiatric Research, 28(2), e1761. [DOI:10.1002/mpr.1761]
Esmaeili, L., Amiri, S., Reza Abedi, M., & Molavi, H. (2018). [The effect of acceptance and commitment therapy focused on self-compassion on social anxiety of adolescent girls (Persian)]. Clinical Psychology Studies, 8(30), 117-137. [Link]
Falsafi, A., & DashtBozorgi, Z. (2019). The effect of mindfulness training on rumination, body image, and sexual satisfaction in women with recurrent pregnancy loss (Persian)]. Iranian Journal of Rehabilitation Research, 5(3), 48-54. [Link]
Ghasemi, F., Emadian, S. O., & Hasanzadeh, R. (2023). Comparison of the effectiveness of mindfulness training and internet-based acceptance and commitment training on academic engagement, mental time travel, and students’ anxiety during the COVID-19 pandemic. International Journal of School Health, 10(2):82-91. [DOI:10.30476/intjsh.2023.97316.1267]
Heimberg R. G. (2002). Cognitive-behavioral therapy for social anxiety disorder: Current status and future directions. Biological Psychiatry, 51(1), 101–108. [DOI:10.1016/S0006-3223(01)01183-0] [PMID]
Herbert, J. D., Forman, E. M., Kaye, J. L., Gershkovich, M., Goetter, E., & Yuen, E. K., et al. (2018). Randomized controlled trial of acceptance and commitment therapy versus traditional cognitive behavior therapy for social anxiety disorder: Symptomatic and behavioral outcomes. Journal of Contextual Behavioral Science, 9, 88-96. [DOI:10.1016/j.jcbs.2018.07.008]
Hovenkamp-Hermelink, J. H. M., van der Veen, D. C., Oude Voshaar, R. C., Batelaan, N. M., Penninx, B. W. J. H., & Jeronimus, B. F., et al. (2019). Anxiety sensitivity, its stability and longitudinal association with severity of anxiety symptoms. Scientific Reports, 9(1), 4314. [DOI:10.1038/s41598-019-39931-7] [PMID]
Hyett, M. P., & McEvoy, P. M. (2018). Social anxiety disorder: Looking back and moving forward. Psychological Medicine, 48(12), 1937–1944. [DOI:10.1017/S0033291717003816] [PMID]
Jefferies, P., & Ungar, M. (2020). Social anxiety in young people: A prevalence study in seven countries. Plos One, 15(9), e0239133. [DOI:10.1371/journal.pone.0239133] [PMID]
Ruiz, F. J. (2012). Acceptance and commitment therapy versus traditional cognitive behavioral therapy: A systematic review and meta-analysis of current empirical evidence. International Journal of Psychology and Psychological Therapy, 12(2), 333-357. [Link]
Joyce-Beaulieu, D., & Sulkowski, M. L. (2015). Cognitive behavioral therapy in K-12 school settings: A practitioner’s toolkit. New York: Springer Publishing Company. [Link]
Karimpour-Vazifehkhorani, A., Bakhshipour Rudsari, A., Rezvanizadeh, A., Kehtary-Harzang, L., & Hasanzadeh, K. (2020). Behavioral activation therapy on reward seeking behaviors in depressed people: An experimental study. Journal of Caring Sciences, 9(4), 195–202. [DOI:10.34172/jcs.2020.030] [PMID]
Karimpour Vazifehkhorani, A., Bakhsipour Roodsari, A., Reyhanimehr, Q., Kamali Ghasemabadi, H., Noroozi, H., & Shadara, Z., et al. (2017). [Comparing brain behavioral systems in couples engaged in infidelity and normal couples in Tabriz, Tehran, and Karaj (Persian)]. Depiction of Health, 8(2), 97-103. [Link]
Karimpour Vazifehkhorani, A., Jafari, M. R., & Rahmati, F. (2023). The effectiveness of acceptance and commitment therapy training on health promoting lifestyle profile among soldiers. Iranian Journal of Health Education and Health Promotion, 10(4), 350-360. [DOI:10.52547/ijhehp.10.4.350]
Khoramnia, S., Bavafa, A., Jaberghaderi, N., Parvizifard, A., Foroughi, A., & Ahmadi, M., et al. (2020). The effectiveness of acceptance and commitment therapy for social anxiety disorder: A randomized clinical trial. Trends in Psychiatry and Psychotherapy, 42(1), 30–38. [DOI:10.1590/2237-6089-2019-0003] [PMID]
Kuru, E., Safak, Y., Özdemir, İ., Tulacı, R., Özdel, K., & Özkula, N., et al. (2018). Cognitive distortions in patients with social anxiety disorder: Comparison of a clinical group and healthy controls. The European Journal of Psychiatry, 32(2), 97-104. [DOI:10.1016/j.ejpsy.2017.08.004]
Leichsenring, F., Salzer, S., Beutel, M. E., Herpertz, S., Hiller, W., & Hoyer, J., et al. (2013). Psychodynamic therapy and cognitive-behavioral therapy in social anxiety disorder: A multicenter randomized controlled trial. The American Journal of Psychiatry, 170(7), 759–767. [DOI:10.1176/appi.ajp.2013.12081125] [PMID]
Leigh, E., & Clark, D. M. (2018). Understanding Social anxiety disorder in adolescents and improving treatment outcomes: Applying the cognitive model of clark and wells (1995). Clinical Child and Family Psychology Review, 21(3), 388–414. [DOI:10.1007/s10567-018-0258-5] [PMID]
Mallorquí-Bagué, N., Bulbena, A., Pailhez, G., Garfinkel, S. N., & Critchley, H. D. (2016). Mind-body interactions in anxiety and somatic symptoms. Harvard Review of Psychiatry, 24(1), 53–60. [DOI:10.1097/HRP.0000000000000085] [PMID]
Mohammadi, M. R., Salehi, M., Khaleghi, A., Hooshyari, Z., Mostafavi, S. A., & Ahmadi, N., et al. (2020). Social anxiety disorder among children and adolescents: A nationwide survey of prevalence, socio-demographic characteristics, risk factors and co-morbidities. Journal of Affective Disorders, 263, 450–457. [DOI:10.1016/j.jad.2019.12.015] [PMID]
Niles, A. N., Burklund, L. J., Arch, J. J., Lieberman, M. D., Saxbe, D., & Craske, M. G. (2014). Cognitive mediators of treatment for social anxiety disorder: Comparing acceptance and commitment therapy and cognitive-behavioral therapy. Behavior Therapy, 45(5), 664–677. [DOI:10.1016/j.beth.2014.04.006] [PMID]
Otte C. (2011). Cognitive behavioral therapy in anxiety disorders: Current state of the evidence. Dialogues in Clinical Neuroscience, 13(4), 413–421. [DOI:10.31887/DCNS.2011.13.4/cotte] [PMID] [PMCID]
Pourfarahani, M., Barabadi, H. A., & Heydarnia, A. (2020). [The effectiveness of acceptance and commitment group therapy in the social anxiety of adolescent orphan girls (Persian)]. Quarterly Journal of Social Work, 8, 5-13. [Link]
Rahmanian, Z., Mirzaian, B., & Hassanzadeh, R. (2020). [Effectiveness of cognitive-behavioral group therapy on social anxiety of female students (Persian)]. Daneshvar Medicine, 19(5), 47-56. [Link]
Rezayi, F., Amiri, M., & Taheri, E. (2017). [Effectiveness of cognitive-behavioral group therapy on reducing social anxiety and negative cognitive evaluation among hard of hearing young girls (Persian)]. Counseling Culture and Psychotherapy, 8(32), 133-160. [DOI:10.22054/qccpc.2018.23065.1565]
Sharp, K. (2012). A review of acceptance and commitment therapy with anxiety disorders. International Journal of Psychology and Psychological Therapy, 12(3), 359-372. [Link]
Smith, T. W., O'Keeffe, J. L., & Christensen, A. J. (1994). Cognitive distortion and depression in chronic pain: Association with diagnosed disorders. Journal of Consulting and Clinical Psychology, 62(1), 195–198. [DOI:10.1037/0022-006X.62.1.195] [PMID]
Soltanizadeh, M., Montazeri, M., & Latifi, Z. (2019). [Effectiveness of cognitive-behavioral therapy in social anxiety among children with type I diabetes mellitus (Persian)]. Journal of Health System Research, 15(3), 192-198. [DOI:10.32592/hsr.2020.15.3.102]
Stein D. J. (2015). Social anxiety disorder and the psychobiology of self-consciousness. Frontiers in Human Neuroscience, 9, 489. [DOI:10.3389/fnhum.2015.00489] [PMID]
Swain, J., Hancock, K., Hainsworth, C., & Bowman, J. (2013). Acceptance and commitment therapy in the treatment of anxiety: A systematic review. Clinical Psychology Review, 33(8), 965–978. [DOI:10.1016/j.cpr.2013.07.002] [PMID]
Takishima-Lacasa, J. Y., Higa-McMillan, C. K., Ebesutani, C., Smith, R. L., & Chorpita, B. F. (2014). Self-consciousness and social anxiety in youth: The revised self-consciousness scales for children. Psychological Assessment, 26(4), 1292–1306.[DOI:10.1037/a0037386] [PMID]
Tavoli, A., Allahyari, A., Azadfallah, P., Fathi Ashtiani, A., Melyani, M., & Sahragard, M. (2012). [Validity and reliability of the Farsi version of the social interaction anxiety scale (SIAS) (Persian)]. Iranian Journal of Psychiatry & Clinical Psychology, 18(3):227-232. [Link]
Toghyani, M. (2014). [The relationship of Islamic lifestyle with dysfunctional attitudes in university students (Persian)]. Knowledge & Research in Applied Psychology, 14(4), 35-43. [Link]
Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27, 247-259. [DOI:10.1023/A:1023910315561]
Weiner, C. L., Meredith Elkins, R., Pincus, D., & Comer, J. (2015). Anxiety sensitivity and sleep-related problems in anxious youth. Journal of Anxiety Disorders, 32, 66–72. [DOI:10.1016/j.janxdis.2015.03.009] [PMID]
Weissman, A. N., & Beck, A. T. (1978). Development and validation of the Dysfunctional Attitude Scale: A preliminary investigation. Paper presented at: the Annual Meeting of The American Educational Research Association, Torento, Canada, 1978. [Link]
Wong, S. S. (2008). The relations of cognitive triad, dysfunctional attitudes, automatic thoughts, and irrational beliefs with test anxiety. Current Psychology, 27, 177-191. [DOI:10.1007/s12144-008-9033-y]
Yabandeh, M. R., Bagholi, H., Sarvghad, S., & Kouroshnia, M. (2019). [Comparing the effectiveness of cognitive behavioral therapy with acceptance and commitment therapy on reduction of social anxiety disorder symptoms (Persian)]. Psychological Methods and Models, 10(36), 177-196. [Link]
Zohdi, Y., Mohammadkhani, P., & Karimpour-Vazifehkhorani, A. (2022). The role of Anhedonia and low arousal in substance use disorder among adolescents with conduct disorder symptoms. Practice in Clinical Psychology, 10(2), 111-120. [DOI:10.32598/jpcp.10.2.815.1]

Adolescence is a vulnerable period where many psychiatric conditions can develop, including social anxiety disorder (SAD) (Hyett & McEvoy, 2018). SAD is a debilitating condition characterized by an intense fear of negative judgment from others (Hyett & McEvoy, 2018). Avoiding social interactions, which is often used as a coping mechanism for social anxiety, can be particularly damaging during adolescence as it hinders important learning experiences from peer interactions. Social anxiety can be considered an “adolescent disorder” since the majority of severe and long-lasting cases tend to begin during mid-adolescence, with an average age of onset at 13 years old (Jefferies & Ungar, 2020). It is worth noting that this disorder ranks as the third most prevalent mental health condition, following depression and substance abuse, with approximately 12% of people experiencing it at some point in their lives. It can cause significant issues for the people unless treatment is not provided. Studies showed that SAD is perpetuated by cognitive distortion and rumination. Patterns of thoughts, beliefs, and cognitions play an important role in social anxiety. These patterns of thinking tend to lead them to avoid social interactions. In this regard, one of the most widely accepted models is the cognitive behavioral model which is used in explaining social anxiety (Mohammadi et al., 2020).
Cognitive models of anxiety disorders operate by focusing on key aspects such as cognitive schema or beliefs that lead individuals to process information with bias, concentrate solely on threats, and interpret ambiguous stimuli in a catastrophizing manner. In dynamic environments, various clinical presentations may emerge due to dysfunctional beliefs and distorted thinking patterns (Cuijpers et al., 2019). According to the cognitive model of social anxiety disorder (SAD), the core of social anxiety seems to stem from a strong desire to present oneself favorably to others and a deep insecurity about one’s ability to do so. Individuals with high social anxiety possess maladaptive thoughts and beliefs about their actions and how others judge them, leading to cognitive errors through consistent misinterpretation of their experiences (Stein, 2015). Additionally, cognitive models suggest that similar unproductive cognitive processes occur during social situations, as well as when an individual anticipates or reflects on the situation afterward (Takishima-Lacasa et al., 2014). This means that the processes that contribute to ongoing social anxiety should also be present when someone with SAD engages in pre- and post-event rumination. Researchers have developed structural equation models that generally support the connection between cognitive processes proposed by models of SAD for immediate anxiety and post-event rumination (Hovenkamp-Hermelink et al., 2019).
Several effective treatments are used for SAD, such as cognitive behavioral therapy (CBP), drug therapy, and social skills training (Karimpour-Vazifehkhorani et al., 2020). A meta-analysis of the effectiveness of drug treatments on SAD has provided little empirical support for these treatments (Mallorquí-Bagué et al., 2016). The main focus in treating this disorder is (CBT). Cognitive-behavioral models in treating SAD emphasize the role of negative cognitions, bias in the information-processing process, and avoidance behaviors in maintaining this disorder (Weiner et al., 2015). Several evidence-based CBT treatments for SAD have been proposed (Aderka et al., 2013; Kuru et al., 2018; Smith et al., 1994). Aderka et al (2013) showed that CBT could significantly affect fear, avoidance, and physiological symptoms in patients with SAD. Based on CBT can reduce anxiety symptoms (AS) and social anxiety symptoms in students with social anxiety. Some studies (Beck, 1993; Smith et al., 1994) indicate the effectiveness of CBT on SAD symptoms in general and cognitive distortions, rumination specifically. Although many of these treatments do not directly target AS, they have positively affected various aspects of this construct. However, some studies report the slight effectiveness of CBT in reducing SAD symptoms, particularly in adolescents (Karimpour Vazifehkhorani et al., 2023). Even though the effectiveness of these treatments has been shown, between 40 and 50% of these patients have not responded to treatment or symptoms remain, and people continue to experience symptoms after cognitive-behavioral interventions (Karimpour Vazifehkhorani et al., 2017). Acceptance and commitment therapy (ACT) has emerged as a promising treatment for anxiety disorders due to its effectiveness in reducing AS (Sharp, 2012). The therapeutic approach of ACT comprises six central processes that aim to promote psychological flexibility. These processes include acceptance, cognitive dissonance, present moment awareness, self-as-context, values clarification, and committed action (Sharp, 2012). The core principle of ACT is that people tend to experience distressing thoughts, emotions, and feelings, and their attempts to control or eliminate these experiences are often ineffective, leading to increased frustration and avoidance behaviors. (Sharp, 2012). The goal of this treatment is to reduce experiential avoidance along with increasing psychological flexibility. Also, therapy based on acceptance and commitment helps clients to create a rich, complete, and meaningful life (Beck, 1993). A meta-analysis (Swain et al., 2013) indicates higher-than-average effectiveness of the treatment based on acceptance and commitment to the symptoms of anxiety disorders in general and SAD in particular. Khoramnia et al. (2020) indicated the positive effects of ACT on a random group of social anxiety sufferers. Patients showed a significant reduction in externalized shame and emotion regulation. Wong (2008) concluded that treatment based on acceptance and commitment plays an important and influential role in improving the quality of life of SAD patients.
Despite the many types of research conducted in the field of SAD treatment, there are many ambiguities and shortcomings in these studies. The research about the effectiveness of CBT in reducing SAD symptoms has contradictions, and the results in this area must be more consistent. Effectiveness studies targeting symptoms of cognitive distortions, rumination, and anxiety sensitivity in adolescents are very few and insufficient. On the other hand, the effect of ACT on these symptoms in SAD has no research history. Further, only a few studies compare the effectiveness of CBT, and ACT treatment approaches in reducing these symptoms. Moreover, a few studies (Arch et al., 2012; Jiménez, 2012; Karimpour Vazifehkhorani et al., 2023) conducted in this area have considered the comparison in reducing SAD symptoms in general. According to these studies, answering these questions, such as Can CBT and ACT treatment effectively reduce the symptoms of cognitive distortions, rumination, and anxiety sensitivity in adolescents? Is inevitable. Moreover, in this regard, the question raised after answering this question and the central question of the present study is whether there is a difference between CBT and therapy based on acceptance and commitment in reducing cognitive distortions, rumination, and anxiety sensitivity. Is there a difference in adolescents with clinical symptoms of social anxiety?
Materials and Methods
Model and study group
The present study was semi-experimental including pre-test and post-test with a control group design. The statistical population was 15- to 18-year-old adolescents. They were identified and recruited through psychological service offices in Bukan City, Iran, between April 4th, 2022, and September 6th, 2022. They were selected by the purposive sampling method and randomly assigned to experimental groups and control groups. The research sample consists of 45 adolescents with the diagnosis of SAD who contributed to the study. A total of 45 adolescents participated in the study, 15 from the first experimental group, 15 from the second experimental group, and 15 from the control group. The sample size was determined using G*Power statistical software with an effect size of 0.25, a significance level of 0.05, a test power of 0.91, and a group size of three (n=15) (Ghasemi et al., 2023). The participants were randomly assigned to three groups: Experimental group 1 (15 students) received training in (CBT), experimental group 2 (15 students) received training in acceptance and commitment therapy (ACT), and the control group (15 students) did not receive any training. The inclusion criteria were having an age range of 15 to 18; having an active medical record with a diagnosis of SAD; diagnosis of SAD based on the diagnostic and statistical manual of mental disorders, the fifth edition (DSM-5) diagnostic interview, and completing the informed consent. The exclusion criteria were having a comorbid psychological disorder based on a structured clinical interview for DSM-5, and being absent in two or more therapy sessions.
Data collection tools
Structured clinical interview for DSM-5: To diagnose SAD, a diagnostic interview based on DSM-5, i.e. a structured clinical interview for DSM-5 (SCID-5) conducted by a clinical psychologist was used. The diagnostic interview is a semi-structured interview based on the DSM-5 This interview has two main parts: A personal history and b: Mental status examination. The first part of this interview includes individual characteristics, chief complaint, current problem, previous illness, and personal and family history. The second part comprises the examination of appearance, perception, cognition, thinking, judgment, and insight. This interview is consistent with the comprehensive psychiatric interview model (Joyce-Beaulieu & Sulkowski, 2015).
Social phobia inventory (SPIN): The amount of social anxiety was measured by the social anxiety questionnaire, which is a 17-item self-assessment scale, and its total score is in the range of 0 to 68. This questionnaire was designed in 2000 by Connor and his colleagues to evaluate social anxiety (Appendix 1). Its advantage is being sensitive to reducing social anxiety symptoms over time. One of its uses is to test the response to treatment in people with SAD. Scores above 51 indicate severe social anxiety; scores between 41 and 50 are considered moderate, 21 to 30 are considered low, and less than 20 are considered normal. A cut-off point of 40 with an efficiency of 80% and a cut-off point of 50 with an efficiency of 89% differentiates people with social anxiety from those without it (Connor et al., 2000). The validity of this questionnaire with the retest method in groups diagnosed with an SAD is equal to 0.78 to 0.89. Its internal consistency coefficient (Cronbach alpha) is 0.94 in a normal group. In Iran, this questionnaire was measured regarding psychometric characteristics in three groups suffering from social anxiety, other anxiety, and normal subjects. In a study by Tavoli et al (2012), the Cronbach alpha of the questionnaire was 0.88 with a reliability coefficient of 0.87. Also, onnor et al., (2000) reported the content validity ratio (CVR) and content validity index (CVI) at 0.77 and 0.82, respectively. In the Persian version, Rezaian et al. (2019) reported the CVR and CVI at 0.75 and 0.87, respectively.
The Ruminative Response Scale (RRS): The RRS is a self-report questionnaire, which includes 22 items describing responses to depressed mood (Treynor et al., 2003). Answers can be acting or thinking about the depressive symptoms and the possible causes and consequences of the sad/depressed mood. Items are rated on a 4-point scale (rarely to almost always). A total score can be calculated by summing all 22 item scores. The range of scores of this questionnaire varies between 22 and 88. The total score of rumination is calculated through the sum of the items. For this scale, the alpha coefficient at time 1 was 0.90 and the test-retest correlation was 0.67 (Treynor et al., 2003). Moreover, Treynor et al. (2003) reported CVR and CVI at 0.72 and 0.89, respectively. Falsafi & DashtBozorgi, (2019) found the Persian version with a CVR of 0.76 and a CVI of 0.88.
Dysfunctional attitude scale (DAS) (Falsafi & DashtBozorgi, 2019): The DAS is a 26-item instrument designed to identify and measure cognitive distortions, particularly those that may relate to or cause depression (Weissman & Beck, 1978). The items on the DAS are based on Beck’s cognitive therapy model and present seven major value systems: Approval, Love, Achievement, Perfectionism, Entitlement, Omnipotence, and Autonomy. For any missing items, a score of zero will be assigned (Appendix 2). The scores on all items (ranging from 1 to 7) are added to obtain the overall score. When no items are omitted, scores on the DAS go from 40 to 280. Lower scores represent more adaptive beliefs and fewer cognitive distortions. The DAS has good internal consistency, with alphas ranging from 0.84 to 0.92. The DAS is also reliable, with test-retest correlations over eight weeks of 0.80 to 0.84. The questionnaire has excellent concurrent validity, significantly correlating with several other measures of depression, including the Beck depression inventory (BDI). Also, Weissman & Beck, (1978) reported the CVR and CVI at 0.79 and 0.85, respectively. The DAS also significantly distinguishes between groups diagnosed as depressed or not depressed on the BDI. Toghyani (2014) reported CVR and CVI 0.78 and 0.86, respectively for the Persian version of DAS.
Procedure
After obtaining the necessary permissions for the research, the sample was divided into three groups, with each group comprising 15 adolescents. Before the research, participants provided written informed consent. The SPIN, the RRS, and the DAS (Falsafi & DashtBozorgi, 2019) were administered to all groups before the training sessions (pre-test). The CBT group received twelve 60-minute sessions, the ACT group received eight 60-minute sessions, and the control group was placed on a waiting list. All therapy sessions were conducted by a registered clinical psychologist with a PhD. After the treatment sessions, post-test assessments were conducted using the research instruments for both the intervention groups and the control group. Table 1 provides an overview of the treatment sessions. (Heimberg, 2002; Herbert et al., 2018) (Figure 1).
Data analysis
The study utilized descriptive and inferential statistics for data analysis. To examine the research hypothesis, an analysis of covariance (ANCOVA) was conducted using SPSS software,version 23. The significance level was set at 0.05. Before analysis, the data was checked to ensure that they met the basic assumptions of ANOVA. This included examining the normal distribution of scores and homogeneity of variance and covariance matrices (homoscedasticity) to confirm the assumption of a normal distribution of student engagement and academic resilience scores in the three study groups. Mauchly’s sphericity test was also used to check if the assumption of homoscedasticity was met. Levene’s and Box’s M tests were employed to validate the assumption of equivalence of covariances and student engagement and academic resilience variances. The results confirmed the homogeneity of variances, and Mauchly’s test verified the assumption of sphericity. Ultimately, the Box’s M test indicated the equivalence of covariances in the intervention and control groups, leading to the conclusion that the assumptions for conducting ANOVA were met.
Results
In the present study, there were 45 subjects in two experimental groups and one control group. Based on the demographic findings, the mean age in the CBT group was 15.99±3.16, in the ACT group it was 16.12±3.14, and in the control group, it was 16.16±3.19 with no significant difference between them (P=0.48). Also, 65% (n=29) of participants were female and 30% (n=16) were male. Moreover, 48% (n=21) of participants reported an average socioeconomic status (SES), 30% (n=14) of the participants announced a low SES, and 22% (n=10) declared a good SES.
Comparison of mean and standard deviation in research variables showed that the implementation of CBT in the first experimental group made significant differences between the pre-test and post-test in success-perfectionism (33.21±2.90, 28.76±3.48, P<0.001), need for others’ approval (28.30±2.80, 24.99±2.99, P<0.001), need to satisfy others (17.92±2.30, 14.68±2.71, P<0.001), vulnerability-function evaluation (18.88±3.72, 15.49±3.61, P<0.001), total score of the cognitive distortions (98.32±7.44, 83.90±7.77, P<0.001), and rumination (54.76±13.88, 49.51±13.42, P<0.001) (Table 2).
Also, the implementation of ACT on second experimental group made significant differences between pre-test and post-test in success-perfectionism (32.90±2.76, 29.77±3.40, P<0.001), need for others’ approval (28.44±3.04, 24.24±3.13, P<0.001), need to satisfy others (18.20±2.04, 15.26±2.18, P<0.001), vulnerability-function evaluation (18.91±3.68, 15.86±3.61, P<0.001), total score of the cognitive distortions (98.70±7.02, 85.13±6.83, P<0.001), and rumination (52.33±17.78, 47.73±14.23, P<0.001).
Moreover, there were no significant differences between the pre-test and post-test in the control group in success-perfectionism (33.21±2.57, 33.36±2.48, P>0.05), need for others’ approval (28.02±2.83, 27.84±3.13, P>0.05), need to satisfy others (17.51±2.65, 17.59±2.63, P=0.28), vulnerability-function evaluation (19.08±3.36, 18.89±3.59, P>0.05), total score of the cognitive distortions (97.83±6.98, 97.69±7.20, P>0.05), and rumination (54.75±13.65, 54.71±13.60, P>0.05) (Table 2). A pairwise comparison was used to determine the nature of the changes made, as reported in Table 3.
The results in Table 3 showed that in the post-test stage, there is no statistically significant difference between the groups of CBT and ACT; however, there is a statistically significant difference between these two experimental groups and the control group (P<0.001). There was no significant difference between the effectiveness of CBT and ACT in success-perfectionism (MD=-0.853, P>0.05), need for others’ approval (MD=0.890, P>0.05), need to satisfy others (MD=-0.323, P>0.05), vulnerability-function evaluation (MD=-0.654, P>0.05), the total score of the cognitive distortions (MD=-0.981, P>0.05), and rumination (MD=-0.601, P>0.05). Furthermore, there was a significant difference between CBT and control group in success-perfectionism (MD=4.860, P<0.001), need for others’ approval (MD=3.355, P<0.001), Need to satisfy others (MD=3.301, P<0.001), vulnerability-function evaluation (MD=3.361, P<0.001), total score of the cognitive distortions (MD=14.911, P<0.001) and rumination (MD=5.261, P<0.001). Moreover, there was a significant difference between ACT and the control group in success-perfectionism (MD=4.007, P<0.001), need for others’ approval (MD=4.244, P<0.001), need to satisfy others (MD=2.978, P<0.001), vulnerability-function evaluation (MD=2.707, P<0.001), total score of the cognitive distortions (MD=13.931, P<0.001) and rumination (MD=4.660, P<0.001).
Discussion
The current study compared the effectiveness of cognitive-behavioral and acceptance and commitment therapy on SAD symptoms, including cognitive distortions and rumination among adolescents with SAD. Although results showed that CBT and ACT treatments had a significant effect on the dependent variables, there is no significant difference between CBT and ACT treatments in influencing the mentioned dependent variables. In this regard, several studies (Rahmanian et al., 2020; Rezayi et al., 2017; Soltanizadeh et al., 2019) showed that CBT has a significant effect on social anxiety symptoms in adolescents with SAD. Herbert et al., (2018) showed that those who received CBT evidenced greater improvements in self-reported social anxiety symptoms and overall functioning. Also, some studies (Azar et al.; Esmaeili et al., 2018; Pourfarahani et al., 2020) showed that ACT has been effective on social anxiety and its components in adolescents.
Previous studies (Herbert et al., 2018; Zohdi et al., 2022) showed that there is no difference between CBT and ACT in the treatment of social anxiety. In a study conducted by Herbert et al., 2018, it was found that although the difference was not statistically significant, the ACT participants showed greater improvements in observer-rated social behavior in comparison to the CBT participants with a medium effect size. This disparity in the symptoms and behavioral outcomes, which is consistent with prior research, highlights the need for further investigation to examine the variations between CBT and ACT treatments regarding behavioral domains.
The present study found that cognitive distortions and rumination were significantly reduced in adolescents with SAD after undergoing CBT and ACT. CBT helps individuals with social anxiety by modifying cognitive distortions through restructuring, social skills training, and confronting their avoidance (Leigh & Clark, 2018). CBT can help those with social anxiety by altering their dysfunctional and distorted beliefs. Anxiety disorder patients commonly have 3 types of beliefs: Setting very high standards for themselves, conditional beliefs, and irrational beliefs about themselves. These beliefs lead to viewing the world as dangerous and avoiding social situations. Cognitive distortions in those with social anxiety disorder can significantly affect their interpretation of social situations and their solutions to social problems. These cognitive errors can lead to the growth and sustainability of their social anxiety. (Leigh & Clark, 2018).
CBT reduces cognitive distortions in SAD patients by preparing a hierarchical list of anxiety-causing situations, regular exercises to confront those situations, evaluating their cognitive distortions, and changing those maladaptive distorted thoughts into more adaptive ones (Leichsenring et al., 2013). Cognitive behavioral therapy is designed to engage and replace negative biases in information processing, negative self-evaluations of social functioning, and the need for other people’s affirmation. It also reduces pathological self-focused attention (Heimberg, 2002). Also, self-focused attention makes SAD individuals perceive their internal physical states, such as heartbeat, thoughts, and feelings, to have a direct representation outside. Therefore, this therapy prevents objective information processing in social situations and emphasizes facing social problems despite having feelings of anxiety by helping them understand its symptoms and encouraging them to increase their social function in social environments and reduce their avoidant lifestyles, protective behaviors, and distortions. Therefore, facing social situations acts as a behavioral test to prove or reject the cognitive hypotheses of people suffering from social anxiety, eventually leading to cognitive distortion modification (Heimberg, 2002).
On the other hand, ACT draws people’s attention to two fundamental aspects of their inner reality: 1) Trying to get close to people and pursuing life’s core values, and 2) Trying to get away from maladaptive thoughts and emotions. In other words, recognizing values and moving in the path of values promotes their psychological flexibility, and experiencing new committed behaviors that even can be against their will encourages them to move in a direction that continues to challenge their maladaptive beliefs and pulls them away from having those thoughts and emotions by gradual modification of them (Otte, 2022).
The fundamental belief in acceptance and commitment therapy for SAD individuals is that psychological distress is caused by experience avoidance, cognitive fusion, failure to meet behavioral needs, and incongruence with one’s core values (Khoramnia et al., 2020). Reducing symptoms is not the therapist’s goal but a byproduct of the treatment process. ACT changes the relationship between irrational thoughts and emotions so that the individual understands them as pathological symptoms and even learns to change them if they are uncomfortable and unpleasant. The general goal of ACT is to reduce the literal perception of the cognitive content that prevents behavior and to increase the probability of positive events by replacing correct cognitions (Sharp, 2012). Therefore, treatment based on acceptance and commitment can be used as one of the effective psychological treatments to reduce cognitive distortions by increasing a person’s psychological flexibility and connection with the present and encouraging him to move toward his values. The reason for the effect of treatment based on acceptance and commitment to cognitive distortions is that this approach targets the function of cognitions and emotions instead of changing the frequency or situational sensitivity. Changing the function of cognition and emotion seems more manageable than changing their form and content. The change in function is more objective than the change in the form and content of cognition and emotions, and the person has a sense of control over the function of cognition and emotions (Niles et al., 2014).
The results of the present study showed that cognitive behavioral therapy and acceptance and commitment-based therapy effectively reduce rumination in adolescents with SAD. In the explanation of the findings, rumination can be one of the characteristics of people with symptoms of anxiety disorders, and this issue continuously increases anxiety; On the other hand, CBT helps to change the content of mental rumination through the detection of cognitive errors, challenging them and conducting behavioral tests (Leichsenring et al., 2013). Also, CBT modifies the cognitive schemas that cause the continuation of negative emotions and strengthens negative beliefs in these individuals through organizing thought processes, emotional problems, and concerns associated with anxiety (avoidance, dependency, helplessness towards change, and rumination responses).
According to Ghasemi et al., (2023), psychological disorders can result from a lack of psychological flexibility, which is the central premise of ACT. ACT posits that individuals often view certain emotions and inner thoughts as distressing and attempt to eliminate or alter them. However, such efforts at emotional control are counterproductive, as they exacerbate the very emotions and thoughts that the individual is attempting to avoid. Consequently, the primary issue for patients in ACT is avoidance. The central process of ACT teaches people how to stop inhibiting thoughts, not to confuse them with disturbing thoughts, and makes them more tolerant of unpleasant emotions (Esmaeili et al., 2018). ACT therapy is based on pervasive awareness or mindfulness. In this method, mindfulness means consciously bringing awareness to the experience of the here and now with openness, interest, acceptance, and not being distracted by thoughts. During the research, Yabandeh et al. (2019) showed that conscious attention to the present moment and the ability to control attention effectively prevent rumination. In general, the main goal of the ACT approach is for the person to create a productive and meaningful life by achieving psychological flexibility and effectively controlling the pains, sufferings, and tensions that life has inevitably caused him, which will reduce rumination. People who are cognitively inflexible turn to rumination when upset and focus their energy and thoughts on rumination, which brings a repetitive and unhelpful response to the person (Yabandeh et al., 2019).
Conclusion
ACT is an effective treatment for anxiety and cognitive distortions. This therapy approach helps in developing psychological flexibility by combining mindfulness skills with self-acceptance, which makes it a form of behavioral therapy. ACT encourages people to open up to unpleasant feelings, learn to avoid overreacting, and not avoid situations that may trigger them. On the other hand, CBT targets the cognitive, behavioral, and physiological mechanisms. It helps in restructuring maladaptive thought patterns, correcting misinterpretations, changing attentional focus, and developing adaptive coping thoughts, which can lead to an increase in adaptive cognitions. Additionally, CBT can help in habituation, extinction of maladaptive responses, behavioral activation, associative learning, and reinforcement of adaptive responding for an increase in adaptive behavioral responses. Normalization of physiological arousal is also possible with CBT through habituation, incompatible response training, and changes in autonomic nervous system activity.
Limitations
Although the psychology centers initially offered their full and free cooperation, they later requested a fee to continue the research process during the intervention and our budget constraints posed challenges for us in this regard. Moreover, the parents of some adolescents disagreed with continuing to participate in the research.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the regional ethics committee (Code: IR.IAU.TABRIZ.REC.1401.239).
Funding
The paper was extracted from thePhD. thesis of Shirin Ebrahimi, Department of Psychology, Faculty of Human Science, Tabriz Branch, Islamic Azad University, Tabriz, East Azerbaijan, Iran.
Authors' contributions
All authors equally contributed to all parts of the study.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We would like to thank all the participants who participated in this study.
References
Aderka, I. M., McLean, C. P., Huppert, J. D., Davidson, J. R., & Foa, E. B. (2013). Fear, avoidance and physiological symptoms during cognitive-behavioral therapy for social anxiety disorder. Behaviour Research and Therapy, 51(7), 352–358.[DOI:10.1016/j.brat.2013.03.007] [PMID]
Arch, J. J., Eifert, G. H., Davies, C., Plumb Vilardaga, J. C., Rose, R. D., & Craske, M. G. (2012). Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders. Journal of Consulting and Clinical Psychology, 80(5), 750–765. [DOI:10.1037/a0028310] [PMID]
karimiazar, F., Saken Azari, R., Abdoltajedini, P., & Azmoudeh, M. (2022). [The effect of acceptance and commitment based therapy on the symptoms of social anxiety in shy girls adolescents (Persian)]. Nursing Psychiatric of Journal Iranian, 10(1), 46-54
Beck A. T. (1993). Cognitive therapy: Past, present, and future. Journal of Consulting and Clinical Psychology, 61(2), 194–198.[DOI:10.1037/0022-006X.61.2.194] [PMID]
Connor, K. M., Davidson, J. R., Churchill, L. E., Sherwood, A., Weisler, R. H., & Foa, E. (2000). Psychometric properties of the Social Phobia Inventory (SPIN): New self-rating scale. The British Journal of Psychiatry, 176(4), 379-386. [DOI:10.1192/bjp.176.4.379] [PMID]
Cuijpers, P., Auerbach, R. P., Benjet, C., Bruffaerts, R., Ebert, D., & Karyotaki, E., et al. (2019). The world health organization world mental health international college student initiative: an overview. International Journal of Methods in Psychiatric Research, 28(2), e1761. [DOI:10.1002/mpr.1761]
Esmaeili, L., Amiri, S., Reza Abedi, M., & Molavi, H. (2018). [The effect of acceptance and commitment therapy focused on self-compassion on social anxiety of adolescent girls (Persian)]. Clinical Psychology Studies, 8(30), 117-137. [Link]
Falsafi, A., & DashtBozorgi, Z. (2019). The effect of mindfulness training on rumination, body image, and sexual satisfaction in women with recurrent pregnancy loss (Persian)]. Iranian Journal of Rehabilitation Research, 5(3), 48-54. [Link]
Ghasemi, F., Emadian, S. O., & Hasanzadeh, R. (2023). Comparison of the effectiveness of mindfulness training and internet-based acceptance and commitment training on academic engagement, mental time travel, and students’ anxiety during the COVID-19 pandemic. International Journal of School Health, 10(2):82-91. [DOI:10.30476/intjsh.2023.97316.1267]
Heimberg R. G. (2002). Cognitive-behavioral therapy for social anxiety disorder: Current status and future directions. Biological Psychiatry, 51(1), 101–108. [DOI:10.1016/S0006-3223(01)01183-0] [PMID]
Herbert, J. D., Forman, E. M., Kaye, J. L., Gershkovich, M., Goetter, E., & Yuen, E. K., et al. (2018). Randomized controlled trial of acceptance and commitment therapy versus traditional cognitive behavior therapy for social anxiety disorder: Symptomatic and behavioral outcomes. Journal of Contextual Behavioral Science, 9, 88-96. [DOI:10.1016/j.jcbs.2018.07.008]
Hovenkamp-Hermelink, J. H. M., van der Veen, D. C., Oude Voshaar, R. C., Batelaan, N. M., Penninx, B. W. J. H., & Jeronimus, B. F., et al. (2019). Anxiety sensitivity, its stability and longitudinal association with severity of anxiety symptoms. Scientific Reports, 9(1), 4314. [DOI:10.1038/s41598-019-39931-7] [PMID]
Hyett, M. P., & McEvoy, P. M. (2018). Social anxiety disorder: Looking back and moving forward. Psychological Medicine, 48(12), 1937–1944. [DOI:10.1017/S0033291717003816] [PMID]
Jefferies, P., & Ungar, M. (2020). Social anxiety in young people: A prevalence study in seven countries. Plos One, 15(9), e0239133. [DOI:10.1371/journal.pone.0239133] [PMID]
Ruiz, F. J. (2012). Acceptance and commitment therapy versus traditional cognitive behavioral therapy: A systematic review and meta-analysis of current empirical evidence. International Journal of Psychology and Psychological Therapy, 12(2), 333-357. [Link]
Joyce-Beaulieu, D., & Sulkowski, M. L. (2015). Cognitive behavioral therapy in K-12 school settings: A practitioner’s toolkit. New York: Springer Publishing Company. [Link]
Karimpour-Vazifehkhorani, A., Bakhshipour Rudsari, A., Rezvanizadeh, A., Kehtary-Harzang, L., & Hasanzadeh, K. (2020). Behavioral activation therapy on reward seeking behaviors in depressed people: An experimental study. Journal of Caring Sciences, 9(4), 195–202. [DOI:10.34172/jcs.2020.030] [PMID]
Karimpour Vazifehkhorani, A., Bakhsipour Roodsari, A., Reyhanimehr, Q., Kamali Ghasemabadi, H., Noroozi, H., & Shadara, Z., et al. (2017). [Comparing brain behavioral systems in couples engaged in infidelity and normal couples in Tabriz, Tehran, and Karaj (Persian)]. Depiction of Health, 8(2), 97-103. [Link]
Karimpour Vazifehkhorani, A., Jafari, M. R., & Rahmati, F. (2023). The effectiveness of acceptance and commitment therapy training on health promoting lifestyle profile among soldiers. Iranian Journal of Health Education and Health Promotion, 10(4), 350-360. [DOI:10.52547/ijhehp.10.4.350]
Khoramnia, S., Bavafa, A., Jaberghaderi, N., Parvizifard, A., Foroughi, A., & Ahmadi, M., et al. (2020). The effectiveness of acceptance and commitment therapy for social anxiety disorder: A randomized clinical trial. Trends in Psychiatry and Psychotherapy, 42(1), 30–38. [DOI:10.1590/2237-6089-2019-0003] [PMID]
Kuru, E., Safak, Y., Özdemir, İ., Tulacı, R., Özdel, K., & Özkula, N., et al. (2018). Cognitive distortions in patients with social anxiety disorder: Comparison of a clinical group and healthy controls. The European Journal of Psychiatry, 32(2), 97-104. [DOI:10.1016/j.ejpsy.2017.08.004]
Leichsenring, F., Salzer, S., Beutel, M. E., Herpertz, S., Hiller, W., & Hoyer, J., et al. (2013). Psychodynamic therapy and cognitive-behavioral therapy in social anxiety disorder: A multicenter randomized controlled trial. The American Journal of Psychiatry, 170(7), 759–767. [DOI:10.1176/appi.ajp.2013.12081125] [PMID]
Leigh, E., & Clark, D. M. (2018). Understanding Social anxiety disorder in adolescents and improving treatment outcomes: Applying the cognitive model of clark and wells (1995). Clinical Child and Family Psychology Review, 21(3), 388–414. [DOI:10.1007/s10567-018-0258-5] [PMID]
Mallorquí-Bagué, N., Bulbena, A., Pailhez, G., Garfinkel, S. N., & Critchley, H. D. (2016). Mind-body interactions in anxiety and somatic symptoms. Harvard Review of Psychiatry, 24(1), 53–60. [DOI:10.1097/HRP.0000000000000085] [PMID]
Mohammadi, M. R., Salehi, M., Khaleghi, A., Hooshyari, Z., Mostafavi, S. A., & Ahmadi, N., et al. (2020). Social anxiety disorder among children and adolescents: A nationwide survey of prevalence, socio-demographic characteristics, risk factors and co-morbidities. Journal of Affective Disorders, 263, 450–457. [DOI:10.1016/j.jad.2019.12.015] [PMID]
Niles, A. N., Burklund, L. J., Arch, J. J., Lieberman, M. D., Saxbe, D., & Craske, M. G. (2014). Cognitive mediators of treatment for social anxiety disorder: Comparing acceptance and commitment therapy and cognitive-behavioral therapy. Behavior Therapy, 45(5), 664–677. [DOI:10.1016/j.beth.2014.04.006] [PMID]
Otte C. (2011). Cognitive behavioral therapy in anxiety disorders: Current state of the evidence. Dialogues in Clinical Neuroscience, 13(4), 413–421. [DOI:10.31887/DCNS.2011.13.4/cotte] [PMID] [PMCID]
Pourfarahani, M., Barabadi, H. A., & Heydarnia, A. (2020). [The effectiveness of acceptance and commitment group therapy in the social anxiety of adolescent orphan girls (Persian)]. Quarterly Journal of Social Work, 8, 5-13. [Link]
Rahmanian, Z., Mirzaian, B., & Hassanzadeh, R. (2020). [Effectiveness of cognitive-behavioral group therapy on social anxiety of female students (Persian)]. Daneshvar Medicine, 19(5), 47-56. [Link]
Rezayi, F., Amiri, M., & Taheri, E. (2017). [Effectiveness of cognitive-behavioral group therapy on reducing social anxiety and negative cognitive evaluation among hard of hearing young girls (Persian)]. Counseling Culture and Psychotherapy, 8(32), 133-160. [DOI:10.22054/qccpc.2018.23065.1565]
Sharp, K. (2012). A review of acceptance and commitment therapy with anxiety disorders. International Journal of Psychology and Psychological Therapy, 12(3), 359-372. [Link]
Smith, T. W., O'Keeffe, J. L., & Christensen, A. J. (1994). Cognitive distortion and depression in chronic pain: Association with diagnosed disorders. Journal of Consulting and Clinical Psychology, 62(1), 195–198. [DOI:10.1037/0022-006X.62.1.195] [PMID]
Soltanizadeh, M., Montazeri, M., & Latifi, Z. (2019). [Effectiveness of cognitive-behavioral therapy in social anxiety among children with type I diabetes mellitus (Persian)]. Journal of Health System Research, 15(3), 192-198. [DOI:10.32592/hsr.2020.15.3.102]
Stein D. J. (2015). Social anxiety disorder and the psychobiology of self-consciousness. Frontiers in Human Neuroscience, 9, 489. [DOI:10.3389/fnhum.2015.00489] [PMID]
Swain, J., Hancock, K., Hainsworth, C., & Bowman, J. (2013). Acceptance and commitment therapy in the treatment of anxiety: A systematic review. Clinical Psychology Review, 33(8), 965–978. [DOI:10.1016/j.cpr.2013.07.002] [PMID]
Takishima-Lacasa, J. Y., Higa-McMillan, C. K., Ebesutani, C., Smith, R. L., & Chorpita, B. F. (2014). Self-consciousness and social anxiety in youth: The revised self-consciousness scales for children. Psychological Assessment, 26(4), 1292–1306.[DOI:10.1037/a0037386] [PMID]
Tavoli, A., Allahyari, A., Azadfallah, P., Fathi Ashtiani, A., Melyani, M., & Sahragard, M. (2012). [Validity and reliability of the Farsi version of the social interaction anxiety scale (SIAS) (Persian)]. Iranian Journal of Psychiatry & Clinical Psychology, 18(3):227-232. [Link]
Toghyani, M. (2014). [The relationship of Islamic lifestyle with dysfunctional attitudes in university students (Persian)]. Knowledge & Research in Applied Psychology, 14(4), 35-43. [Link]
Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27, 247-259. [DOI:10.1023/A:1023910315561]
Weiner, C. L., Meredith Elkins, R., Pincus, D., & Comer, J. (2015). Anxiety sensitivity and sleep-related problems in anxious youth. Journal of Anxiety Disorders, 32, 66–72. [DOI:10.1016/j.janxdis.2015.03.009] [PMID]
Weissman, A. N., & Beck, A. T. (1978). Development and validation of the Dysfunctional Attitude Scale: A preliminary investigation. Paper presented at: the Annual Meeting of The American Educational Research Association, Torento, Canada, 1978. [Link]
Wong, S. S. (2008). The relations of cognitive triad, dysfunctional attitudes, automatic thoughts, and irrational beliefs with test anxiety. Current Psychology, 27, 177-191. [DOI:10.1007/s12144-008-9033-y]
Yabandeh, M. R., Bagholi, H., Sarvghad, S., & Kouroshnia, M. (2019). [Comparing the effectiveness of cognitive behavioral therapy with acceptance and commitment therapy on reduction of social anxiety disorder symptoms (Persian)]. Psychological Methods and Models, 10(36), 177-196. [Link]
Zohdi, Y., Mohammadkhani, P., & Karimpour-Vazifehkhorani, A. (2022). The role of Anhedonia and low arousal in substance use disorder among adolescents with conduct disorder symptoms. Practice in Clinical Psychology, 10(2), 111-120. [DOI:10.32598/jpcp.10.2.815.1]
Type of Study: Original Research Article |
Subject:
Cognitive behavioral
Received: 2023/07/19 | Accepted: 2023/09/13 | Published: 2024/01/1
Received: 2023/07/19 | Accepted: 2023/09/13 | Published: 2024/01/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
