

Volume 14, Issue 2 (Spring 2026)
PCP 2026, 14(2): 151-166 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mehrvarz F, Abolghasemi A, Khosrojavid M, Hosseinkhanzadeh A A. Comparing the Effectiveness of Parent-child Interaction Therapy, Cognitive-behavioural Therapy, and Their Combination in Adolescents With Problematic Sexual Behaviours. PCP 2026; 14 (2) :151-166
URL: http://jpcp.uswr.ac.ir/article-1-1052-en.html
URL: http://jpcp.uswr.ac.ir/article-1-1052-en.html



1- Faculty of Literature and Humanities, University of Guilan, Rasht, Iran.
2- Faculty of Literature and Humanities, University of Guilan, Rasht, Iran. ,abolghasemi1344@guilan.ac.ir
2- Faculty of Literature and Humanities, University of Guilan, Rasht, Iran. ,
Keywords: Parent-child interaction therapy (PCIT), Cognitive-behavioural therapy (CBT), Depression, Family function, Parenting stress, Problematic sexual behaviour (PSBs)
Full-Text [PDF 814 kb]
(99 Downloads)
| Abstract (HTML) (836 Views)
Full-Text: (101 Views)
Introduction
Aolescence is widely acknowledged as a critical phase marked by significant changes in physical, cognitive, and socioemotional domains, the effects of which often extend into adulthood (Cheng et al., 2024). One of the crucial aspects of growth in adolescence is sexual growth (Hackett et al., 2013). Problematic sexual behaviour (PSB) consists of a sexual part of the body (genitals, breasts) includes, interference with a person’s growth, using coercion, intimidation, or force, physical injuries, continuing and addictive behaviours, and sexual activity (Mori et al., 2023; Pistre et al., 2023; Hacket et al., 2013). According to Davis et al. (2003), the development of PSBs can be influenced by four categories of factors in individuals: child and adolescent vulnerabilities, including developmental problems; family adversities, such as lack of guidance and supervision, stress, parental depression, and substance use; sexual modelling; and coercive modelling. A developmental period of the greatest risk for PSBs exposure is late childhood and early adolescence (ages 10–14) (Finkelhor et al., 2009; Pistre et al., 2023). Overall, almost 47% of adolescents worldwide have experienced sexual behaviours, and 6% of them experienced the first sex before age 13 (Delago et al., 2020). In Iran, the prevalence of sexual relationships among teenage boys and girls has been reported to range from 12.8% to 20%(Alimoradi et al., 2017).
One of these adolescent vulnerabilities for PSB can be depression. According to Aaron Beck’s theory (1976), which is also applicable to children and adolescents (Beck & Alford, 2009), depression results from automatic negative thoughts, dysfunctional schemas, and cognitive distortions, including a negative outlook toward oneself, the world, and what lies ahead. Studies have shown that adolescent sexual experiences and behaviours are associated with depression (Boyd et al., 2022), and this relationship is stronger in younger adolescents (Savioja et al., 2015). Sexual behaviours are a breakthrough attempt to regulate emotions, and depression among PSBs means overcoming negative emotions (Craparo, 2014), and is related to the way parents respond to these emotions (Whalen, 2020).
As mentioned, besides adolescent vulnerabilities, family adversities have a major role in children’s problems. The McMaster model considers six aspects of family functioning: Problem solving, communication, roles, emotional response, emotional involvement, behaviour control (Epstein, 1993). Studies have shown that the functioning of the family directly and indirectly predicts the behavioural problems of children (Song et al.,2023; Du et al., 2020, Abbass ghorbani & Naghdi, 2020; Mirzaaghasi et al., 2019; Wang et al., 2021), and parental depression plays a moderate role (Du et al., 2020). Another crucial family adversity is parental stress. According to Abidin’s (2016) model, there are three areas for parental stress: parent, child, and parent-child relationship (Deckard, 2020). The results of the studies show parents’ stress is a positive predictor of children’s behavioural problems (Thériault et al., 2025; Cook et al., 2024; Khoshkerdar et al., 2020) and parental depression plays a moderate role in the relation of family functioning and behavioural problems of children (Du et al., 2020). Additionally, parenting stress is a barrier for families who receive intervention for PSBs (Shields et al., 2018)
Adolescents with PSBs achieve the desired result by treatments (Grady et al., 2023), such as PCIT and CBT (Shawler, et al. 2018, Jenkins et al., 2020). PCIT, which addresses behavioural issues by focusing on both adolescents and their caregivers (Bonner et al., 2017), pursues goals, such as strengthening parent-child relationships, while decreasing behavioural issues; parental skills, including positive discipline, reducing parental stress and shame (O’Toole et al., 2021; Warren et al., 2022; Hashemi & Eyni ,2020) and depression (Fatemi et al., 2022; Wessing et al., 2015), improving family functioning (Sharifi & Sepehvand ,2023). Additionally, parents’ parenting styles are related to family functioning (Abbass ghorbani & Naghdi, 2020) and parent-child relationships marked by minimal conflict strengthen the connection between mindful parenting and maternal depression (He et al.,2025). CBT treatment is a family-based, psychological and supportive group treatment consisting of behavioural and cognitive discipline (Silovsky et al., 2018), has strong empirical evidence to reduce internal and external behaviour problems (Hacket et al., 2013; Jenkins et al., 2020; Silovsky et al., 2018) characteristic clinical features of depression (Lisoy et al., 2024; Murray et al., 2015; Samavatyan et al., 2021) and decrease in parental stress (Gusler et al., 2023).
According to the background of the research, PSBs can be an obstacle to the normal transformation of late childhood and early adolescence (ages 10–13) and can damage them or their families; and according to the high prevalence and early onset, the researchers believe this study can contribute to early identification and intervention of PSBs. Moreover, to date, most research have only reviewed proposed therapies for PSB and the effectiveness of them or their combinations—even internationally—has been examined in only a few studies, which primarily focused on PSBs itself, rather than its underlying factors. Also, personal vulnerabilities and family adversities, which are identified in this study, have not been examined in other studies yet. To address this gap, the aim of the present study is to compare
Materials and Methods
This study is a quasi-experimental study with a pre-test-post-test design with three experimental groups and without a control group. The statistical population of the present study consisted of all primary school students with PSBs in Guilan Province, Iran, during the 2023-2024 academic year. The sample of the study included 35 female primary school students aged 10-13 years with PSBs, who were identified through purposive sampling based on the cut-off point in the PSBs Questionnaire and through semi-structured clinical interviews based on the diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) (McKibbin et al., 2017). To comply with ethical guidelines, the present study was conducted exclusively with female participants. Considering the presence of three experimental groups and two time points (pre-test and post-test), the sample size and assignment of participants to each group were determined using Cohen’s sample-size tables based on the F-ratio (Cohen, 1988). The degrees of freedom for the table were calculated using the Equation 1:
1. Degrees of freedom (u)=(r−1)×(c−1)=(3−1)×(2−1)=2
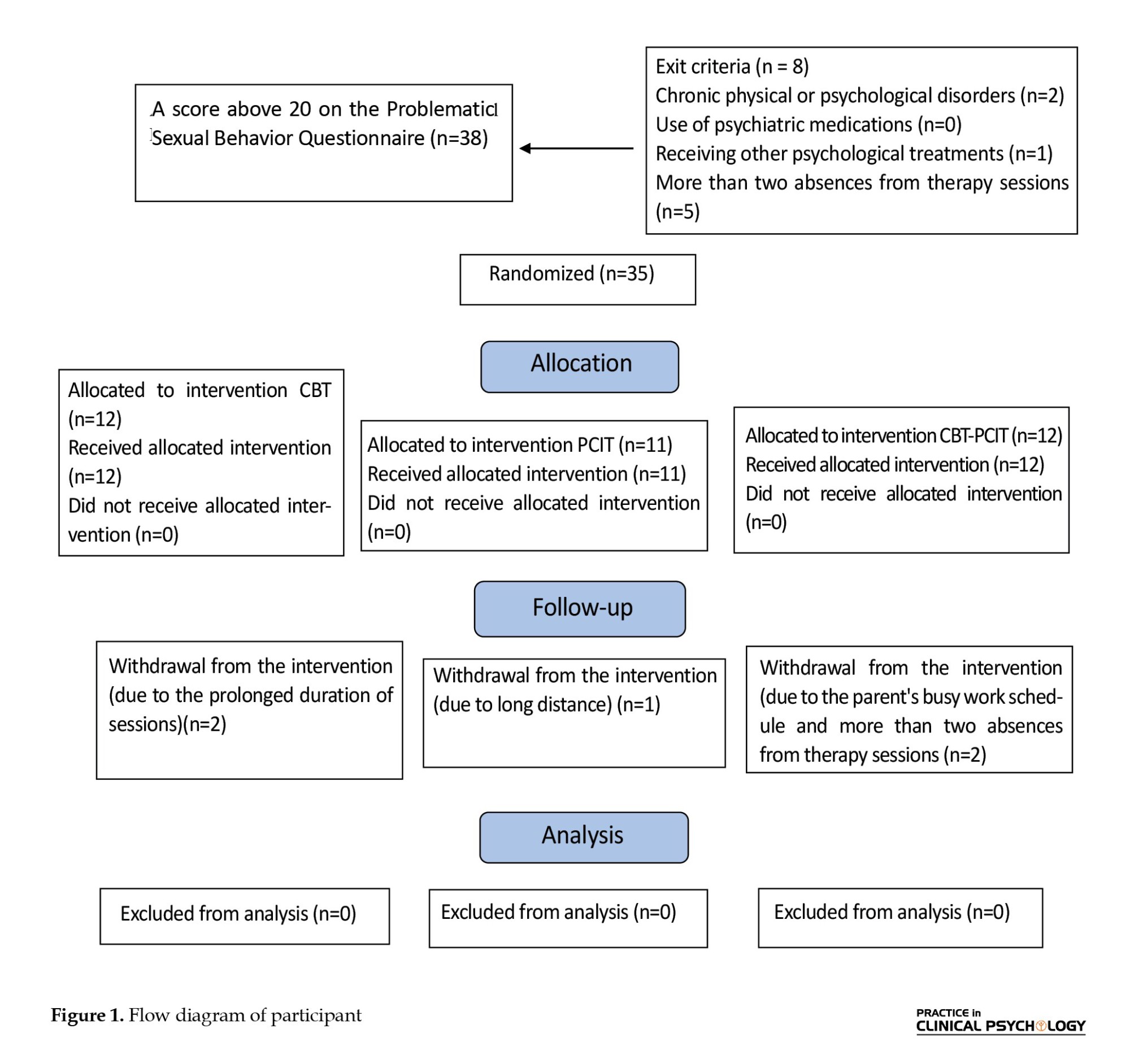
The minimum sample size for degrees of freedom equal to 2, considering a confidence level of 95%, test power of 80%, and an effect size of 0.50, was determined to be 10 participants per group. In this study, accounting for possible attrition of participants, 12 individuals were selected for two groups and 11 individuals for one group, and were randomly assigned to the groups. Randomization was performed using a table of random numbers to ensure unbiased and fully random allocation of participants to the study groups.
Top of Figure 1, the inclusion criteria included age (10 to 13 years), gender (female), tendency to participate and collaborate in the research. The exclusion criteria included physical and psychological diseases (direct question), consumption of psychiatric drugs (direct question), receiving other psychological therapies (direct question), and more than two absences from therapy sessions, and a very high score in the PSB questionnaire.
Study instruments
Clinical Interview: Semi-structured interviews of six provided treatments (McKibbin et al., 2017) and the clinical interview based on the DSM-5 were used.
Child and Adolescent Sexual Behaviour Checklist: The Child and Adolescent Sexual Behaviour Checklist (Friedrich, 1998) for children aged 2-12 years includes 37 items and 9 main content areas: boundary issues, gender role behaviour, sexual interest, sexual knowledge, nudism, self-stimulation, sexual influence, behavioural attitude, and sexual anxiety, rated on a 5-level Likert scale. The main caregiver ranked the behaviours they observed during the past six months on a four-point scale from 0 (never) to 4 (at least once a week). Cronbach’s α on the normal sexual behaviour scale in children was equal to 0.77, and Cronbach’s α for each component was between 0.75 and 0.78 (Kareshki et al., 2019). The Cronbach’s α of this scale in this research was 0.77. In this study, it was also administered to participants aged 13, given the minimal developmental differences at this age.
Maria Kovacs children’s depression questionnaire: The Child Depression Questionnaire is a self-reported scale designed by Kovacs (1992) for children and adolescents aged 7-17 years and includes 27 items and 3 main content areas: behavioural, cognitive, and emotional symptoms of depression, based on the Likert scale from 0 to 2 (for A to C). The reliability coefficients for the two inventories—the Maria Kovacs and Beck questionnaires—were reported as 0.789 and 0.526, respectively. Furthermore, when comparing the Maria Kovacs inventory to the Beck inventory (used as the criterion test), it was found that a non-depression score range of 0–8 on the Kovacs inventory corresponded to a sensitivity of 97.2%, specificity of 46.1%, and positive and negative predictive values of 85.7% (Mirzaie et al., 2019). The Cronbach’s α of this scale in this research was 0.78.
Family functioning questionnaire: The family functioning questionnaire was designed by Epstein et al (1983) based on McMaster’s pattern, and includes 60 items and 7 main content areas: problem solving, communication, roles, emotional companionship, emotional intercourse, behaviour control of family functioning, and overall function of the family, which are rated on a 4-level Likert ranging from 1 to 4 “strongly agree,” “agree», “disagree,” and “strongly disagree”. A high score means unhealthy functioning. This tool has a good internal consistency from 0.72 to 0.92 with its subscales from 0.72 to 0.92. Cronbach’s α was calculated for 60 items and 7 subscales as 0.83 and 0.82, respectively. Its total reliability was 0.79 (Eimani & Shiralinia, 2015). The Cronbach’s α of this scale in this research was 0.72.
Parenting stress scale: The parenting stress scale was designed by Berry and Jones (1995) and includes 18 items that are rated on a 5-level Likert scale from 1 to 5, “completely agree,” “agree”, “no opinion “,”disagree,” and “completely disagree”. The items relate to the positive aspects of parental tasks, as well as their negative aspects. Berry and Jones have examined the reliability of the tool in the test-re-test method and reported this scale to be 80%. In a preliminary study conducted to assess the validity of the scale translated into Persian, the test-re-test reliability was reported as 0.78 (Paghandeh, 2019). Additionally, the reliability of the instrument was reported by Mohtashami et al. (2012) using Cronbach’s α, yielding a value of 0.73. The Cronbach’s α of this scale in this research was 0.71.
Parent-child interaction therapy (PCIT) for Problematic sexual behaviours (PSBs): The PCIT is a family-based approach designed to address behavioural issues, focusing on two key skill categories: Child-related skills and caregiver-related skills. In this therapy, mothers can effectively take on the role of a therapist for their children (Bonner et al., 2017). The PCIT treatment specifically designed for PSBs was introduced by Allen et al. (2016). For the purposes of this research, PCIT was implemented by rigorously applying the principles and techniques of this therapy over 18 weekly 1-hour sessions, lasting 4 to 5 months, and exactly based on the treatment protocol. During these sessions, two general types of interactions (child-directed interaction [CDI] and parent-directed interaction [PDI]) were developed within families. The treatment included clinical assessment and treatment planning along with psychoeducation for 2 sessions, CDI training for 5 sessions, PDI training for 7 sessions, and completion of the treatment plan over 4 sessions (Appendix 1).
Cognitive-behavioural therapy (CBT) for PSBs: The CBT for PSBs is a family-based, psychoeducational, and supportive group therapy aimed at reducing or eliminating incidents of such behaviours. The CBT treatment specifically designed for PSBs was introduced by Silovsky et al. (2013). Like PCIT, this approach was also implemented over 18 weekly 1-hour sessions, taking place over 4 to 5 months. The key clinical components for the child and caregiver include rules regarding sexual behaviour and boundaries, abuse prevention skills and safety planning, emotional regulation and coping skills, impulse control and problem-solving skills for children, developmentally appropriate sexual education, social skills and peer relationships, and acknowledgment of sexual behaviour, apology, and restitution. Additional key clinical components for caregivers include behavioural parent training for the prevention of and response to PSB and other behavioural issues; promoting the child’s overall development with an emphasis on psychological and emotional changes; correcting misconceptions about PSB and their consequences for the child; communicating effectively with children about sexual behaviour and development; and supporting children’s use of coping and decision-making skills (Silovsky et al., 2018) (Appendix 2).
Combination of Parent-Child Interaction and (CBT): This research utilized a combined approach based on common factors, emphasizing the shared elements of the two therapies over their unique components, thus leading to more effective treatment outcomes (Norcross & Goldfried, 2005). The combined therapy integrated key aspects of both PCIT and CBT, including clinical assessment, treatment planning, and introduction to treatment over 2 sessions, psychoeducation over 4 sessions, CDI training over 4 sessions, and PDI training along with sexual knowledge over 4 sessions. Additionally, the stage of sexual education, understanding, and prevention of sexual abuse was conducted over 2 sessions, followed by completion of the treatment plan over 2 sessions. The formal validity of the treatment package was evaluated and confirmed by supervisors and advisors based on criteria, such as alignment of components with treatment goals, comprehensiveness, and content coherence. The evaluation indicated that the selected components from the two therapeutic approaches have conceptual overlap and are complementary, making their integration scientifically and practically justified.
Furthermore, the integrated treatment package was pilot-tested with five previous clients of the center. Based on their feedback, the content of the intervention was considered satisfactory in terms of coherence, clarity of concepts, and alignment with treatment needs, and minor adjustments were made to the delivery of the sessions. This combined approach was carried out over 18 weekly sessions, spanning 4-5 months.
Participants and procedure
This study was conducted after obtaining the necessary approvals from the Faculty of Literature and Humanities at the University of Guilan. The researcher subsequently approached the Counseling Center of District 1, Rasht City, Iran, and, with the support of academic supervisors, obtained permission to conduct the study. Parents of female elementary school students were informed about the study through school principals and counselors, using both in-person meetings and virtual communication via the Shad platform. They were invited to participate if they were interested in receiving training related to their children’s sexual development. To enhance parental engagement, the researcher emphasized the high prevalence of problematic sexual behaviors, the importance of early adolescence education in preventing future sexual disorders, the ethical and cultural considerations of the study, and the confidentiality of participants’ information. Parents were also instructed to attend the initial assessment and interviews without their children to ensure ethical standards.
A total of 63 interested parents visited the counseling center and voluntarily completed the Problematic Sexual Behavior Questionnaire regarding their child. Subsequently, the researcher conducted semi-structured clinical interviews with the parents based on the DSM-5 criteria (McKibbin et al., 2017). Based on the questionnaire and interview results, 38 students who scored above 20 on the problematic sexual behavior questionnaire and exhibited early-stage problematic sexual behaviors (e.g. touching, voyeurism, weak boundaries, and interest in the opposite sex) were identified.
After applying inclusion and exclusion criteria, 35 students meeting all criteria were selected as adolescents with problematic sexual behaviors. Their parents were invited to participate in the interventions, and the adolescents were randomly assigned to three treatment groups using a random number table. After completing the questionnaires related to the study variables, treatment sessions were implemented. During treatment, five individuals were excluded from the research due to absence of more than two sessions.
In this study, 18 PSB-CBT and PCIT treatment sessions were held within 4-5 months. These sessions were conducted by the researcher and at the Centre of Psychological Services and included individual and combined sessions of children and parents. To minimize interaction between the groups, separate time slots were allocated for each group’s attendance at the center. Participants were instructed not to disclose or discuss the type of treatment they were receiving with others. Although all sessions were delivered by a single therapist, the use of a detailed standardized treatment manual helped minimize therapist-related biases. To maintain participants’ motivation and minimize dropouts, a respectful and supportive relationship was established between the researcher and participants. Session schedules were adjusted based on participants’ availability, with reminders sent one day prior via the Shad messaging platform. Missed sessions were supplemented with audio summaries sent to parents and children, and key concepts from previous sessions were briefly reviewed at the start of each session. Finally, after completing complete treatment sessions, the post-test was administered, and data were analysed using SPSS software, version 27.
Results
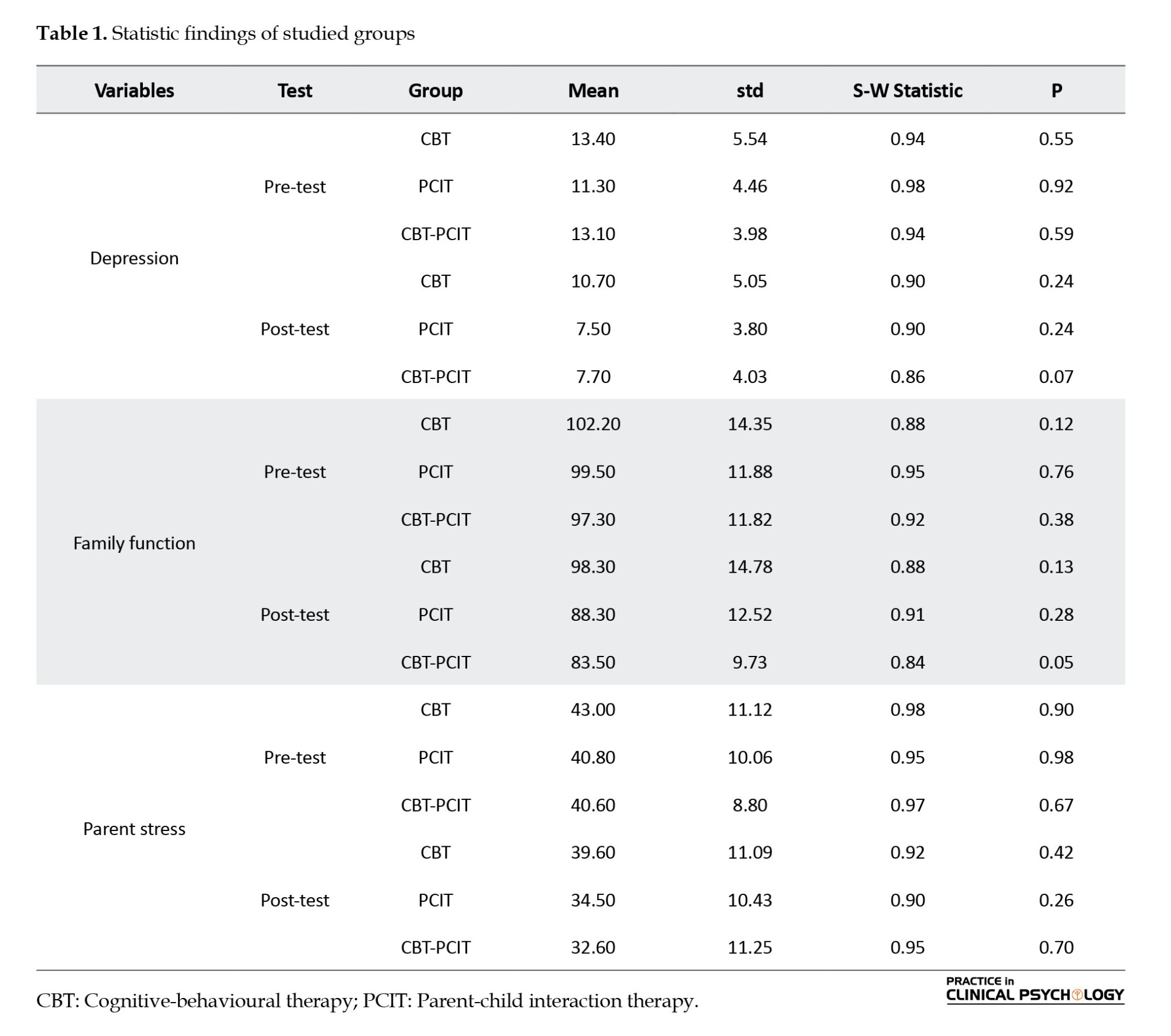
In the descriptive statistics section, results obtained from the one-way analysis of variance (ANOVA) indicated no significant difference in the mean age of students (P>0.05, F=0.7) and no significant difference in the mean age of mothers across the experimental groups (P>0.05, F=1.11). Also, the results of the chi-square test showed no significant difference in the frequency of participants across the experimental groups in birth order (P>0.05, χ²(3)=0.95), mothers’ education (P>0.05, χ²(3)=2.40), and family economic status (P>0.05, χ²(3)=1.25). Table 1 presents the means and standard deviations of the research variables in the test groups and in the pre-test and post-test. To check the normality of the variables, the Shapiro-Wilk test was employed, and the results revealed that the assumption of normality of all the variables in the pre-test and post-test was met and the distribution of all the variables was normal (P>0.05).
To examine the assumption of homogeneity of regression slopes for the pre-test and post-test scores across experimental groups, an F-test was conducted. The results of this test for depression variable were (F=0.83, P=0.49) and family function were (F=0.53, P=0.49). Neither variable was significant (P>0.05). The results indicated no significant interaction between the treatments and the pre-test scores, suggesting that the assumption of homogeneity of regression slopes was met and that performing analysis of covariance (ANCOVA) was appropriate. However, for the parental stress variable (F=66.61, P=0.001), the results showed a significant interaction between the treatments and the pre-test scores (P<0.05), indicating that the assumption of homogeneity of regression slopes was violated. Therefore, we must use the one-way ANOVA instead. To determine the homogeneity of the test groups in the post-test, Levene’s test was used to compare group variances. The results for the depression variable were (F=3.325, df=2, P=0.05) and for the family functioning variable were (F=1.337, df=2, P=0.28). Both variables were not significant (P>0.05). It can be said that the variances are equal in experimental groups; therefore, further analysis of this variable was not performed.
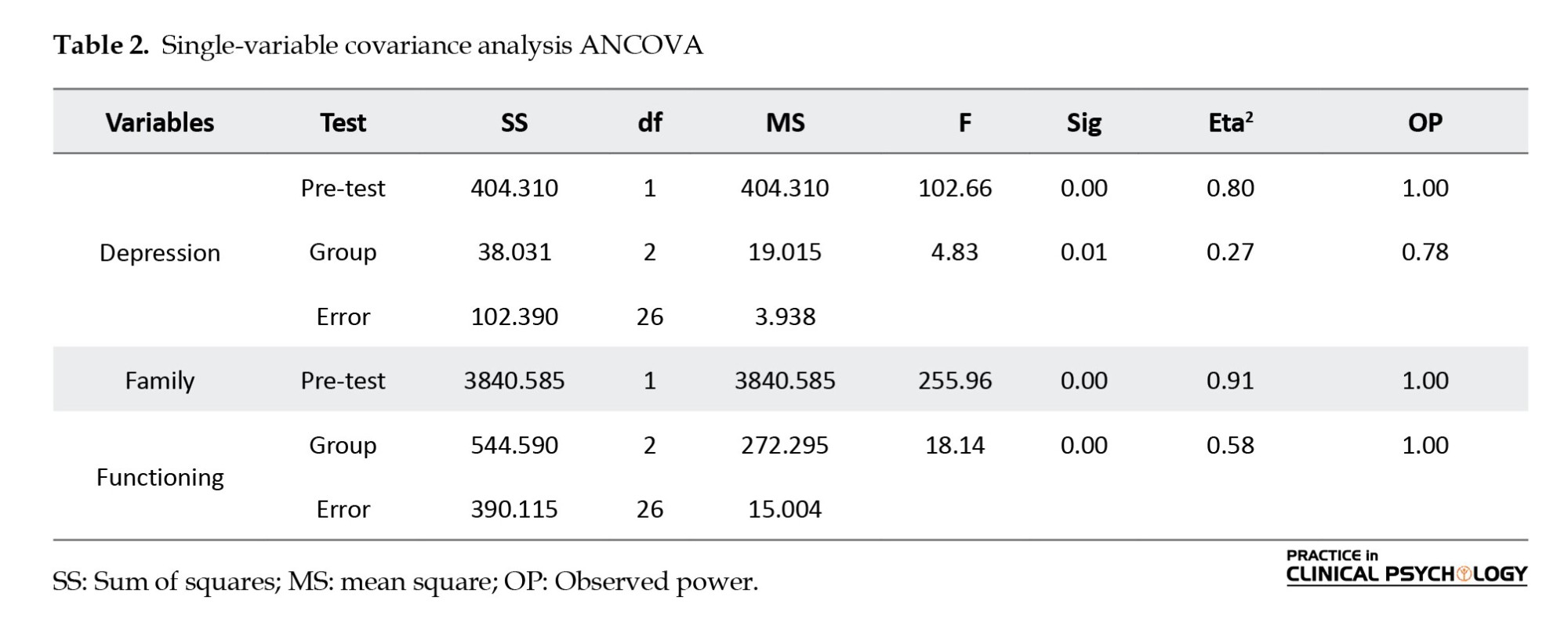
The results of ANCOVA have been reported to determine post-test differences between the test groups, by controlling the pre-test effect, as presented in Table 2. Results for depression were (F=4.83, df=2, P=0.01, observed power [OP]=0.78). This table shows a significant difference between the experimental groups for the depression variable (P≤0.05). The eta squared (η²) indicates that 27% of the variance in depression can be explained by the experimental conditions. In addition, the results for family functioning were (F=18.14, df=2, P=0.00, OP=1.00). This table shows a significant difference between the experimental groups in the family functioning variable (P≤0.05). The eta squared (η²) indicates that 58% of the variance in family functioning can be explained by the experimental conditions.
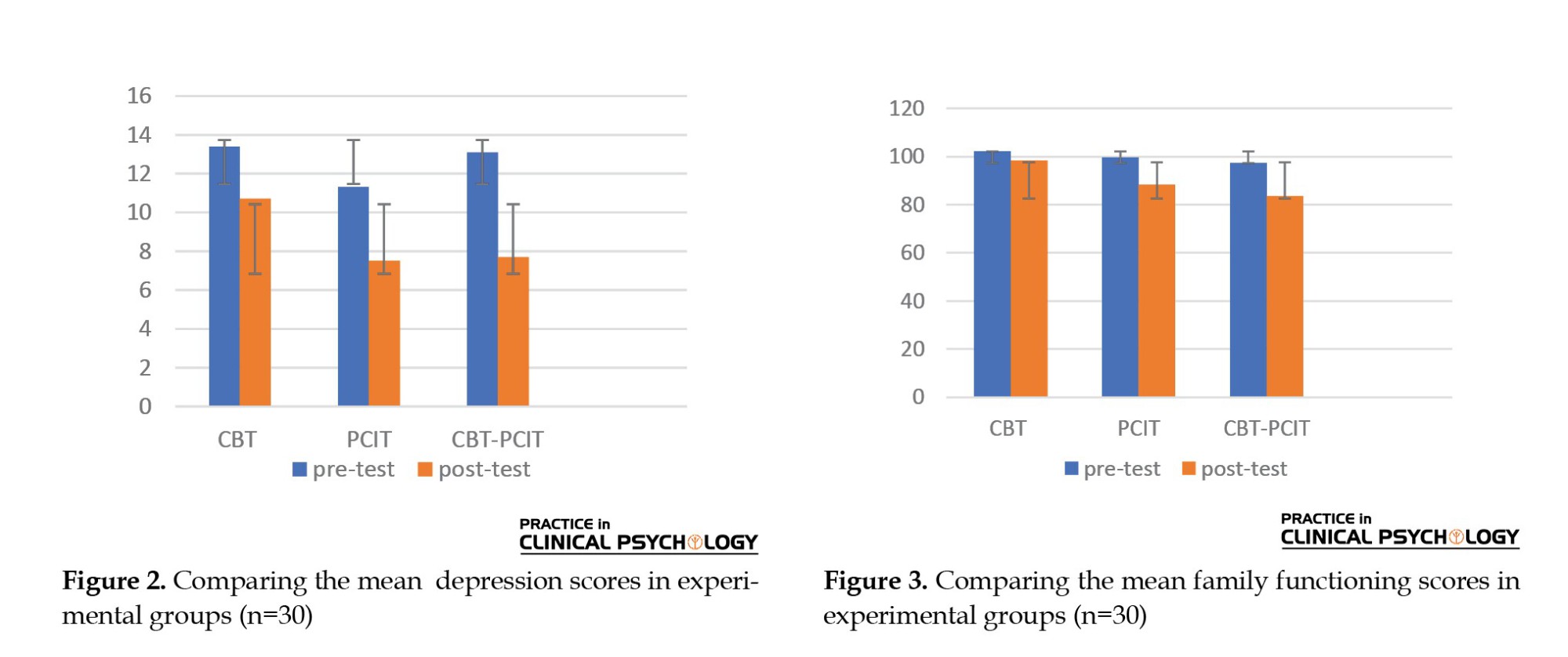
To examine which experimental groups showed differences in depression scores, a Bonferroni test with a 95% confidence interval was conducted. The results indicate that a significant difference was found in depression scores only between the CBT group and the PCIT-CBT group (P≤0.05). The comparison between the CBT and PCIT groups revealed no significant difference, nor was a significant difference found between the PCIT and CBT-PCIT groups (P>0.05). According to the mean scores of the experimental groups in Figure 2, the depression score of the CBT group is 10.05, the score of PCIT group is 8.55, and the score of CBT-PCIT group is 7.29. The depression scores of participants in the CBT-PCIT group are lower than those of participants in the CBT group. Based on this finding, it can be inferred that the combined therapy is more effective than CBT in reducing depression.
To examine which experimental groups showed differences in family functioning scores, a Bonferroni test with a 95% confidence interval was conducted, and the results indicated that a significant difference is observed between the CBT group and the PCIT group, as well as between the CBT group and the PCIT-CBT group (P<0.001). However, no significant difference was found between the PCIT and CBT-PCIT groups (P>0.05). The mean family functioning score shown in Figure 3 were as follows: 95.93 for the CBT group, 88.46 for the PCIT group, and 85.71 for the PCITCBT group. The results showed that the adjusted mean of family functioning scores of participants in the PCIT and CBT-PCIT groups were lower than those of participants in the CBT group. Since a lower score in family functioning indicates a more favourable outcome, it can be concluded that PCIT and CBT-PCIT are more effective than CBT in improving family functioning.
For the parental stress variable, due to the lack of assumptions of the regression slope required for ANCOVA, we could not use ANCOVA; therefore, we used one-way ANOVA instead. To determine the homogeneity of the experimental groups, Levene’s test was used to compare group variances. The results for the parents’ stress variable were (F=0.440, df=2, P=0.65) and were not significant (P>0.05), indicating that the variance of this variable was equal in experimental groups; therefore, further analysis of this variable was not performed.
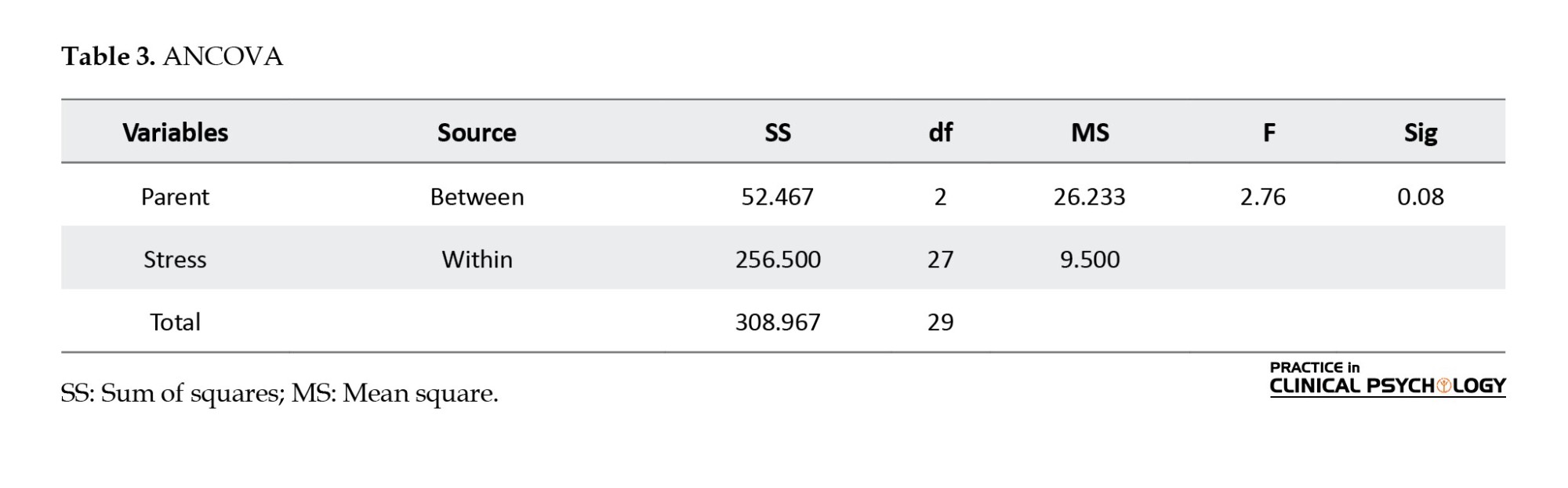
In Table 3, the results of the one-way ANOVA showed no significant differences among the experimental groups (F=2.76, df=2, P=0.08). The results showed no significant difference among experimental groups in the parental stress variable (P>0.05).
Discussion
This study aimed to compare the effectiveness of PCIT, CBT, and their combination on depression, family functioning, and parenting stress among adolescents with PSB. The findings of the present study revealed a significant difference between the experimental groups in the depression variable and 27% of the variance was explained by the experimental conditions of this research. Furthermore, CBT-PCIT was more effective than CBT in reducing depression. The results of this study were consistent with previous research that has shown a relationship between childhood sexual behaviours and depression (Savioja et al., 2015) and that PCIT and CBT lead to changes in depressive cognitions and a reduction in clinical symptoms of depression (Lisoy et al., 2024; Murray et al., 2015; Wessing et al., 2015; Samavatian et al., 2021; Fatemi et al., 2022). This convergence may stem from the shared emphasis on cognitive restructuring, enhanced emotional regulation mechanisms, and parenting skills.
These findings extend prior evidence by demonstrating that combining CBT with parent–child interaction components can yield broader and more sustainable outcomes, particularly in contexts where relational stressors play a central role in depressive symptomatology.
As mentioned earlier, depression results from automatic negative thoughts, dysfunctional schemas, and cognitive distortions. In this study, the combined therapy involved teaching parent-child relationship skills, which included behaviour management and communication, reducing stigma and shame, addressing myths and misconceptions, fostering hope, recognizing and expressing emotions, self-control skills, and emotional regulation, as well as family reunification. Alongside these, cognitive-behavioural skills were taught, including self-control and self-soothing strategies, using behavioural techniques to stop unhealthy thoughts or actions, cognitive restructuring, identifying erroneous beliefs, challenging thoughts, teaching social skills, applying self-control to sexual behaviour rules, enhancing self-control cues, creating and maintaining friendships, peer pressure management, preventing abuse, empathy, and apologizing. These interventions collectively contributed to the improvement of depression in these adolescents.
Regarding differences between these two approaches, CBT primarily targets intrapersonal factors of depression by modifying dysfunctional cognitions, maladaptive beliefs, and avoidance behaviours. Its mechanisms of change are largely cognitive and behavioural, aiming to restructure thought patterns and promote adaptive actions. In contrast, PCIT focuses on interpersonal and emotional dimensions by enhancing the quality of parent-child interactions, strengthening attachment security, and improving emotion regulation through responsive and supportive relationships. The therapist guides parents to become emotionally attuned and behaviorally consistent, which creates a more nurturing family environment. Thus, while CBT operates mainly through cognitive restructuring and behavioural activation, PCIT facilitates emotional regulation and relational repair through experiential learning within the parent–child dyad. Integrating these two approaches addresses both the internal cognitive processes and the external relational context that contribute to depressive symptomatology. The presence of the parent as an active agent of change extends the therapeutic process beyond the clinical setting, allowing newly acquired emotional and behavioural skills to be practiced and reinforced in daily interactions. This generalization of therapeutic gains may explain the greater durability and magnitude of symptom reduction observed in the integrated treatment. Overall, by simultaneously targeting cognitive distortions, emotional dysregulation, and relational insecurity, the combined CBT–PCIT model provides a more comprehensive and ecologically valid framework for treating depression. This integrative approach leverages complementary mechanisms of change—cognitive insight and emotional connection—to foster deeper and more sustainable therapeutic outcomes than CBT alone.
Moreover, the findings of the present study indicated a significant difference between the experimental groups in family functioning and 58% of the variance was explained by the experimental conditions of this research. PCIT and CBT-PCIT were more effective than CBT in improving family functioning. These results align with those reported in earlier studies showing that adolescents’ behavioural problems are related to family functions and behavioural and family based education can improve family functioning (Song et al.,2023; Du et al., 2020; Ghorbani & Naghdi, 2020; Mirzaaghasi et al., 2019; Wang et al., 2021; Sharifi & Sepehvand , 2023; Silovsky, 2020). It may be explained by the fact that PCIT directly targets patterns of interaction, communication, and emotional responsiveness within the family system, domains that are only indirectly addressed in traditional CBT. Moreover, the inclusion of parents as active participants likely facilitated the generalization of therapeutic gains to the home environment. These findings extend prior evidence by demonstrating that interventions combining cognitive restructuring with relational and systemic components can yield broader improvements in family functioning, beyond symptom reduction alone.
We also found that the effect size for the depression variable was 0.27, while that for the family functioning variable was 0.85. This shows that the family functioning was affected by experimental conditions more than the depression variable. This can be explained by the fact that, first, PCIT directly targets parent–child interactions, which are the core components of family functioning, whereas subclinical depressive symptoms are internal and may be less responsive to interaction-focused strategies. Second, observable behavioural changes can occur relatively quickly, while changes in mood and cognition often require longer periods and more intensive cognitive work.
As mentioned, PCIT can lead to improvements in parenting skills and positive discipline, enjoyment of shared time, parental control over standards, direct targeting of dysfunctional behaviours, and family reunification in two stages, thereby improving family functioning. Since caregivers in this therapy learn a systematic approach to discipline and practice behavioural management and communication skills, they can influence family functioning aspects, such as problem-solving, communication, roles, emotional responsiveness, emotional involvement, and behaviour control. Additionally, the combined treatment, with its focus on emotional regulation and coping skills, impulse control and problem-solving for children, developmentally appropriate sexual education, social skills, peer relationships, and affirmation of sexual behaviours, as well as behavioural techniques to stop unhealthy thoughts or actions, cognitive restructuring, identifying misconceptions, apologizing, and compensating, alongside family components, can lead to the improvement of family functioning.
Additionally, the results showed no significant difference between the experimental groups in the parental stress variable. Previous studies have shown that parents’ stress is associated with children’s behaviour and parent-child relationship (He et al., 2025; Cook et al., 2024; Hashemi & Eyni, 2020, Khoshkardar et al., 2020) and CBT can lead to a decrease in parental stress (Gusler, 2023) and PCIT is effective in reducing parental stress (Warren et al., 2022). Previous studies did not compare the effectiveness of these kinds of therapies on parent stress. Therefore, the findings from this study on parental stress are not consistent with previous studies. Several factors may explain this finding. First, parental stress was not necessarily severe at baseline, limiting the potential for measurable reductions. Second, while the interventions targeted child behaviour and parent–child interactions, they did not directly focus on stress management or coping strategies for parents. Third, changes in parental stress may require longer or more intensive interventions, as short-term programs are more likely to produce observable improvements in family functioning or child behaviour.
The parent-child-relationship model (Abidin, 2016) presents three domains for parental stress: the parent, the child, and the parent-child relationship. Research in this area shows that parental stress acts as an obstacle for families who receive PSB services. Since parental stress is influenced by multiple factors across parenting (such as age, education, and psychological functioning), the child domain (including children’s traits, such as health, mood, and behavioural problems), and the parent–child relationship (including the quality of proximity or conflict), it is not solely dependent on parent–child behavioural interactions. Therefore, parental stress is not substantially reduced during these treatments and may be considered as a potential exclusion criterion for participation.
Conclusion
According to the results of the research, CBT-PCIT is more effective than CBT in reducing depression and PCIT and CBT-PCIT are more effective than CBT in improving family functioning. Furthermore, family functioning is affected by experimental conditions more than depression. However, no significant difference was found between the experimental groups in parental stress. Therefore, adopting CBT-PCIT therapy to decrease depression, using PCIT or CBTPCIT to improve family functioning, could be a valuable approach to support these adolescents. Additionally, to strengthen the applicability of future findings, it is recommended that other adolescent vulnerabilities, including developmental problems and other family adversities, such as lack of guidance and supervision, parental depression, and substance use, be examined.
Limitations and future directions
Regarding the limitations of this study, the limited sample size and the absence of a control group reduce the strength of the findings. Additionally, maternal reporting bias and cultural factors affecting the reporting of sexual behaviours may influence the results, and since the treatments were administered by the researcher, there is an increased risk of therapist-related bias. Comparing treatment effectiveness between boys and girls, follow-up assessments to examine the durability of treatment effects, systemic factors as the third category of variables, can be addressed in future research. Moreover, delivering these interventions in a complementary and multifaceted way within schools, including training for school staff, may increase their overall effectiveness.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Guilan, Rasht, Iran (Code: IR.GUILAN.REC.1402.053). To comply with ethical standards, written informed consent was obtained from all participants prior to their involvement in the study. Participation was entirely voluntary, and no coercion was involved. The information about the participants was kept confidential.
Funding
This article was extracted from the doctoral dissertation of Fatemeh Mehrvarz, approved by the University of Guilan, Rasht, Iran.
Authors' contributions
Data collection, funding acquisition and resources: Fatemeh Mehrvarz; Data analysis: Fatemeh Mehrvarz and Abbas Abolghasemi; Conceptualization and supervision: Abbas Abolghasemi, Mahvaz Khosrojavid and Abbas Ali Hosseinkhanzadeh; Investigation, Writing the original draft, review & editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors are grateful to the participants who cooperated in data collection.
References
Aolescence is widely acknowledged as a critical phase marked by significant changes in physical, cognitive, and socioemotional domains, the effects of which often extend into adulthood (Cheng et al., 2024). One of the crucial aspects of growth in adolescence is sexual growth (Hackett et al., 2013). Problematic sexual behaviour (PSB) consists of a sexual part of the body (genitals, breasts) includes, interference with a person’s growth, using coercion, intimidation, or force, physical injuries, continuing and addictive behaviours, and sexual activity (Mori et al., 2023; Pistre et al., 2023; Hacket et al., 2013). According to Davis et al. (2003), the development of PSBs can be influenced by four categories of factors in individuals: child and adolescent vulnerabilities, including developmental problems; family adversities, such as lack of guidance and supervision, stress, parental depression, and substance use; sexual modelling; and coercive modelling. A developmental period of the greatest risk for PSBs exposure is late childhood and early adolescence (ages 10–14) (Finkelhor et al., 2009; Pistre et al., 2023). Overall, almost 47% of adolescents worldwide have experienced sexual behaviours, and 6% of them experienced the first sex before age 13 (Delago et al., 2020). In Iran, the prevalence of sexual relationships among teenage boys and girls has been reported to range from 12.8% to 20%(Alimoradi et al., 2017).
One of these adolescent vulnerabilities for PSB can be depression. According to Aaron Beck’s theory (1976), which is also applicable to children and adolescents (Beck & Alford, 2009), depression results from automatic negative thoughts, dysfunctional schemas, and cognitive distortions, including a negative outlook toward oneself, the world, and what lies ahead. Studies have shown that adolescent sexual experiences and behaviours are associated with depression (Boyd et al., 2022), and this relationship is stronger in younger adolescents (Savioja et al., 2015). Sexual behaviours are a breakthrough attempt to regulate emotions, and depression among PSBs means overcoming negative emotions (Craparo, 2014), and is related to the way parents respond to these emotions (Whalen, 2020).
As mentioned, besides adolescent vulnerabilities, family adversities have a major role in children’s problems. The McMaster model considers six aspects of family functioning: Problem solving, communication, roles, emotional response, emotional involvement, behaviour control (Epstein, 1993). Studies have shown that the functioning of the family directly and indirectly predicts the behavioural problems of children (Song et al.,2023; Du et al., 2020, Abbass ghorbani & Naghdi, 2020; Mirzaaghasi et al., 2019; Wang et al., 2021), and parental depression plays a moderate role (Du et al., 2020). Another crucial family adversity is parental stress. According to Abidin’s (2016) model, there are three areas for parental stress: parent, child, and parent-child relationship (Deckard, 2020). The results of the studies show parents’ stress is a positive predictor of children’s behavioural problems (Thériault et al., 2025; Cook et al., 2024; Khoshkerdar et al., 2020) and parental depression plays a moderate role in the relation of family functioning and behavioural problems of children (Du et al., 2020). Additionally, parenting stress is a barrier for families who receive intervention for PSBs (Shields et al., 2018)
Adolescents with PSBs achieve the desired result by treatments (Grady et al., 2023), such as PCIT and CBT (Shawler, et al. 2018, Jenkins et al., 2020). PCIT, which addresses behavioural issues by focusing on both adolescents and their caregivers (Bonner et al., 2017), pursues goals, such as strengthening parent-child relationships, while decreasing behavioural issues; parental skills, including positive discipline, reducing parental stress and shame (O’Toole et al., 2021; Warren et al., 2022; Hashemi & Eyni ,2020) and depression (Fatemi et al., 2022; Wessing et al., 2015), improving family functioning (Sharifi & Sepehvand ,2023). Additionally, parents’ parenting styles are related to family functioning (Abbass ghorbani & Naghdi, 2020) and parent-child relationships marked by minimal conflict strengthen the connection between mindful parenting and maternal depression (He et al.,2025). CBT treatment is a family-based, psychological and supportive group treatment consisting of behavioural and cognitive discipline (Silovsky et al., 2018), has strong empirical evidence to reduce internal and external behaviour problems (Hacket et al., 2013; Jenkins et al., 2020; Silovsky et al., 2018) characteristic clinical features of depression (Lisoy et al., 2024; Murray et al., 2015; Samavatyan et al., 2021) and decrease in parental stress (Gusler et al., 2023).
According to the background of the research, PSBs can be an obstacle to the normal transformation of late childhood and early adolescence (ages 10–13) and can damage them or their families; and according to the high prevalence and early onset, the researchers believe this study can contribute to early identification and intervention of PSBs. Moreover, to date, most research have only reviewed proposed therapies for PSB and the effectiveness of them or their combinations—even internationally—has been examined in only a few studies, which primarily focused on PSBs itself, rather than its underlying factors. Also, personal vulnerabilities and family adversities, which are identified in this study, have not been examined in other studies yet. To address this gap, the aim of the present study is to compare
Materials and Methods
This study is a quasi-experimental study with a pre-test-post-test design with three experimental groups and without a control group. The statistical population of the present study consisted of all primary school students with PSBs in Guilan Province, Iran, during the 2023-2024 academic year. The sample of the study included 35 female primary school students aged 10-13 years with PSBs, who were identified through purposive sampling based on the cut-off point in the PSBs Questionnaire and through semi-structured clinical interviews based on the diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) (McKibbin et al., 2017). To comply with ethical guidelines, the present study was conducted exclusively with female participants. Considering the presence of three experimental groups and two time points (pre-test and post-test), the sample size and assignment of participants to each group were determined using Cohen’s sample-size tables based on the F-ratio (Cohen, 1988). The degrees of freedom for the table were calculated using the Equation 1:
1. Degrees of freedom (u)=(r−1)×(c−1)=(3−1)×(2−1)=2
The minimum sample size for degrees of freedom equal to 2, considering a confidence level of 95%, test power of 80%, and an effect size of 0.50, was determined to be 10 participants per group. In this study, accounting for possible attrition of participants, 12 individuals were selected for two groups and 11 individuals for one group, and were randomly assigned to the groups. Randomization was performed using a table of random numbers to ensure unbiased and fully random allocation of participants to the study groups.
Top of Figure 1, the inclusion criteria included age (10 to 13 years), gender (female), tendency to participate and collaborate in the research. The exclusion criteria included physical and psychological diseases (direct question), consumption of psychiatric drugs (direct question), receiving other psychological therapies (direct question), and more than two absences from therapy sessions, and a very high score in the PSB questionnaire.
Study instruments
Clinical Interview: Semi-structured interviews of six provided treatments (McKibbin et al., 2017) and the clinical interview based on the DSM-5 were used.
Child and Adolescent Sexual Behaviour Checklist: The Child and Adolescent Sexual Behaviour Checklist (Friedrich, 1998) for children aged 2-12 years includes 37 items and 9 main content areas: boundary issues, gender role behaviour, sexual interest, sexual knowledge, nudism, self-stimulation, sexual influence, behavioural attitude, and sexual anxiety, rated on a 5-level Likert scale. The main caregiver ranked the behaviours they observed during the past six months on a four-point scale from 0 (never) to 4 (at least once a week). Cronbach’s α on the normal sexual behaviour scale in children was equal to 0.77, and Cronbach’s α for each component was between 0.75 and 0.78 (Kareshki et al., 2019). The Cronbach’s α of this scale in this research was 0.77. In this study, it was also administered to participants aged 13, given the minimal developmental differences at this age.
Maria Kovacs children’s depression questionnaire: The Child Depression Questionnaire is a self-reported scale designed by Kovacs (1992) for children and adolescents aged 7-17 years and includes 27 items and 3 main content areas: behavioural, cognitive, and emotional symptoms of depression, based on the Likert scale from 0 to 2 (for A to C). The reliability coefficients for the two inventories—the Maria Kovacs and Beck questionnaires—were reported as 0.789 and 0.526, respectively. Furthermore, when comparing the Maria Kovacs inventory to the Beck inventory (used as the criterion test), it was found that a non-depression score range of 0–8 on the Kovacs inventory corresponded to a sensitivity of 97.2%, specificity of 46.1%, and positive and negative predictive values of 85.7% (Mirzaie et al., 2019). The Cronbach’s α of this scale in this research was 0.78.
Family functioning questionnaire: The family functioning questionnaire was designed by Epstein et al (1983) based on McMaster’s pattern, and includes 60 items and 7 main content areas: problem solving, communication, roles, emotional companionship, emotional intercourse, behaviour control of family functioning, and overall function of the family, which are rated on a 4-level Likert ranging from 1 to 4 “strongly agree,” “agree», “disagree,” and “strongly disagree”. A high score means unhealthy functioning. This tool has a good internal consistency from 0.72 to 0.92 with its subscales from 0.72 to 0.92. Cronbach’s α was calculated for 60 items and 7 subscales as 0.83 and 0.82, respectively. Its total reliability was 0.79 (Eimani & Shiralinia, 2015). The Cronbach’s α of this scale in this research was 0.72.
Parenting stress scale: The parenting stress scale was designed by Berry and Jones (1995) and includes 18 items that are rated on a 5-level Likert scale from 1 to 5, “completely agree,” “agree”, “no opinion “,”disagree,” and “completely disagree”. The items relate to the positive aspects of parental tasks, as well as their negative aspects. Berry and Jones have examined the reliability of the tool in the test-re-test method and reported this scale to be 80%. In a preliminary study conducted to assess the validity of the scale translated into Persian, the test-re-test reliability was reported as 0.78 (Paghandeh, 2019). Additionally, the reliability of the instrument was reported by Mohtashami et al. (2012) using Cronbach’s α, yielding a value of 0.73. The Cronbach’s α of this scale in this research was 0.71.
Parent-child interaction therapy (PCIT) for Problematic sexual behaviours (PSBs): The PCIT is a family-based approach designed to address behavioural issues, focusing on two key skill categories: Child-related skills and caregiver-related skills. In this therapy, mothers can effectively take on the role of a therapist for their children (Bonner et al., 2017). The PCIT treatment specifically designed for PSBs was introduced by Allen et al. (2016). For the purposes of this research, PCIT was implemented by rigorously applying the principles and techniques of this therapy over 18 weekly 1-hour sessions, lasting 4 to 5 months, and exactly based on the treatment protocol. During these sessions, two general types of interactions (child-directed interaction [CDI] and parent-directed interaction [PDI]) were developed within families. The treatment included clinical assessment and treatment planning along with psychoeducation for 2 sessions, CDI training for 5 sessions, PDI training for 7 sessions, and completion of the treatment plan over 4 sessions (Appendix 1).
Cognitive-behavioural therapy (CBT) for PSBs: The CBT for PSBs is a family-based, psychoeducational, and supportive group therapy aimed at reducing or eliminating incidents of such behaviours. The CBT treatment specifically designed for PSBs was introduced by Silovsky et al. (2013). Like PCIT, this approach was also implemented over 18 weekly 1-hour sessions, taking place over 4 to 5 months. The key clinical components for the child and caregiver include rules regarding sexual behaviour and boundaries, abuse prevention skills and safety planning, emotional regulation and coping skills, impulse control and problem-solving skills for children, developmentally appropriate sexual education, social skills and peer relationships, and acknowledgment of sexual behaviour, apology, and restitution. Additional key clinical components for caregivers include behavioural parent training for the prevention of and response to PSB and other behavioural issues; promoting the child’s overall development with an emphasis on psychological and emotional changes; correcting misconceptions about PSB and their consequences for the child; communicating effectively with children about sexual behaviour and development; and supporting children’s use of coping and decision-making skills (Silovsky et al., 2018) (Appendix 2).
Combination of Parent-Child Interaction and (CBT): This research utilized a combined approach based on common factors, emphasizing the shared elements of the two therapies over their unique components, thus leading to more effective treatment outcomes (Norcross & Goldfried, 2005). The combined therapy integrated key aspects of both PCIT and CBT, including clinical assessment, treatment planning, and introduction to treatment over 2 sessions, psychoeducation over 4 sessions, CDI training over 4 sessions, and PDI training along with sexual knowledge over 4 sessions. Additionally, the stage of sexual education, understanding, and prevention of sexual abuse was conducted over 2 sessions, followed by completion of the treatment plan over 2 sessions. The formal validity of the treatment package was evaluated and confirmed by supervisors and advisors based on criteria, such as alignment of components with treatment goals, comprehensiveness, and content coherence. The evaluation indicated that the selected components from the two therapeutic approaches have conceptual overlap and are complementary, making their integration scientifically and practically justified.
Furthermore, the integrated treatment package was pilot-tested with five previous clients of the center. Based on their feedback, the content of the intervention was considered satisfactory in terms of coherence, clarity of concepts, and alignment with treatment needs, and minor adjustments were made to the delivery of the sessions. This combined approach was carried out over 18 weekly sessions, spanning 4-5 months.
Participants and procedure
This study was conducted after obtaining the necessary approvals from the Faculty of Literature and Humanities at the University of Guilan. The researcher subsequently approached the Counseling Center of District 1, Rasht City, Iran, and, with the support of academic supervisors, obtained permission to conduct the study. Parents of female elementary school students were informed about the study through school principals and counselors, using both in-person meetings and virtual communication via the Shad platform. They were invited to participate if they were interested in receiving training related to their children’s sexual development. To enhance parental engagement, the researcher emphasized the high prevalence of problematic sexual behaviors, the importance of early adolescence education in preventing future sexual disorders, the ethical and cultural considerations of the study, and the confidentiality of participants’ information. Parents were also instructed to attend the initial assessment and interviews without their children to ensure ethical standards.
A total of 63 interested parents visited the counseling center and voluntarily completed the Problematic Sexual Behavior Questionnaire regarding their child. Subsequently, the researcher conducted semi-structured clinical interviews with the parents based on the DSM-5 criteria (McKibbin et al., 2017). Based on the questionnaire and interview results, 38 students who scored above 20 on the problematic sexual behavior questionnaire and exhibited early-stage problematic sexual behaviors (e.g. touching, voyeurism, weak boundaries, and interest in the opposite sex) were identified.
After applying inclusion and exclusion criteria, 35 students meeting all criteria were selected as adolescents with problematic sexual behaviors. Their parents were invited to participate in the interventions, and the adolescents were randomly assigned to three treatment groups using a random number table. After completing the questionnaires related to the study variables, treatment sessions were implemented. During treatment, five individuals were excluded from the research due to absence of more than two sessions.
In this study, 18 PSB-CBT and PCIT treatment sessions were held within 4-5 months. These sessions were conducted by the researcher and at the Centre of Psychological Services and included individual and combined sessions of children and parents. To minimize interaction between the groups, separate time slots were allocated for each group’s attendance at the center. Participants were instructed not to disclose or discuss the type of treatment they were receiving with others. Although all sessions were delivered by a single therapist, the use of a detailed standardized treatment manual helped minimize therapist-related biases. To maintain participants’ motivation and minimize dropouts, a respectful and supportive relationship was established between the researcher and participants. Session schedules were adjusted based on participants’ availability, with reminders sent one day prior via the Shad messaging platform. Missed sessions were supplemented with audio summaries sent to parents and children, and key concepts from previous sessions were briefly reviewed at the start of each session. Finally, after completing complete treatment sessions, the post-test was administered, and data were analysed using SPSS software, version 27.
Results
In the descriptive statistics section, results obtained from the one-way analysis of variance (ANOVA) indicated no significant difference in the mean age of students (P>0.05, F=0.7) and no significant difference in the mean age of mothers across the experimental groups (P>0.05, F=1.11). Also, the results of the chi-square test showed no significant difference in the frequency of participants across the experimental groups in birth order (P>0.05, χ²(3)=0.95), mothers’ education (P>0.05, χ²(3)=2.40), and family economic status (P>0.05, χ²(3)=1.25). Table 1 presents the means and standard deviations of the research variables in the test groups and in the pre-test and post-test. To check the normality of the variables, the Shapiro-Wilk test was employed, and the results revealed that the assumption of normality of all the variables in the pre-test and post-test was met and the distribution of all the variables was normal (P>0.05).
To examine the assumption of homogeneity of regression slopes for the pre-test and post-test scores across experimental groups, an F-test was conducted. The results of this test for depression variable were (F=0.83, P=0.49) and family function were (F=0.53, P=0.49). Neither variable was significant (P>0.05). The results indicated no significant interaction between the treatments and the pre-test scores, suggesting that the assumption of homogeneity of regression slopes was met and that performing analysis of covariance (ANCOVA) was appropriate. However, for the parental stress variable (F=66.61, P=0.001), the results showed a significant interaction between the treatments and the pre-test scores (P<0.05), indicating that the assumption of homogeneity of regression slopes was violated. Therefore, we must use the one-way ANOVA instead. To determine the homogeneity of the test groups in the post-test, Levene’s test was used to compare group variances. The results for the depression variable were (F=3.325, df=2, P=0.05) and for the family functioning variable were (F=1.337, df=2, P=0.28). Both variables were not significant (P>0.05). It can be said that the variances are equal in experimental groups; therefore, further analysis of this variable was not performed.
The results of ANCOVA have been reported to determine post-test differences between the test groups, by controlling the pre-test effect, as presented in Table 2. Results for depression were (F=4.83, df=2, P=0.01, observed power [OP]=0.78). This table shows a significant difference between the experimental groups for the depression variable (P≤0.05). The eta squared (η²) indicates that 27% of the variance in depression can be explained by the experimental conditions. In addition, the results for family functioning were (F=18.14, df=2, P=0.00, OP=1.00). This table shows a significant difference between the experimental groups in the family functioning variable (P≤0.05). The eta squared (η²) indicates that 58% of the variance in family functioning can be explained by the experimental conditions.
To examine which experimental groups showed differences in depression scores, a Bonferroni test with a 95% confidence interval was conducted. The results indicate that a significant difference was found in depression scores only between the CBT group and the PCIT-CBT group (P≤0.05). The comparison between the CBT and PCIT groups revealed no significant difference, nor was a significant difference found between the PCIT and CBT-PCIT groups (P>0.05). According to the mean scores of the experimental groups in Figure 2, the depression score of the CBT group is 10.05, the score of PCIT group is 8.55, and the score of CBT-PCIT group is 7.29. The depression scores of participants in the CBT-PCIT group are lower than those of participants in the CBT group. Based on this finding, it can be inferred that the combined therapy is more effective than CBT in reducing depression.
To examine which experimental groups showed differences in family functioning scores, a Bonferroni test with a 95% confidence interval was conducted, and the results indicated that a significant difference is observed between the CBT group and the PCIT group, as well as between the CBT group and the PCIT-CBT group (P<0.001). However, no significant difference was found between the PCIT and CBT-PCIT groups (P>0.05). The mean family functioning score shown in Figure 3 were as follows: 95.93 for the CBT group, 88.46 for the PCIT group, and 85.71 for the PCITCBT group. The results showed that the adjusted mean of family functioning scores of participants in the PCIT and CBT-PCIT groups were lower than those of participants in the CBT group. Since a lower score in family functioning indicates a more favourable outcome, it can be concluded that PCIT and CBT-PCIT are more effective than CBT in improving family functioning.
For the parental stress variable, due to the lack of assumptions of the regression slope required for ANCOVA, we could not use ANCOVA; therefore, we used one-way ANOVA instead. To determine the homogeneity of the experimental groups, Levene’s test was used to compare group variances. The results for the parents’ stress variable were (F=0.440, df=2, P=0.65) and were not significant (P>0.05), indicating that the variance of this variable was equal in experimental groups; therefore, further analysis of this variable was not performed.
In Table 3, the results of the one-way ANOVA showed no significant differences among the experimental groups (F=2.76, df=2, P=0.08). The results showed no significant difference among experimental groups in the parental stress variable (P>0.05).
Discussion
This study aimed to compare the effectiveness of PCIT, CBT, and their combination on depression, family functioning, and parenting stress among adolescents with PSB. The findings of the present study revealed a significant difference between the experimental groups in the depression variable and 27% of the variance was explained by the experimental conditions of this research. Furthermore, CBT-PCIT was more effective than CBT in reducing depression. The results of this study were consistent with previous research that has shown a relationship between childhood sexual behaviours and depression (Savioja et al., 2015) and that PCIT and CBT lead to changes in depressive cognitions and a reduction in clinical symptoms of depression (Lisoy et al., 2024; Murray et al., 2015; Wessing et al., 2015; Samavatian et al., 2021; Fatemi et al., 2022). This convergence may stem from the shared emphasis on cognitive restructuring, enhanced emotional regulation mechanisms, and parenting skills.
These findings extend prior evidence by demonstrating that combining CBT with parent–child interaction components can yield broader and more sustainable outcomes, particularly in contexts where relational stressors play a central role in depressive symptomatology.
As mentioned earlier, depression results from automatic negative thoughts, dysfunctional schemas, and cognitive distortions. In this study, the combined therapy involved teaching parent-child relationship skills, which included behaviour management and communication, reducing stigma and shame, addressing myths and misconceptions, fostering hope, recognizing and expressing emotions, self-control skills, and emotional regulation, as well as family reunification. Alongside these, cognitive-behavioural skills were taught, including self-control and self-soothing strategies, using behavioural techniques to stop unhealthy thoughts or actions, cognitive restructuring, identifying erroneous beliefs, challenging thoughts, teaching social skills, applying self-control to sexual behaviour rules, enhancing self-control cues, creating and maintaining friendships, peer pressure management, preventing abuse, empathy, and apologizing. These interventions collectively contributed to the improvement of depression in these adolescents.
Regarding differences between these two approaches, CBT primarily targets intrapersonal factors of depression by modifying dysfunctional cognitions, maladaptive beliefs, and avoidance behaviours. Its mechanisms of change are largely cognitive and behavioural, aiming to restructure thought patterns and promote adaptive actions. In contrast, PCIT focuses on interpersonal and emotional dimensions by enhancing the quality of parent-child interactions, strengthening attachment security, and improving emotion regulation through responsive and supportive relationships. The therapist guides parents to become emotionally attuned and behaviorally consistent, which creates a more nurturing family environment. Thus, while CBT operates mainly through cognitive restructuring and behavioural activation, PCIT facilitates emotional regulation and relational repair through experiential learning within the parent–child dyad. Integrating these two approaches addresses both the internal cognitive processes and the external relational context that contribute to depressive symptomatology. The presence of the parent as an active agent of change extends the therapeutic process beyond the clinical setting, allowing newly acquired emotional and behavioural skills to be practiced and reinforced in daily interactions. This generalization of therapeutic gains may explain the greater durability and magnitude of symptom reduction observed in the integrated treatment. Overall, by simultaneously targeting cognitive distortions, emotional dysregulation, and relational insecurity, the combined CBT–PCIT model provides a more comprehensive and ecologically valid framework for treating depression. This integrative approach leverages complementary mechanisms of change—cognitive insight and emotional connection—to foster deeper and more sustainable therapeutic outcomes than CBT alone.
Moreover, the findings of the present study indicated a significant difference between the experimental groups in family functioning and 58% of the variance was explained by the experimental conditions of this research. PCIT and CBT-PCIT were more effective than CBT in improving family functioning. These results align with those reported in earlier studies showing that adolescents’ behavioural problems are related to family functions and behavioural and family based education can improve family functioning (Song et al.,2023; Du et al., 2020; Ghorbani & Naghdi, 2020; Mirzaaghasi et al., 2019; Wang et al., 2021; Sharifi & Sepehvand , 2023; Silovsky, 2020). It may be explained by the fact that PCIT directly targets patterns of interaction, communication, and emotional responsiveness within the family system, domains that are only indirectly addressed in traditional CBT. Moreover, the inclusion of parents as active participants likely facilitated the generalization of therapeutic gains to the home environment. These findings extend prior evidence by demonstrating that interventions combining cognitive restructuring with relational and systemic components can yield broader improvements in family functioning, beyond symptom reduction alone.
We also found that the effect size for the depression variable was 0.27, while that for the family functioning variable was 0.85. This shows that the family functioning was affected by experimental conditions more than the depression variable. This can be explained by the fact that, first, PCIT directly targets parent–child interactions, which are the core components of family functioning, whereas subclinical depressive symptoms are internal and may be less responsive to interaction-focused strategies. Second, observable behavioural changes can occur relatively quickly, while changes in mood and cognition often require longer periods and more intensive cognitive work.
As mentioned, PCIT can lead to improvements in parenting skills and positive discipline, enjoyment of shared time, parental control over standards, direct targeting of dysfunctional behaviours, and family reunification in two stages, thereby improving family functioning. Since caregivers in this therapy learn a systematic approach to discipline and practice behavioural management and communication skills, they can influence family functioning aspects, such as problem-solving, communication, roles, emotional responsiveness, emotional involvement, and behaviour control. Additionally, the combined treatment, with its focus on emotional regulation and coping skills, impulse control and problem-solving for children, developmentally appropriate sexual education, social skills, peer relationships, and affirmation of sexual behaviours, as well as behavioural techniques to stop unhealthy thoughts or actions, cognitive restructuring, identifying misconceptions, apologizing, and compensating, alongside family components, can lead to the improvement of family functioning.
Additionally, the results showed no significant difference between the experimental groups in the parental stress variable. Previous studies have shown that parents’ stress is associated with children’s behaviour and parent-child relationship (He et al., 2025; Cook et al., 2024; Hashemi & Eyni, 2020, Khoshkardar et al., 2020) and CBT can lead to a decrease in parental stress (Gusler, 2023) and PCIT is effective in reducing parental stress (Warren et al., 2022). Previous studies did not compare the effectiveness of these kinds of therapies on parent stress. Therefore, the findings from this study on parental stress are not consistent with previous studies. Several factors may explain this finding. First, parental stress was not necessarily severe at baseline, limiting the potential for measurable reductions. Second, while the interventions targeted child behaviour and parent–child interactions, they did not directly focus on stress management or coping strategies for parents. Third, changes in parental stress may require longer or more intensive interventions, as short-term programs are more likely to produce observable improvements in family functioning or child behaviour.
The parent-child-relationship model (Abidin, 2016) presents three domains for parental stress: the parent, the child, and the parent-child relationship. Research in this area shows that parental stress acts as an obstacle for families who receive PSB services. Since parental stress is influenced by multiple factors across parenting (such as age, education, and psychological functioning), the child domain (including children’s traits, such as health, mood, and behavioural problems), and the parent–child relationship (including the quality of proximity or conflict), it is not solely dependent on parent–child behavioural interactions. Therefore, parental stress is not substantially reduced during these treatments and may be considered as a potential exclusion criterion for participation.
Conclusion
According to the results of the research, CBT-PCIT is more effective than CBT in reducing depression and PCIT and CBT-PCIT are more effective than CBT in improving family functioning. Furthermore, family functioning is affected by experimental conditions more than depression. However, no significant difference was found between the experimental groups in parental stress. Therefore, adopting CBT-PCIT therapy to decrease depression, using PCIT or CBTPCIT to improve family functioning, could be a valuable approach to support these adolescents. Additionally, to strengthen the applicability of future findings, it is recommended that other adolescent vulnerabilities, including developmental problems and other family adversities, such as lack of guidance and supervision, parental depression, and substance use, be examined.
Limitations and future directions
Regarding the limitations of this study, the limited sample size and the absence of a control group reduce the strength of the findings. Additionally, maternal reporting bias and cultural factors affecting the reporting of sexual behaviours may influence the results, and since the treatments were administered by the researcher, there is an increased risk of therapist-related bias. Comparing treatment effectiveness between boys and girls, follow-up assessments to examine the durability of treatment effects, systemic factors as the third category of variables, can be addressed in future research. Moreover, delivering these interventions in a complementary and multifaceted way within schools, including training for school staff, may increase their overall effectiveness.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Guilan, Rasht, Iran (Code: IR.GUILAN.REC.1402.053). To comply with ethical standards, written informed consent was obtained from all participants prior to their involvement in the study. Participation was entirely voluntary, and no coercion was involved. The information about the participants was kept confidential.
Funding
This article was extracted from the doctoral dissertation of Fatemeh Mehrvarz, approved by the University of Guilan, Rasht, Iran.
Authors' contributions
Data collection, funding acquisition and resources: Fatemeh Mehrvarz; Data analysis: Fatemeh Mehrvarz and Abbas Abolghasemi; Conceptualization and supervision: Abbas Abolghasemi, Mahvaz Khosrojavid and Abbas Ali Hosseinkhanzadeh; Investigation, Writing the original draft, review & editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors are grateful to the participants who cooperated in data collection.
References
Abidin, R. (2016). Manual for the parenting stress index. Odessa: Psychological Assessment Resources. [Link]
Alimoradi, Z., Kariman, N., Simbar, M. & Ahmadi, F. (2017). Contributing factors to high-risk sexual behaviours among iranian adolescent girls: A systematic review. International Journal of Community Based Nursing & Midwifery, 5(1), 2-12. [PMID]
Allen, B., Timmer, S. G., & Urquiza, A. J. (2016). Parent-Child Interaction Therapy for sexual concerns of maltreated children: A preliminary investigation. Child Abuse & Neglect, 56, 80 –88. [DOI:10.1016/j.chiabu.2016.04.008]
Beck, A. T., & Alford, B. A. (2009). Depression: Causes and treatment (2nd ed.). Philadelphia: University of Pennsylvania Press. [Link]
Berry, J. D., & Jones, W. H. (1995) The parental stress scale: initial psychometric evidence. Journal of Social and Personal Relationships, 12, 463-472. [DOI:10.1177/0265407595123009]
Boyd, D.T., Abu-Ba’are, G.R., LoVette, A., Whitfield, D.L., Turpin, R.E., Ramos, S.R. et al. (2022). Assessing the influence of child sexual behaviour on depression among black SMM in the southeastern United States. International Journal of Environmental Research and Public Health, 19, 130-39. [DOI:10.3390/ijerph192113930] [PMID]
Cheng, T. W., Mills, K. L., & Pfeifer, J. H. (2024). Revisiting adolescence as a sensitive period for sociocultural processing. Neuroscience and Biobehavioural Reviews, 164, 105820. [DOI:10.1016/j.neubiorev.2024.105820] [PMID]
Cohen, J. (1988). Statistical power analysis for the behavioural sciences (2nd ed.). Mahwah: Lawrence Erlbaum Associates. [Link]
Cook, M., Yan, J., & Butler, K. (2024). Maternal parenting stress and child externalizing behaviours: Low-income as a context. Journal of Applied Developmental Psychology, 93, 0193-3973. [DOI:10.1016/j.appdev.2024.101673]
Craparo, G. (2014). The role of dissociation, affect dysregulation, and developmental trauma in sexual addiction. Clinical Neuropsychiatry, 11(2), 86-90. [Link]
DeLago, C., Schroeder, C., Cooper, B., Deblinger, E., Dudek, E., & Yu, R., et al. (2020). Children who engaged in interpersonal problematic sexual behaviors. Child Abuse & Neglect, 105, 104260. [DOI:10.1016/j.chiabu.2019.104260]
Du, X., & Kim, Y. K. (2020). Family functioning and adolescent behaviour problems: A moderated mediation model of caregiver depression and neighborhood collective efficacy. Children and Youth Services Review, 116, 105270. [DOI:10.1016/j.childyouth.2020.105270]
Eimani M., shiralinia K. (2015). [The role of family functions and process on internet addiction among teenagers (Persian)]. Journal of Family Counseling & Psychotherapy, 5(2), 143-164. [Link]
Epstein, N. B., Baldwin, L. M., & Bishop, D. S. (1983). The mcmaster family assessment device. Journal of Marital and Family Therapy, 9(2), 171–180. [DOI:10.1111/j.1752-0606.1983.tb01497.x]
Epstein, B. E., Ryan, C. E., Bishop, D. S., Miller, I. W., & Keitner, G. I. (1993). The Mc master model: A view of healthy family functioning. Healthy Couple and Family Processes, 21, 581- 607. [DOI:10.4324/9780203428436_chapter_21]
Fatemi A A., Yarmohamadi M., Mohagheghi H., Zoghipaidar M. (2022). The effect of parent and child interaction therapy focused emotional on parent’s reactions to children’s negative emotions in children with depression. Journal of Psychological Science. 21(114), 1215-1228. [DOI:10.52547/JPS.21.114.1215]
Finkelhor D, Cuevas CA, Drawbridge D. (2016). The four precondition models. Hoboken: Wiley Online Library. [DOI:10.1002/9781118574003.wattso002]
Friedrich, W.N., Davies,W.H., Feher, E., & Wright, J. (2003). Sexual behaviour problems in preteen children: Developmental, ecological, and behavioural correlates. NewYork Academy of Sciences, 989(1),95-104. [DOI:10.1111/j.1749-6632.2003.tb07296.x] [PMID]
Ghorbani A., & Naghdi, F. (2020). The relationship between parenting style and family functioning with preschool children’s behavioural problems. Management and Educational Perspective, 2(1), 71-86. [Link]
Grady, M., Yoder, J., Deblinger, E., Mannarino, A. (2023). Developing a trauma focused cognitive behavioural therapy application for adolescents with problematic sexual behaviours: A conceptual framework. Child Abuse & Neglect, 140, 106139. [DOI:10.1016/j.chiabu.2023.106139] [PMID]
Gusler S, Sprang G, Eslinger J. (2023) Parenting stress and children’s trauma symptoms over the course of TF-CBT: Examining differences between relative and foster/adoptive caregivers. Child Abuse Neglect, 137, 106035. [DOI:10.1016/j.chiabu.2023.106035] [PMID]
Hackett, S., Masson, H., Balfe, M., & Philips, J. (2013). Individual, family and abuse characteristics of 700 British child and adolescent sexual abusers. Child Abuse Review, 22, 232-245. [DOI:10.1002/car.2246]
Hashemi, Z. and Eyni, S. (2021). The effectiveness of Parent-Child Interactive therapy on parenting stress and parenting self-efficacy of mothers of children with learning disabilities. Journal of Learning Disabilities, 10(3), 380-393. [DOI:10.32598/JLD.10.3.7]
He, J., Rahman, M. N. B. A., Xu, M., & Jiang, M. (2025). The impact of maternal mindful parenting on preschoolers’ emotional regulation abilities: The mediating role of depression and the moderating role of the parent-child relationship. Acta psychologica, 252, 104685. [DOI:10.1016/j.actpsy.2024.104685] [PMID]
Jenkins, C. S., Grimm, J. R., Shier, E. K., van Dooren, S., Ciesar, E. R., & Reid-Quiñones, K. (2020). Preliminary findings of problematic sexual behaviour-cognitive-behavioural therapy for adolescents in an outpatient treatment setting. Child Abuse and Neglect, 105, 104428. [DOI:10.1016/j.chiabu.2020.104428] [PMID]
Kareshki, H., Mahdavia, S., Khademi, G. & Golmakani, H. (2019). Validity and reliability of normal Sexual Behaviour Scale in Iranian Children. Journal of Clinical Psychology, 11(1), 83-92. [DOI:10.22075/jcp.2019.16129.1539]
Khoshkerdar S. F., Baradaran M., & Ranjbar Noushari F. (2020). The role of parenting styles, parental stress and children’s executive functions deficits in predicting the children’s internalizing and externalizing problems. Quarterly Journal of Child Mental Health, 7(2), 156-168. [DOI:10.29252/jcmh.7.2.14]
Kovacs, M. (1978). Children’s depression inventory (CDI). Washington: APA SysTest. [DOI:10.1037/t19482-000]
Lisøy, C., Neumer, S. P., Adolfsen, F., Ingul, J. M., Rasmussen, L. M. P., & Wentzel-Larsen, T., et al. (2024). Optimizing indicated cognitive behavioral therapy to prevent child anxiety and depression: A cluster-randomized factorial trial. Behaviour Research and Therapy, 176, 104520. [DOI:10.1016/j.brat.2024.104520] [PMID]
McKibbin, G., Humphreys, C., & Hamilton, B. (2017). “Talking about child sexual abuse would have helped me”: Young people who sexually abused reflect on preventing harmful sexual behavior. Child Abuse & Neglect, 70, 210-221. [DOI:10.1016/j.chiabu.2017.06.017] [PMID]
Mohtashami, T., Aliakbari Dehkordi, M., Chimeh, N., Alipor, A., & Ofoghi, H.. (2012). [The effect of traning of pivotal response treatment to mothers of autistic children on family functioning (Persian)]. Journal of Family Research, 8(31), 273-289. [Link]
Mirzaie, P. , Nazarian, L. and Zare, H. (2019). Validation of the Maria Kovacs children’s depression inventory to assess depression among school children in afghanistan. Journal of Midwifery and Reproductive Health, 7(3), 1742-1758. [Link]
Mirzaaghasi R., Boubi M., Dikadeh Fard F. (2019). Predicting children’s internalized behavioural problems based on family function mediated by attachment style. Journal of Psychological Science. 18(84), 2311-2318. [Link]
Mori, C., Park, J., Racine, N., Ganshorn, H., Hartwick, C., & Madigan, S. (2023). Exposure to sexual content and problematic sexual behaviours in children and adolescents: A systematic review and meta-analysis. Child Abuse & Neglect, 143, 106255. [DOI:10.1016/j.chiabu.2023.106255] [PMID]
Murray, L. K, et al. (2015). Effectiveness of trauma-focused cognitive behavioural therapy among trauma-affected children in Lusaka, Zambia: A randomized clinical trial. JAMA Paediatrics, 169(8), 761-769. [DOI:10.1001/jamapediatrics.2015.0580] [PMID]
Norcross, J. C., & Goldfried, M. R. (Eds.). (2005). Handbook of psychotherapy integration (2nd ed.). Oxford: Oxford University Press. [DOI:10.1093/med:psych/9780195165791.001.0001]
O’Toole, C., Lyons, R., Houghton, C. (2021). A qualitative evidence synthesis of parental experiences and perceptions of parent-Child interaction therapy for preschool children with Communication difficulties. Journal of Speech, Language, and Hearing Research, 64(8), 3159-3185. [DOI:10.1044/2021_JSLHR-20-00732] [PMID]
Paghandeh, M., Hassanzadeh, S., & Ghasemzadeh, S. (2019). Effectiveness of parent-child interaction program on parenting stress and parent-hearing impaired child relationship, Journal of Research in Psychological Health, 13(1), 99-124. [Link]
Pistre, N., Schreck, B., Grall-Bronnec, M., & Fatseas, M. (2023). Should problematic sexual behaviour be viewed under the scope of addiction? A systematic review based on DSM-5 substance use disorder criteria. Addictive Behaviours Reports, 18, 100510. [DOI:10.1016/j.abrep.2023.100510] [PMID]
Samavatyan, H., kalantari, M., aslipoor, A., & Abedi, A. (2021). The effectiveness of parent-child cognitive behavioural therapy on emotional behavioural problems of grief children. Counseling Culture and Psycotherapy, 12(47), 195-220. [DOI:10.22054/qccpc.2021.60104.2674]
Savioja, H., Helminen, M., Fröjd, S., Marttunen, M., & Kaltiala-Heino, R. (2015). Sexual experience and self-reported depression across adolescent years. Health Psychology And Behavioural Medicine, 3(1), 337-347. [DOI:10.1080/21642850.2015.1101696]
Sharifi M, Sepahvand T. (2023). The effectiveness of child parent relationship therapy (CPRT) on dimesions of family functioning in mothers of preschool children: A quasi-experimental study. Journal of Rafsanjan University of Medical Sciences, 22 (7), 677-690. [DOI:10.61186/jrums.22.7.677]
Shawler, P. M., Bard, M. E., Taylor, E. K., Wilsie, C., Funderburk, B., & Silovsky, J. F. (2018). Parent-child interaction therapy and young children with problematic sexual behaviour: A conceptual overview and treatment considerations. Children and Youth Services Review, 84, 206-214, [DOI:10.1016/j.childyouth.2017.12.006]
Shields, J. D., Klinkebiel, C. M., Taylor, E. K., Espeleta, H. C., Beasley, L. O., & Silovsky, J. F. (2018). A qualitative analysis of family perspective on treatment services for youths with problematic sexual behavior. Victims & Offenders, 13(7), 955-973. [DOI:10.1080/15564886.2018.1506853]
Silovsky, J. F., Hunter, M. D., & Taylor, E. K.(2018). Impact of early intervention for youth with problematic sexual behaviors and their caregivers. Journal of Sexual Aggression, 1–12. [DOI:10.1080/13552600.2018.1507487]
Silovsky, J. F., Letourneau, E. J., & Bonner, B. L. (2020). Introduction to CAN special issue: Children with problem sexual behaviour. Child Abuse & Neglect, 105, 104508. [DOI:10.1016/j.chiabu.2020.104508] [PMID]
Song, Q., Su, W., Li, N., Wang, H., Guo, X., Liang, Q., et al. (2023). Family function and emotional behaviour problems in Chinese children and adolescents: A moderated mediation model. Journal of Affective Disorders, 341, 296-303. [DOI:10.1016/j.jad.2023.08.138] [PMID]
Theriault, R. L., Bernier, A., & Deneault, A. A. (2025). Maternal and paternal parenting stress: Direct and interactive associations with child externalizing and internalizing behavior problems. Early Childhood Research Quarterly, 71, 114-122. [DOI:10.1016/j.ecresq.2024.12.006]
W. N. Davis, W., Feher, E., & Wright, J. (2003). Sexual behaviour problems in preteen children. Annals of the New York Academy of Sciences, 989, 95-104. [DOI:10.1111/j.1749-6632.2003.tb07296.x] [PMID]
Wang, Q., Peng, S., Chi, X. (2021). The relationship between family functioning and internalizing problems in Chinese adolescents: A moderated mediation model. Frontiers in Psychology, 24(12), 64-42. [DOI:10.3389/fpsyg.2021.644222] [PMID]
Warren, J. M., Halpin, S. A., Hanstock, T. L., Hood, C., & Hunt, S. A. (2022). Outcomes of parent-child interaction therapy (PCIT) for families presenting with child maltreatment: A systematic review. Child Abuse & Neglect, 134, 105942. [DOI:10.1016/j.chiabu.2022.105942] [PMID]
Wessing I., et al. (2015). Cognitive emotion regulation in children: Reappraisal of emotional faces modulates neural source activity in a frontoparietal network. Developmental Cognitive Neuroscience, 13, 1-10. [DOI:10.1016/j.dcn.2015.01.012] [PMID]
Whalen, D.J., Gilbert, K.E., & Luby, J.L. (2021). Changes in self‐reported and observed parenting following a randomized control trial of parent -child interaction therapy for the treatment of preschool depression. Journal of Child Psychology and Psychiatry, 62(1), 86 -96. [DOI:10.1111/jcpp.13263] [PMID]
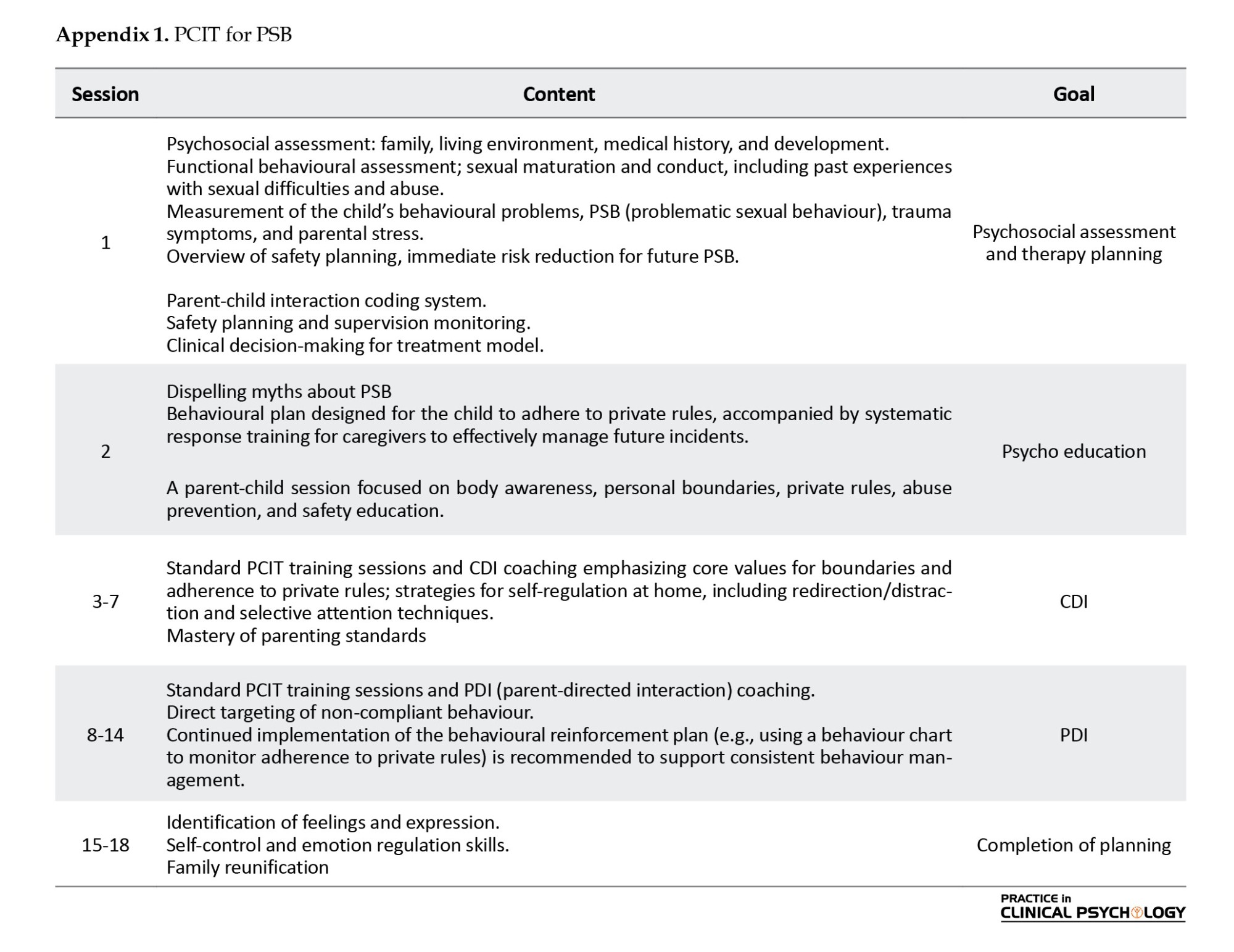
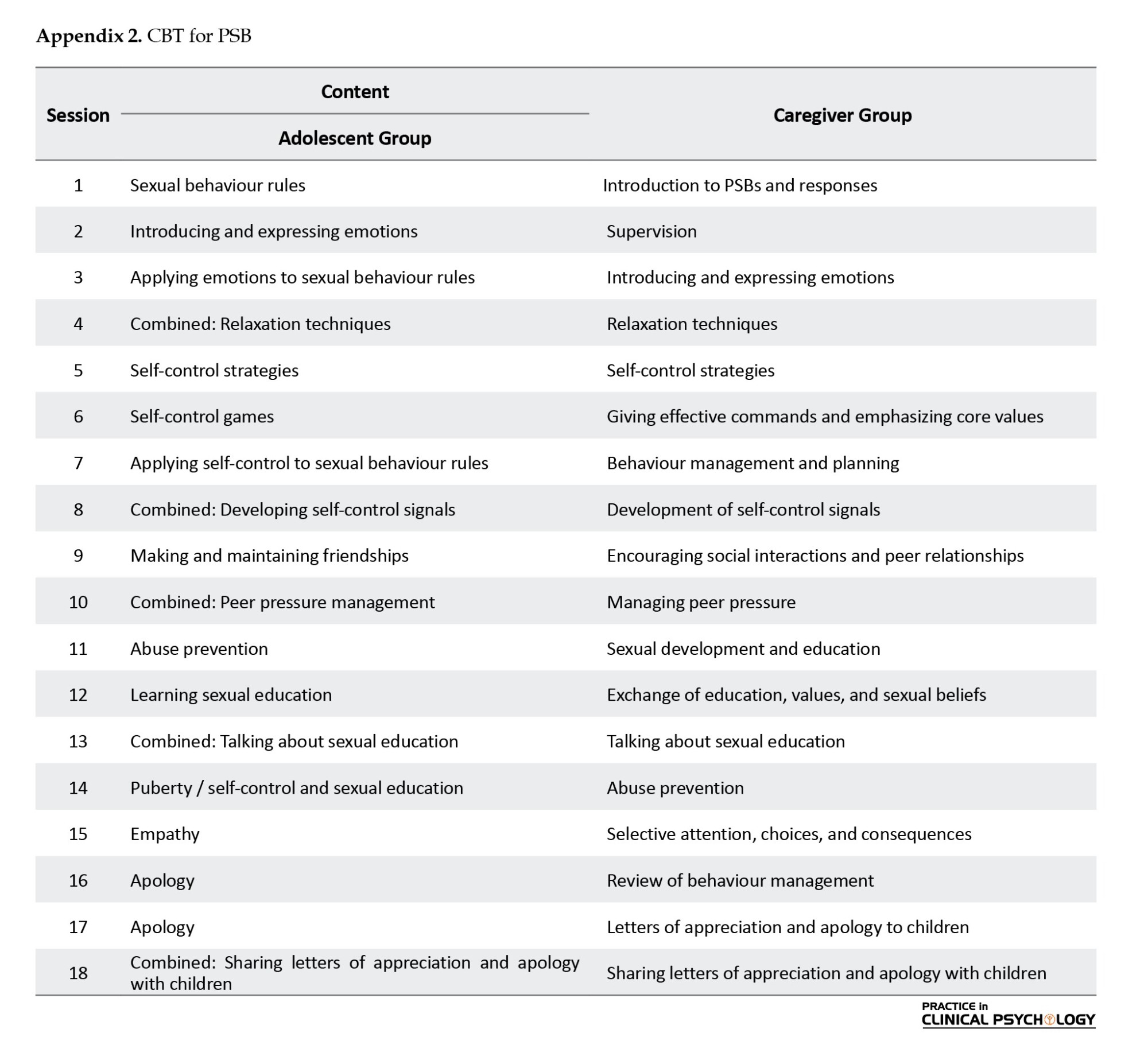
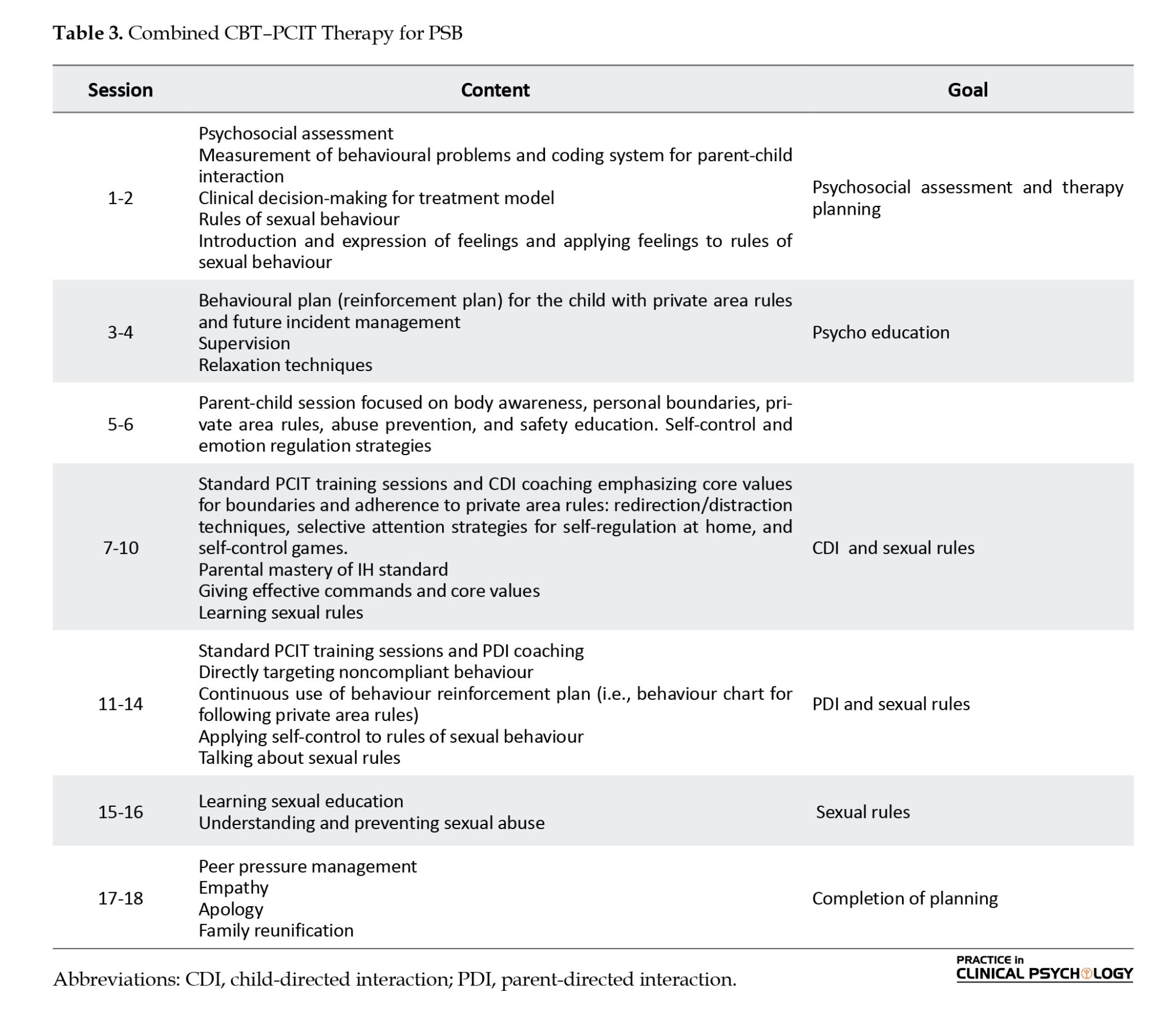
Type of Study: Original Research Article |
Subject:
Family and group therapy
Received: 2025/09/3 | Accepted: 2025/12/13 | Published: 2026/04/27
Received: 2025/09/3 | Accepted: 2025/12/13 | Published: 2026/04/27
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
