

Volume 14, Issue 2 (Spring 2026)
PCP 2026, 14(2): 103-112 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mahmoudi M, Loni E, AkbarFahimi N, Mahmoudi M. A Scoping Review of Cognitive Impairment in Adults With Spinal Cord Injury: Mechanisms and Assessment Tools. PCP 2026; 14 (2) :103-112
URL: http://jpcp.uswr.ac.ir/article-1-1045-en.html
URL: http://jpcp.uswr.ac.ir/article-1-1045-en.html



1- Department of Occupational Therapy, School of Rehabilitation, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Clinical Sciences, Clinical Research Development Center, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Occupational Therapy, School of Rehabilitation, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,fahimi1970@yahoo.com
4- Young Researchers and Elite Club, Islamic Azad University, Semnan, Iran.
2- Department of Clinical Sciences, Clinical Research Development Center, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Occupational Therapy, School of Rehabilitation, Rofeideh Rehabilitation Hospital, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
4- Young Researchers and Elite Club, Islamic Azad University, Semnan, Iran.
Keywords: Spinal cord injury (SCI), Adult, Cognitive impairment, Cognitive domains, Evaluation, Assessment, Cognitive dysfunction, Neuropsychological assessment, Scoping review, Rehabilitation
Full-Text [PDF 661 kb]
(97 Downloads)
| Abstract (HTML) (884 Views)
Full-Text: (144 Views)
Introduction
Spinal cord injury (SCI) is a devastating neurological condition resulting from traumatic or non-traumatic damage that causes bruising, compression, or disruption of neural tissue (Chay et al., 2020; Craig et al., 2017). Globally, SCI imposes a significant burden: in the United States, approximately 54 new cases per million occur annually (~17,900 cases/year) (Furlan et al., 2013), while in Iran, the prevalence is estimated at 318 per million (Jazayeri et al., 2015). Beyond its physical consequences (such as motor impairment, sensory loss, and autonomic dysfunction below the injury level), SCI is increasingly recognized as a condition with substantial cognitive sequelae (Craig et al., 2015). Emerging evidence indicates that adults with SCI (awSCI) face up to a 13-fold higher risk of cognitive impairment compared to the general population (Molina et al., 2018; Sachdeva et al., 2018), even in the absence of concomitant traumatic brain injury (TBI). Cognitive deficits in awSCI can profoundly affect daily functioning, reduce independence, and increase the risk of rehospitalization (Craig et al., 2017; Chiaravalloti et al., 2020a; Chiaravalloti et al., 2020b). Reported prevalence rates of cognitive impairment in this population vary widely—from 10% to 60%, with some studies citing rates as high as 80% (likely reflecting heterogeneity in assessment methods, sample characteristics, and definitions of impairment) (Craig et al., 2017; Chiaravalloti et al., 2020a; Chiaravalloti et al., 2020b).
Critically, however, the underlying mechanisms of cognitive dysfunction following pure SCI (i.e. without TBI or other central nervous system [CNS] insults) remain poorly understood. Moreover, it is unclear which specific cognitive domains (e.g. attention, executive function, memory, processing speed) are most consistently affected, and which assessment tools are most appropriate for detecting these deficits in awSCI. Given these uncertainties, there is a pressing need to map and synthesize the existing evidence on cognitive impairment after pure SCI. A scoping review is the optimal methodological approach for this purpose, as it allows for broad exploration of a heterogeneous and evolving evidence base, identification of key concepts, and clarification of gaps in the literature (Arksey & O’malley, 2005). Unlike a systematic review, which seeks to answer a narrowly defined clinical question with rigorous quality appraisal, a scoping review is designed to chart the scope and nature of research activity, particularly in areas where evidence is fragmented or conceptual clarity is lacking (Arksey & O’malley, 2005). This approach aligns with the Preferred Reporting Items for Systematic Reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) framework, which emphasizes transparency in mapping existing knowledge and informing future research priorities (Tricco et al., 2018).
What is the reported prevalence of cognitive impairment in adults with pure SCI (i.e. no history of TBI or other brain injury)?
Which cognitive domains are most frequently and significantly affected? What assessment tools or neuropsychological batteries have been used to detect cognitive impairment in this population?
Pediatric populations were excluded due to the dynamic nature of neurocognitive development during childhood and adolescence, which may confound the interpretation of cognitive test results and limit comparability across studies. By systematically mapping the current evidence, this review seeks to inform clinical practice, guide rehabilitation strategies, and highlight priorities for future research in cognitive outcomes after SCI.
Materials and Methods
This study adopted the scoping review methodology proposed by Arksey and O’Malley (2005), which involves a five-stage framework:
1) defining the research question, 2) identifying relevant studies through electronic databases, 3) establishing inclusion and exclusion criteria, 4) charting and synthesizing data using a narrative approach, and 5) summarizing and reporting the findings.
Stage 1: Identifying the research question
This review aimed to explore the following key questions:
What is the reported prevalence of cognitive impairment among adults with pure SCI, excluding those with TBI or other cerebral lesions? Which cognitive domains are most consistently and significantly affected in this population? What assessment tools or neuropsychological batteries have been applied to evaluate cognitive impairment in adults with pure SCI?
Stage 2: Identifying relevant studies
A comprehensive search was conducted in major electronic databases (MEDLINE, ScienceDirect, OTseeker, and PEDro) chosen for their broad coverage of peer-reviewed literature in psychology, neuroscience, and rehabilitation. Additional sources, such as Google Scholar, clinical guidelines, theses, and conference proceedings, were also reviewed to capture potentially relevant studies.
The search strategy combined both keywords and MeSH terms, including SCI, pure SCI, adult, cognitive impairment, cognitive dysfunction, memory impairment, attention deficit, executive function, neuropsychological assessment, and evaluation, connected through appropriate Boolean operators.
Stage 3: Study selection
The inclusion criteria included peer-reviewed, full-text articles published in English or Persian between January 2013 and January 2024, involving adults with pure SCI and no history of TBI or other cerebral involvement. Studies were excluded if they involved animal models, targeted non-SCI populations or those with co-morbid neurological conditions, participants under 18 years of age, lacked clear cognitive definitions or measures, or were case reports or editorials without empirical data.
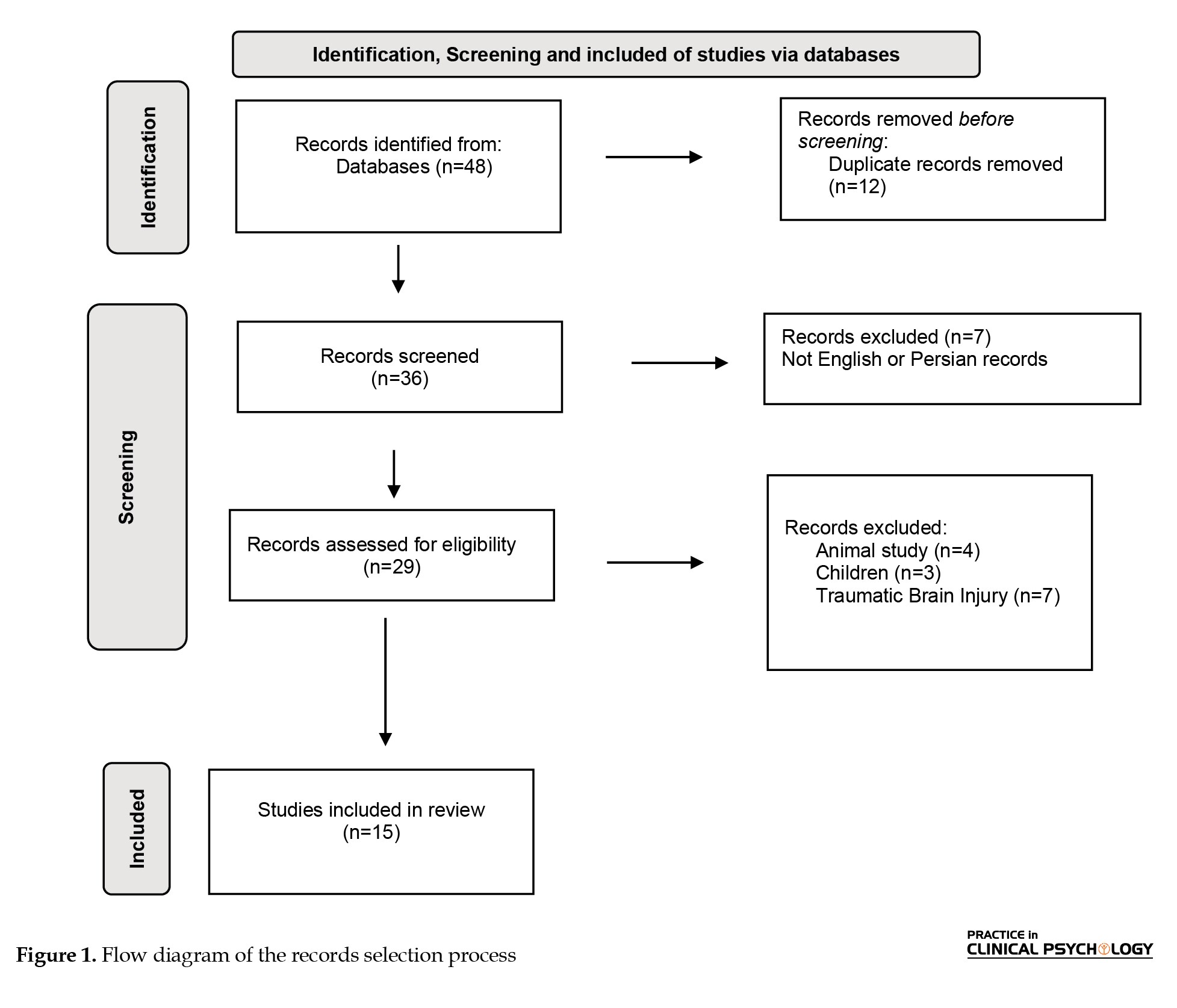
After database searching and manual screening, 48 articles were imported into EndNote. Following the removal of 12 duplicates, 36 titles and abstracts were independently reviewed by two authors. A total of 21 articles were excluded for the following reasons: seven studies were published in languages other than English or Persian; four were animal studies; three focused on pediatric populations; and seven investigated SCI or TBI. Ultimately, 15 studies met all inclusion criteria. Any discrepancies between the two reviewers were resolved through discussion with a third independent author. Figure 1 shows the study selection process.
Stage 4: Charting the data
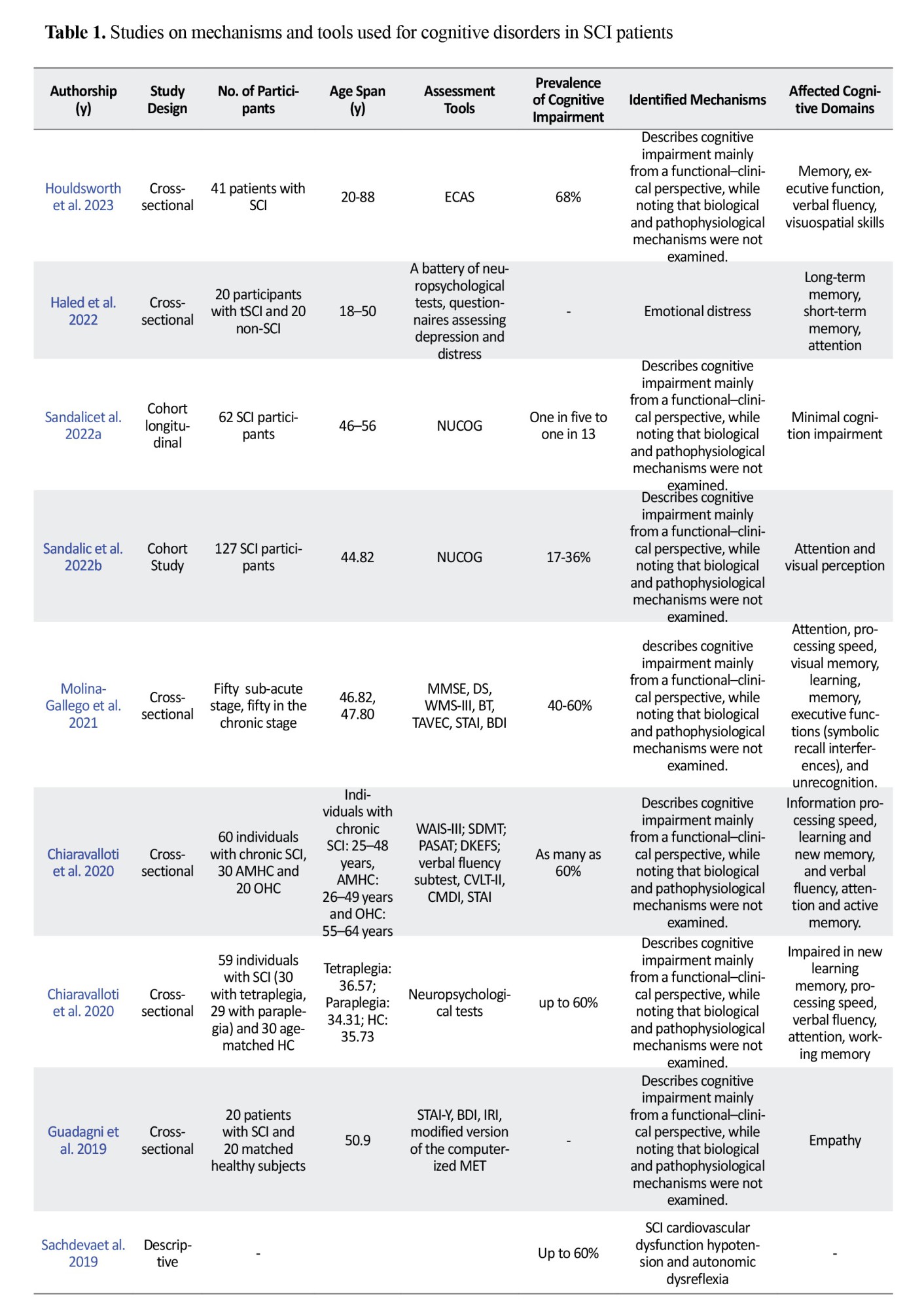
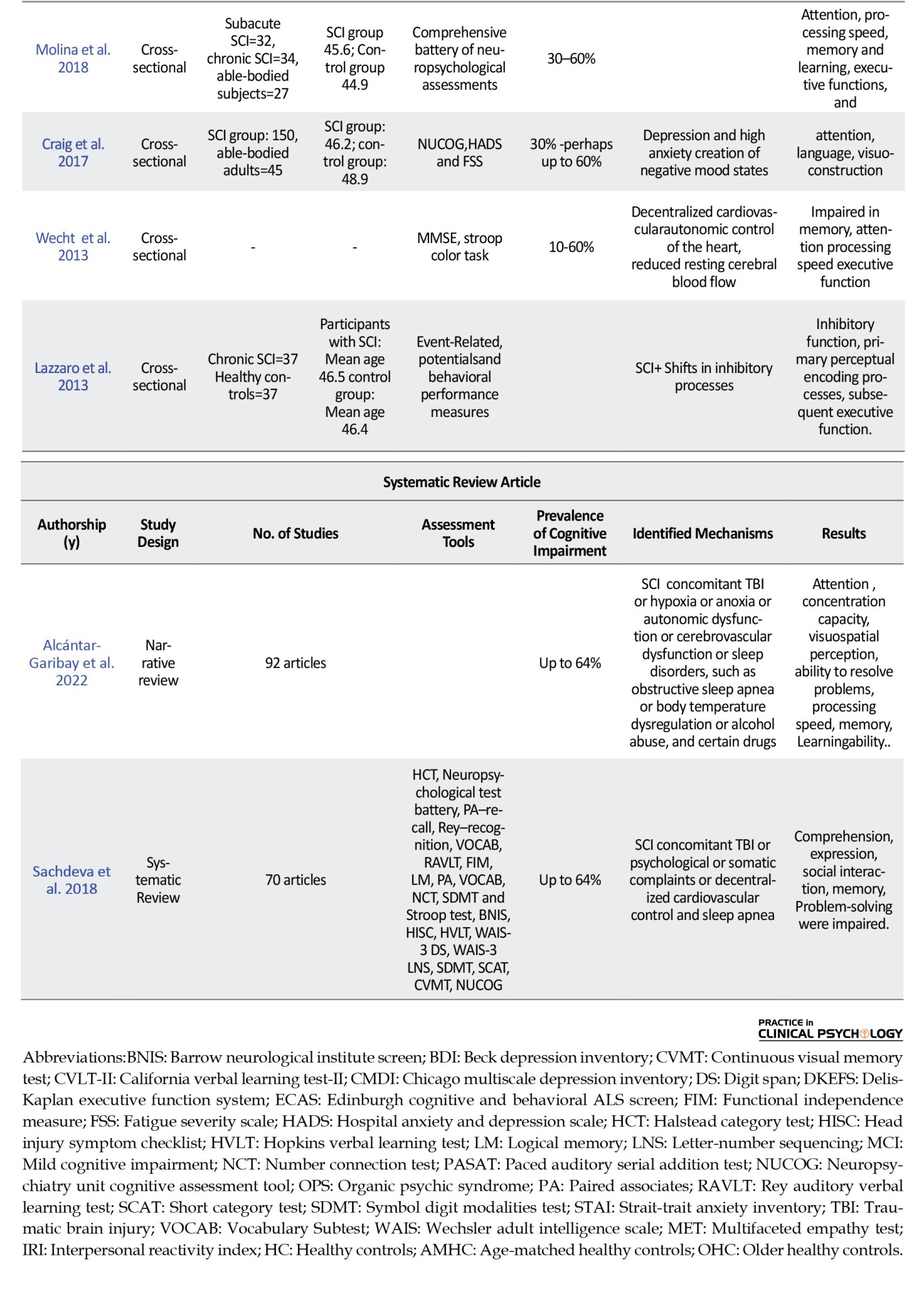
Data were extracted using Microsoft Excel. Table 1 presents a synthesis of key information from the 15 included studies, such as authorship, publication year, participant characteristics, study design, prevalence of cognitive impairment, identified mechanisms, assessment tools, and the affected cognitive domains.
Stage 5: Collating, summarizing, and reporting results
The extracted findings were systematically organized into thematic categories that directly correspond to the research objectives. A narrative synthesis approach was employed to integrate and interpret the results, with thematic priorities established based on their salience and alignment with the study’s guiding research questions.
The protocol of this study was not registered in PROSPERO or any other databases.
Result
This process led to the identification of 48 articles. All findings were transferred to the EndNote software, and duplicates were eliminated (n=36). Two authors reviewed the abstracts of these 36 articles and removing 7 articles due to did not meet inclusion criteria (n=29). After checking the full text, the 14 articles were excluded (Figure 1). Finally 15 articles: A total of 10 cross-sectional studies, one descriptive study, a cohort study, a longitudinal cohort study (771 participants in total), a narrative review study and a systematic review study, were included to this review (Table 1). The first author name, type of study, number of participant and participant age or number of studies which reviewed, prevalence and mechanism of cognitive impairment, type of assessment and cognitive impairment domains were extracted from articles. According to the guidelines for a scoping review, the quality of studies did not appraise.
Discussion
Cognitive impairment after SCI is increasingly recognized as a multifaceted condition, though its underlying mechanisms remain incompletely understood. Current evidence suggests that cognitive difficulties may arise from the interplay of neurological, cardiovascular, and psychosocial factors. However, most supporting data derive from cross-sectional or observational studies, limiting causal inference. Therefore, the relationships described below should be interpreted as associations or potential contributors rather than established causal pathways.
Potential contributing factors
CNS dysfunction
Individuals with SCI may exhibit cognitive deficits linked to CNS alterations, including subclinical brain injury, hypoxia secondary to respiratory compromise, autonomic dysregulation, sleep disturbances, or impaired thermoregulation (Heled et al., 2022.; Alcántar-Garib et al., 2022). Neurochemical shifts (particularly reduced dopaminergic activity) have been associated with impairments in object recognition and spatial memory in preclinical models (Kheyrkhah et al., 2020). Additionally, functional and structural changes in brain networks involved in pain processing and neural excitation/inhibition balance may indirectly influence cognition (Lazzaro et al., 2013; Wu et al., 2014). While these findings are biologically plausible, longitudinal and mechanistic studies are needed to confirm their clinical relevance in human SCI populations.
Cardiovascular alterations
Systemic blood pressure instability and reduced vascular compliance (common after high-level cervical or upper thoracic SCI) may compromise cerebral perfusion, potentially contributing to cognitive changes (Sachdeva et al., 2019; Wecht & Bauman, 2013). Although individuals with lower-level injuries may experience more subtle cardiovascular dysregulation, the long-term cognitive implications remain uncertain. Importantly, the available evidence is predominantly correlational; therefore, cardiovascular factors should be considered potential modulators rather than definitive causes of post-SCI cognitive impairment.
Psychosocial and behavioral influences
Psychological and social stressors following SCI, including depression, anxiety, reduced resilience, and disruptions in employment or social roles, are frequently reported (Wu et al., 2014; Budd et al., 2022). Maladaptive coping strategies, such as substance use, appear to exacerbate cognitive difficulties, particularly during the critical first six months of community reintegration (Craig et al., 2017). These associations highlight the importance of integrated biopsychosocial models in understanding cognitive outcomes, though directionality remains unclear (e.g. whether cognitive decline predisposes individuals to poorer coping or vice versa).
Cognitive domains affected and assessment approaches A range of cognitive domains are reported as vulnerable after SCI, including attention, memory, executive function, processing speed, visuospatial/visuoconstructional abilities, language, learning, and problem-solving. Notably, deficits in attention and processing speed are the most consistently reported across studies (10 and 9 out of 15, respectively), whereas problem-solving impairments were documented in only one study.
This variability may reflect methodological differences in assessment sensitivity. for instance, instruments, such as the symbol digit modalities test (SDMT) and paced auditory serial addition test (PASAT), commonly used to evaluate processing speed are highly sensitive to subtle cognitive slowing and are frequently included in SCI research protocols. In contrast, higher-order functions, such as problem-solving, are less routinely assessed and may require more complex, ecologically valid tasks that are not consistently applied across studies.
Lazzaro et al. (2013) observed impairments in inhibitory control, early perceptual processing, and executive functions (e.g. contextual manipulation and working memory updating), yet found no significant associations between cognitive performance and injury level, completeness, or chronicity. This underscores the limited predictive value of traditional lesion characteristics and suggests that individual differences, such as premorbid cognitive reserve, comorbidities, or psychosocial context, may play a more substantial role than previously acknowledged.
Commonly used assessment tools include: Memory disorders occur when damage to certain parts of the brain prevents or reduces the ability to store, retain, or remember memories, which were reported in 11 of the 15 studies reviewed. The digit span, rey auditory verbal learning test (Rey AVLT), neuropsychiatry unit cognitive assessment tool (NUCOG), Wechsler Intelligence Scale-III (WAIS-III), mini-mental state examination (MMSE), and visual memory test (BMT) can evaluate different types of memory impairment following SCI (Craig et al., 2017; Molina et al., 2018; Chiaravalloti et al., 2020a; Houldsworth et al., 2023; Molina-Gallego et al. 2021; Wecht & Bauman, 2013). Deficits attention disorders are marked by an ongoing pattern of inattention that interferes with functioning, which was reported in 10 of the 15 studies reviewed. The Digit Span, Stroop Test, NUCOG, and WAIS-III tests are particularly useful in assessing attentional deficits in patients with SCI (Craig et al., 2017; Molina et al., 2018; Chiaravalloti et al., 2020a; Heled et al., 2022; Molina-Gallegoe t al. 2021).
Executive function impairment disrupts a person’s ability to manage their own thoughts, emotions and actions, which were reported in 10 of the 15 studies reviewed. The NUCOG, the verbal fluency subtest of the Delis-Kaplan executive function system (D-KEFS) and the verbal learning test spain-complutense (TAVEC) are common tools for detecting executive function in patients with SCI (Craig et al., 2017; Molina et al., 2018; Chiaravalloti et al., 2020a; Houldsworth et al., 2023; Molina-Gallego et al., 2021).
Processing speed is the time it takes people to receive, understand and respond to information, which was reported in 9 of the 15 studies reviewed. The stroop test, SDMT, and the PASAT are widely utilized in clinical setting to determining deficits in processing speed (Molina et al., 2018; Chiaravalloti et al., 2020b; Heled et al., 2022; Molina-Gallego et al., 2021).
Language disorders are difficulties in communicating one’s meaning through speech, writing, or even gesture, which were reported in 7 of the 15 studies reviewed. The edinburgh cognitive and behavioral ALS Screen (ECAS), NUCOG, MMSE, and Kavé naming test can help assess language disorders after SCI (Craig et al., 2017; Sachdeva et al., 2018; Heled et al., 2022; Molina-Gallego et al. 2021; Wecht & Bauman, 2013).
Visuo-spatial and visuo-constructional disorders are an inability to see an object or image as a collection of parts and then make a copy of the original from these parts, which was reported in 5 of the 15 studies reviewed. Most of the studies suggested using ECAS, NUCOG, and Rey–recognition tests to check visuospatial disorders in these individuals (Craig et al., 2017; Sachdeva et al., 2018; Houldsworth et al., 2023; Sandalic et al., 2022a; Sandalic et al., 2022b).
Learning disorders are the inability to master reading, spelling, writing, or math skills at or near the expected age and grade level, which were reported in 5 of the 15 studies reviewed. Learning disorders are evaluated using the verbal learning test spain-complutense (TAVEC) and the short category test (SCAT) (Molina et al., 2018; Chiaravalloti et al., 2020a; Molina-Gallegoet al. 2021).
Problem-solving disorder was reported in 1 out of 15 articles, which suggested using SCAT and the halstead category test (HCT) test to assessing this problem (Sachdeva et al., 2018). The heterogeneity of instruments complicates cross-study comparisons and may contribute to inconsistent prevalence estimates across domains.
Knowledge gaps and future perspectives
Several critical gaps warrant attention
Longitudinal studies are needed to track cognitive trajectories from acute to chronic phases post-SCI and to clarify temporal relationships between physiological changes (e.g. autonomic dysfunction, cerebral hypoperfusion) and cognitive outcomes. Standardized, SCI-validated cognitive screening tools should be developed and implemented to improve detection, comparability, and clinical utility. Mechanistic investigations, particularly those integrating neuroimaging, autonomic monitoring, and cerebrovascular assessments, are essential to elucidate how SCI-related physiological disruptions affect brain function. Intervention trials targeting modifiable factors (e.g. cardiovascular stability, depression, sleep quality) could inform preventive or rehabilitative strategies. Ecologically valid assessments of higher-order cognitive functions (e.g. problem-solving, real-world executive functioning) are underutilized and should be prioritized.
Conclusion
Cognitive impairment after SCI is a multidimensional phenomenon influenced by an interplay of neurological, cardiovascular, and psychosocial factors. While associations are increasingly documented, causal pathways remain speculative due to methodological constraints in the current evidence base. However, there is no specialized tool to accurately screen or detect the cognitive impairment after SCI, but ECAS, NUCOG, WAIS-III, MMSE, the Stroop test, and the BDI are the most commonly used tools. Future research must prioritize longitudinal designs, standardized assessments, and mechanistic studies to translate these insights into effective clinical interventions that enhance cognitive and functional outcomes for adults with SCI.
Limitations of the current evidence base
This synthesis is constrained by several methodological limitations in the existing literature. Most studies employ small, heterogeneous samples, limiting statistical power and generalizability. Inconsistent reporting of injury characteristics (e.g. level, completeness, time since injury) hinders subgroup analyses. Diverse assessment tools with varying psychometric properties reduce comparability across studies. The predominantly cross-sectional design of available research precludes causal inference. Language restrictions and publication bias may have excluded relevant non-English or negative findings. The absence of formal critical appraisal of study quality in many reviews further limits confidence in aggregated conclusions.
Ethical Considerations
Compliance with ethical guidelines
This article is a review study with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Nazila Akbarfahimi, Elham Loni; Data collection: Mahyar Mahmoudi; Data analysis and interpretation of results: Mahyar Mahmoudi, Elham Loni; Draft manuscript preparation: Mahyar Mahmoudi, Elham Loni, Nazila Akbarfahimi, and Mohammadmasoud Mahmoudi; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank the Clinical Research Development Center of Rofeideh Rehabilitation Hospital, Tehran Province, Iran, for their continued support throughout this study.
References
Spinal cord injury (SCI) is a devastating neurological condition resulting from traumatic or non-traumatic damage that causes bruising, compression, or disruption of neural tissue (Chay et al., 2020; Craig et al., 2017). Globally, SCI imposes a significant burden: in the United States, approximately 54 new cases per million occur annually (~17,900 cases/year) (Furlan et al., 2013), while in Iran, the prevalence is estimated at 318 per million (Jazayeri et al., 2015). Beyond its physical consequences (such as motor impairment, sensory loss, and autonomic dysfunction below the injury level), SCI is increasingly recognized as a condition with substantial cognitive sequelae (Craig et al., 2015). Emerging evidence indicates that adults with SCI (awSCI) face up to a 13-fold higher risk of cognitive impairment compared to the general population (Molina et al., 2018; Sachdeva et al., 2018), even in the absence of concomitant traumatic brain injury (TBI). Cognitive deficits in awSCI can profoundly affect daily functioning, reduce independence, and increase the risk of rehospitalization (Craig et al., 2017; Chiaravalloti et al., 2020a; Chiaravalloti et al., 2020b). Reported prevalence rates of cognitive impairment in this population vary widely—from 10% to 60%, with some studies citing rates as high as 80% (likely reflecting heterogeneity in assessment methods, sample characteristics, and definitions of impairment) (Craig et al., 2017; Chiaravalloti et al., 2020a; Chiaravalloti et al., 2020b).
Critically, however, the underlying mechanisms of cognitive dysfunction following pure SCI (i.e. without TBI or other central nervous system [CNS] insults) remain poorly understood. Moreover, it is unclear which specific cognitive domains (e.g. attention, executive function, memory, processing speed) are most consistently affected, and which assessment tools are most appropriate for detecting these deficits in awSCI. Given these uncertainties, there is a pressing need to map and synthesize the existing evidence on cognitive impairment after pure SCI. A scoping review is the optimal methodological approach for this purpose, as it allows for broad exploration of a heterogeneous and evolving evidence base, identification of key concepts, and clarification of gaps in the literature (Arksey & O’malley, 2005). Unlike a systematic review, which seeks to answer a narrowly defined clinical question with rigorous quality appraisal, a scoping review is designed to chart the scope and nature of research activity, particularly in areas where evidence is fragmented or conceptual clarity is lacking (Arksey & O’malley, 2005). This approach aligns with the Preferred Reporting Items for Systematic Reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) framework, which emphasizes transparency in mapping existing knowledge and informing future research priorities (Tricco et al., 2018).
What is the reported prevalence of cognitive impairment in adults with pure SCI (i.e. no history of TBI or other brain injury)?
Which cognitive domains are most frequently and significantly affected? What assessment tools or neuropsychological batteries have been used to detect cognitive impairment in this population?
Pediatric populations were excluded due to the dynamic nature of neurocognitive development during childhood and adolescence, which may confound the interpretation of cognitive test results and limit comparability across studies. By systematically mapping the current evidence, this review seeks to inform clinical practice, guide rehabilitation strategies, and highlight priorities for future research in cognitive outcomes after SCI.
Materials and Methods
This study adopted the scoping review methodology proposed by Arksey and O’Malley (2005), which involves a five-stage framework:
1) defining the research question, 2) identifying relevant studies through electronic databases, 3) establishing inclusion and exclusion criteria, 4) charting and synthesizing data using a narrative approach, and 5) summarizing and reporting the findings.
Stage 1: Identifying the research question
This review aimed to explore the following key questions:
What is the reported prevalence of cognitive impairment among adults with pure SCI, excluding those with TBI or other cerebral lesions? Which cognitive domains are most consistently and significantly affected in this population? What assessment tools or neuropsychological batteries have been applied to evaluate cognitive impairment in adults with pure SCI?
Stage 2: Identifying relevant studies
A comprehensive search was conducted in major electronic databases (MEDLINE, ScienceDirect, OTseeker, and PEDro) chosen for their broad coverage of peer-reviewed literature in psychology, neuroscience, and rehabilitation. Additional sources, such as Google Scholar, clinical guidelines, theses, and conference proceedings, were also reviewed to capture potentially relevant studies.
The search strategy combined both keywords and MeSH terms, including SCI, pure SCI, adult, cognitive impairment, cognitive dysfunction, memory impairment, attention deficit, executive function, neuropsychological assessment, and evaluation, connected through appropriate Boolean operators.
Stage 3: Study selection
The inclusion criteria included peer-reviewed, full-text articles published in English or Persian between January 2013 and January 2024, involving adults with pure SCI and no history of TBI or other cerebral involvement. Studies were excluded if they involved animal models, targeted non-SCI populations or those with co-morbid neurological conditions, participants under 18 years of age, lacked clear cognitive definitions or measures, or were case reports or editorials without empirical data.
After database searching and manual screening, 48 articles were imported into EndNote. Following the removal of 12 duplicates, 36 titles and abstracts were independently reviewed by two authors. A total of 21 articles were excluded for the following reasons: seven studies were published in languages other than English or Persian; four were animal studies; three focused on pediatric populations; and seven investigated SCI or TBI. Ultimately, 15 studies met all inclusion criteria. Any discrepancies between the two reviewers were resolved through discussion with a third independent author. Figure 1 shows the study selection process.
Stage 4: Charting the data
Data were extracted using Microsoft Excel. Table 1 presents a synthesis of key information from the 15 included studies, such as authorship, publication year, participant characteristics, study design, prevalence of cognitive impairment, identified mechanisms, assessment tools, and the affected cognitive domains.
Stage 5: Collating, summarizing, and reporting results
The extracted findings were systematically organized into thematic categories that directly correspond to the research objectives. A narrative synthesis approach was employed to integrate and interpret the results, with thematic priorities established based on their salience and alignment with the study’s guiding research questions.
The protocol of this study was not registered in PROSPERO or any other databases.
Result
This process led to the identification of 48 articles. All findings were transferred to the EndNote software, and duplicates were eliminated (n=36). Two authors reviewed the abstracts of these 36 articles and removing 7 articles due to did not meet inclusion criteria (n=29). After checking the full text, the 14 articles were excluded (Figure 1). Finally 15 articles: A total of 10 cross-sectional studies, one descriptive study, a cohort study, a longitudinal cohort study (771 participants in total), a narrative review study and a systematic review study, were included to this review (Table 1). The first author name, type of study, number of participant and participant age or number of studies which reviewed, prevalence and mechanism of cognitive impairment, type of assessment and cognitive impairment domains were extracted from articles. According to the guidelines for a scoping review, the quality of studies did not appraise.
Discussion
Cognitive impairment after SCI is increasingly recognized as a multifaceted condition, though its underlying mechanisms remain incompletely understood. Current evidence suggests that cognitive difficulties may arise from the interplay of neurological, cardiovascular, and psychosocial factors. However, most supporting data derive from cross-sectional or observational studies, limiting causal inference. Therefore, the relationships described below should be interpreted as associations or potential contributors rather than established causal pathways.
Potential contributing factors
CNS dysfunction
Individuals with SCI may exhibit cognitive deficits linked to CNS alterations, including subclinical brain injury, hypoxia secondary to respiratory compromise, autonomic dysregulation, sleep disturbances, or impaired thermoregulation (Heled et al., 2022.; Alcántar-Garib et al., 2022). Neurochemical shifts (particularly reduced dopaminergic activity) have been associated with impairments in object recognition and spatial memory in preclinical models (Kheyrkhah et al., 2020). Additionally, functional and structural changes in brain networks involved in pain processing and neural excitation/inhibition balance may indirectly influence cognition (Lazzaro et al., 2013; Wu et al., 2014). While these findings are biologically plausible, longitudinal and mechanistic studies are needed to confirm their clinical relevance in human SCI populations.
Cardiovascular alterations
Systemic blood pressure instability and reduced vascular compliance (common after high-level cervical or upper thoracic SCI) may compromise cerebral perfusion, potentially contributing to cognitive changes (Sachdeva et al., 2019; Wecht & Bauman, 2013). Although individuals with lower-level injuries may experience more subtle cardiovascular dysregulation, the long-term cognitive implications remain uncertain. Importantly, the available evidence is predominantly correlational; therefore, cardiovascular factors should be considered potential modulators rather than definitive causes of post-SCI cognitive impairment.
Psychosocial and behavioral influences
Psychological and social stressors following SCI, including depression, anxiety, reduced resilience, and disruptions in employment or social roles, are frequently reported (Wu et al., 2014; Budd et al., 2022). Maladaptive coping strategies, such as substance use, appear to exacerbate cognitive difficulties, particularly during the critical first six months of community reintegration (Craig et al., 2017). These associations highlight the importance of integrated biopsychosocial models in understanding cognitive outcomes, though directionality remains unclear (e.g. whether cognitive decline predisposes individuals to poorer coping or vice versa).
Cognitive domains affected and assessment approaches A range of cognitive domains are reported as vulnerable after SCI, including attention, memory, executive function, processing speed, visuospatial/visuoconstructional abilities, language, learning, and problem-solving. Notably, deficits in attention and processing speed are the most consistently reported across studies (10 and 9 out of 15, respectively), whereas problem-solving impairments were documented in only one study.
This variability may reflect methodological differences in assessment sensitivity. for instance, instruments, such as the symbol digit modalities test (SDMT) and paced auditory serial addition test (PASAT), commonly used to evaluate processing speed are highly sensitive to subtle cognitive slowing and are frequently included in SCI research protocols. In contrast, higher-order functions, such as problem-solving, are less routinely assessed and may require more complex, ecologically valid tasks that are not consistently applied across studies.
Lazzaro et al. (2013) observed impairments in inhibitory control, early perceptual processing, and executive functions (e.g. contextual manipulation and working memory updating), yet found no significant associations between cognitive performance and injury level, completeness, or chronicity. This underscores the limited predictive value of traditional lesion characteristics and suggests that individual differences, such as premorbid cognitive reserve, comorbidities, or psychosocial context, may play a more substantial role than previously acknowledged.
Commonly used assessment tools include: Memory disorders occur when damage to certain parts of the brain prevents or reduces the ability to store, retain, or remember memories, which were reported in 11 of the 15 studies reviewed. The digit span, rey auditory verbal learning test (Rey AVLT), neuropsychiatry unit cognitive assessment tool (NUCOG), Wechsler Intelligence Scale-III (WAIS-III), mini-mental state examination (MMSE), and visual memory test (BMT) can evaluate different types of memory impairment following SCI (Craig et al., 2017; Molina et al., 2018; Chiaravalloti et al., 2020a; Houldsworth et al., 2023; Molina-Gallego et al. 2021; Wecht & Bauman, 2013). Deficits attention disorders are marked by an ongoing pattern of inattention that interferes with functioning, which was reported in 10 of the 15 studies reviewed. The Digit Span, Stroop Test, NUCOG, and WAIS-III tests are particularly useful in assessing attentional deficits in patients with SCI (Craig et al., 2017; Molina et al., 2018; Chiaravalloti et al., 2020a; Heled et al., 2022; Molina-Gallegoe t al. 2021).
Executive function impairment disrupts a person’s ability to manage their own thoughts, emotions and actions, which were reported in 10 of the 15 studies reviewed. The NUCOG, the verbal fluency subtest of the Delis-Kaplan executive function system (D-KEFS) and the verbal learning test spain-complutense (TAVEC) are common tools for detecting executive function in patients with SCI (Craig et al., 2017; Molina et al., 2018; Chiaravalloti et al., 2020a; Houldsworth et al., 2023; Molina-Gallego et al., 2021).
Processing speed is the time it takes people to receive, understand and respond to information, which was reported in 9 of the 15 studies reviewed. The stroop test, SDMT, and the PASAT are widely utilized in clinical setting to determining deficits in processing speed (Molina et al., 2018; Chiaravalloti et al., 2020b; Heled et al., 2022; Molina-Gallego et al., 2021).
Language disorders are difficulties in communicating one’s meaning through speech, writing, or even gesture, which were reported in 7 of the 15 studies reviewed. The edinburgh cognitive and behavioral ALS Screen (ECAS), NUCOG, MMSE, and Kavé naming test can help assess language disorders after SCI (Craig et al., 2017; Sachdeva et al., 2018; Heled et al., 2022; Molina-Gallego et al. 2021; Wecht & Bauman, 2013).
Visuo-spatial and visuo-constructional disorders are an inability to see an object or image as a collection of parts and then make a copy of the original from these parts, which was reported in 5 of the 15 studies reviewed. Most of the studies suggested using ECAS, NUCOG, and Rey–recognition tests to check visuospatial disorders in these individuals (Craig et al., 2017; Sachdeva et al., 2018; Houldsworth et al., 2023; Sandalic et al., 2022a; Sandalic et al., 2022b).
Learning disorders are the inability to master reading, spelling, writing, or math skills at or near the expected age and grade level, which were reported in 5 of the 15 studies reviewed. Learning disorders are evaluated using the verbal learning test spain-complutense (TAVEC) and the short category test (SCAT) (Molina et al., 2018; Chiaravalloti et al., 2020a; Molina-Gallegoet al. 2021).
Problem-solving disorder was reported in 1 out of 15 articles, which suggested using SCAT and the halstead category test (HCT) test to assessing this problem (Sachdeva et al., 2018). The heterogeneity of instruments complicates cross-study comparisons and may contribute to inconsistent prevalence estimates across domains.
Knowledge gaps and future perspectives
Several critical gaps warrant attention
Longitudinal studies are needed to track cognitive trajectories from acute to chronic phases post-SCI and to clarify temporal relationships between physiological changes (e.g. autonomic dysfunction, cerebral hypoperfusion) and cognitive outcomes. Standardized, SCI-validated cognitive screening tools should be developed and implemented to improve detection, comparability, and clinical utility. Mechanistic investigations, particularly those integrating neuroimaging, autonomic monitoring, and cerebrovascular assessments, are essential to elucidate how SCI-related physiological disruptions affect brain function. Intervention trials targeting modifiable factors (e.g. cardiovascular stability, depression, sleep quality) could inform preventive or rehabilitative strategies. Ecologically valid assessments of higher-order cognitive functions (e.g. problem-solving, real-world executive functioning) are underutilized and should be prioritized.
Conclusion
Cognitive impairment after SCI is a multidimensional phenomenon influenced by an interplay of neurological, cardiovascular, and psychosocial factors. While associations are increasingly documented, causal pathways remain speculative due to methodological constraints in the current evidence base. However, there is no specialized tool to accurately screen or detect the cognitive impairment after SCI, but ECAS, NUCOG, WAIS-III, MMSE, the Stroop test, and the BDI are the most commonly used tools. Future research must prioritize longitudinal designs, standardized assessments, and mechanistic studies to translate these insights into effective clinical interventions that enhance cognitive and functional outcomes for adults with SCI.
Limitations of the current evidence base
This synthesis is constrained by several methodological limitations in the existing literature. Most studies employ small, heterogeneous samples, limiting statistical power and generalizability. Inconsistent reporting of injury characteristics (e.g. level, completeness, time since injury) hinders subgroup analyses. Diverse assessment tools with varying psychometric properties reduce comparability across studies. The predominantly cross-sectional design of available research precludes causal inference. Language restrictions and publication bias may have excluded relevant non-English or negative findings. The absence of formal critical appraisal of study quality in many reviews further limits confidence in aggregated conclusions.
Ethical Considerations
Compliance with ethical guidelines
This article is a review study with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Nazila Akbarfahimi, Elham Loni; Data collection: Mahyar Mahmoudi; Data analysis and interpretation of results: Mahyar Mahmoudi, Elham Loni; Draft manuscript preparation: Mahyar Mahmoudi, Elham Loni, Nazila Akbarfahimi, and Mohammadmasoud Mahmoudi; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank the Clinical Research Development Center of Rofeideh Rehabilitation Hospital, Tehran Province, Iran, for their continued support throughout this study.
References
Alcántar-Garibay, O. V., Incontri-Abraham, D., & Ibarra, A. (2022). Spinal cord injury-induced cognitive impairment: A narrative review. Neural Regeneration Research, 17(12), 2649–2654. [DOI:10.4103/1673-5374.339475] [PMID]
Arksey, H., & O'malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19-32. [DOI:10.1080/1364557032000119616]
Chay, W., & Kirshblum, S. (2020). Predicting outcomes after spinal cord injury. Physical Medicine and Rehabilitation Clinics, 31(3), 331-343. [DOI:10.1016/j.pmr.2020.03.003] [PMID]
Chiaravalloti, N. D., Weber, E., Wylie, G., Dyson-Hudson, T., & Wecht, J. M. (2020a). Patterns of cognitive deficits in persons with spinal cord injury as compared with both age-matched and older individuals without spinal cord injury. The Journal of Spinal Cord Medicine, 43(1), 88-97. [DOI:10.1080/10790268.2018.1543103] [PMID]
Chiaravalloti, N. D., Weber, E., Wylie, G., Dyson-Hudson, T., & Wecht, J. M. (2020b). The impact of level of injury on patterns of cognitive dysfunction in individuals with spinal cord injury. The Journal of Spinal Cord Medicine, 43(5), 633-641. [DOI:10.1080/10790268.2019.1696076] [PMID]
Craig, A., Guest, R., Tran, Y., & Middleton, J. (2017). Cognitive impairment and mood states after spinal cord injury. Journal of Neurotrauma, 34(6), 1156-1163. [DOI:10.1089/neu.2016.4632] [PMID]
Craig, A., Perry, K. N., Guest, R., Tran, Y., Dezarnaulds, A., & Hales, A., et al. (2015). Prospective study of the occurrence of psychological disorders and comorbidities after spinal cord injury. Archives of Physical Medicine and Rehabilitation, 96(8), 1426-1434. [DOI:10.1016/j.apmr.2015.02.027] [PMID]
Furlan, J. C., Sakakibara, B. M., Miller, W. C., & Krassioukov, A. V. (2013). Global incidence and prevalence of traumatic spinal cord injury. Canadian Journal of Neurological Sciences, 40(4), 456-464. [DOI:10.1017/S0317167100014530] [PMID]
Guadagni, V., Sarà, M., Conson, M., Carolei, A., Sacco, S., & Vadini, S., et al. (2019). Cognitive and emotional empathy in individuals with spinal cord injury. Behavioural Neurology, 2019(1), 1312934. [DOI:10.1155/2019/1312934] [PMID]
Heled, E., Tal, K., & Zeilig, G. (2022). Does lack of brain injury mean lack of cognitive impairment in traumatic spinal cord injury?. The Journal of Spinal Cord Medicine, 45(3), 373-380. [DOI:10.1080/10790268.2020.1847564] [PMID]
Houldsworth, C., Nair, K. P. S., & Hariharan, R. P. (2023). Cognition and quality of life of people with spinal cord injury. Progress in Rehabilitation Medicine, 8, 20230001. [DOI:10.2490/prm.20230001] [PMID]
Jazayeri, S. B., Ataeepour, M., Rabiee, H., Motevalian, S. A., Saadat, S., & Vaccaro, A. R., et al. (2015). Prevalence of spinal cord injury in Iran: A 3-source capture-recapture study. Neuroepidemiology, 45(1), 28-33. [DOI:10.1159/000435785] [PMID]
Kheyrkhah, H., Soltani Zangbar, H., Salimi, O., Shahabi, P., & Alaei, H. (2020). Prefrontal dopaminergic system and its role in working memory and cognition in spinal cord-injured rats. Experimental Physiology, 105(9), 1579-1587. [DOI:10.1113/EP088537] [PMID]
Lazzaro, I., Tran, Y., Wijesuriya, N., & Craig, A. (2013). Central correlates of impaired information processing in people with spinal cord injury. Journal of Clinical Neurophysiology, 30(1), 59-65. [DOI:10.1097/WNP.0b013e31827edb0c] [PMID]
Molina-Gallego, B., Gómez-Cantarino, S., Ugarte-Gurrutxaga, M. I., Molina-Gallego, L., & Mordillo-Mateos, L. (2021). Neuropsychological study in patients with spinal cord injuries. Healthcare, 9(3), 241. [DOI:10.3390/healthcare9030241]
Molina, B., Segura, A., Serrano, J. P., Alonso, F. J., Molina, L., & Pérez-Borrego, Y. A., et al. (2018). Cognitive performance of people with traumatic spinal cord injury: A cross-sectional study comparing people with subacute and chronic injuries. Spinal Cord, 56(8), 796-805. [DOI:10.1038/s41393-018-0076-0] [PMID]
Sachdeva, R., Gao, F., Chan, C. C., & Krassioukov, A. V. (2018). Cognitive function after spinal cord injury: A systematic review. Neurology, 91(13), 611-621 [DOI:10.1212/WNL.0000000000006244] [PMID]
Sandalic, D., Tran, Y., Arora, M., Middleton, J., McBain, C., & Myles, D., et al. (2022). Improving assessment of cognitive impairment after spinal cord injury: Methods to reduce the risk of reporting false positives. Journal of Clinical Medicine, 12(1), 68. [DOI:10.3390/jcm12010068]
Sandalic, D., Tran, Y., Craig, A., Arora, M., Pozzato, I., & Simpson, G., et al. (2022). The need for a specialized neurocognitive screen and consistent cognitive impairment criteria in spinal cord injury: analysis of the suitability of the neuropsychiatry unit cognitive assessment tool. Journal of Clinical Medicine, 11(12), 3344. [DOI:10.3390/jcm11123344] [PMID]
Sachdeva, R., Nightingale, T. E., & Krassioukov, A. V. (2019). The blood pressure pendulum following spinal cord injury: implications for vascular cognitive impairment. International Journal of Molecular Sciences, 20(10), 2464. [DOI:10.3390/ijms20102464] [PMID]
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., & Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of Internal Medicine, 169(7), 467-473. [DOI:10.7326/M18-0850] [PMID]
Wecht, J. M., & Bauman, W. A. (2013). Decentralized cardiovascular autonomic control and cognitive deficits in persons with spinal cord injury. The Journal of Spinal Cord Medicine, 36(2), 74-81. [DOI:10.1179/2045772312Y.0000000056] [PMID]
Wu, J., Zhao, Z., Sabirzhanov, B., Stoica, B. A., Kumar, A., & Luo, T., et al. (2014). Spinal cord injury causes brain inflammation associated with cognitive and affective changes: Role of cell cycle pathways. Journal of Neuroscience, 34(33), 10989-11006. [DOI:10.1523/JNEUROSCI.5110-13.2014] [PMID]
Type of Study: Review paper |
Subject:
Rehabilitation
Received: 2025/08/23 | Accepted: 2025/11/2 | Published: 2026/04/27
Received: 2025/08/23 | Accepted: 2025/11/2 | Published: 2026/04/27
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
