

Volume 14, Issue 2 (Spring 2026)
PCP 2026, 14(2): 175-184 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Akbari E, Heydarinasab L, Yaghoubi H, Farahani H. Childhood Abuse and Mentalization Among Students with Different Levels of Suicidal Ideation: A Comparative Study. PCP 2026; 14 (2) :175-184
URL: http://jpcp.uswr.ac.ir/article-1-1059-en.html
URL: http://jpcp.uswr.ac.ir/article-1-1059-en.html



1- Department of Psychology, Faculty of Humanities, Shahed University, Tehran, Iran.
2- Department of Psychology, Faculty of Humanities, Shahed University, Tehran, Iran. ,l.heydaryn@gmail.com
3- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran.
2- Department of Psychology, Faculty of Humanities, Shahed University, Tehran, Iran. ,
3- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran.
Full-Text [PDF 590 kb]
(97 Downloads)
| Abstract (HTML) (888 Views)
Full-Text: (107 Views)
Introduction
Suicidal ideation is a key predictor of suicidal behavior and is influenced by multiple factors, including biological, psychological, social, and familial determinants (Bertule et al., 2021; Serebriakova et al., 2025). Among young people, these factors can increase the likelihood of suicide attempts, highlighting the importance of identifying key risk mechanisms (Afifi et al., 2016). Globally, suicide is a leading cause of mortality among individuals aged 15–29 (World Health Organization, 2025).
Childhood abuse—including emotional, physical, and sexual abuse, as well as emotional and physical neglect—is a well-established risk factor for suicidal ideation and behavior (Angelakis et al., 2020; Berardelli et al., 2022). Evidence suggests that specific abuse subtypes, particularly sexual abuse, may exert a direct effect on suicidal thoughts, whereas other forms may influence ideation indirectly through mediators, such as depression, anxiety, or reduced social support (Huang & Hou, 2023; McRae et al., 2022). Meta-analyses indicate substantial heterogeneity across studies, highlighting the need for more nuanced research to clarify these pathways (Dube et al., 2023; Xie et al., 2024).
Mentalization—the ability to understand one’s own and others’ mental states—plays a critical role in emotion regulation and social cognition (Arabadzhiev & Paunova, 2024; Wagner-Skacel et al., 2022). Deficits in mentalization can impair emotion regulation and social problem-solving, increasing vulnerability to psychological distress and suicidal ideation (Doba et al., 2025; Zohdi et al., 2022; Pompili et al., 2017). Childhood abuse, encompassing emotional, physical, and sexual maltreatment as well as neglect, can profoundly disrupt the development of mentalization—the ability to understand and interpret one’s own and others’ mental states. Early exposure to abusive or neglectful caregiving environments often impairs the formation of secure attachment, limits opportunities for emotional reflection, and fosters distorted self and other representations. These deficits in mentalization hinder emotional regulation and interpersonal understanding, increasing susceptibility to maladaptive coping strategies such as suicidal ideation. Consequently, impaired mentalization serves as a critical psychological mechanism through which childhood abuse contributes to elevated suicide risk in young adults (Yang & Huang, 2024; Wang et al., 2021).
Emerging evidence suggests that childhood abuse and impaired mentalization interact to heighten suicide risk (Weijers et al., 2018; Wagner-Skacel et al., 2022). Students with higher suicidal ideation not only report more adverse childhood experiences but also demonstrate greater difficulties in mentalization (Li et al., 2020; Yang et al., 2025). This interaction underscores the importance of addressing both trauma and reflective functioning in preventive and therapeutic interventions. Future research should employ longitudinal and culturally sensitive designs to further clarify these mechanisms and inform targeted strategies to reduce suicide risk among vulnerable students.
Childhood abuse can have profound effects on a child’s emotional and cognitive development, particularly in shaping the capacity for self-reflection and understanding others. The quality of early caregiving experiences plays a critical role in the development of mentalization—the ability to interpret and understand one’s own and others’ mental states (Arabadzhiev & Paunova, 2024; Fonagy & Target, 1997). When children experience maltreatment instead of sensitive and responsive caregiving, the development of mentalization may be disrupted. Traumatic interactions such as neglect, emotional invalidation, or abuse can impair the child’s ability to regulate emotions and recognize internal psychological states, leading to distorted perceptions of the self and others (Wagner-Skacel et al., 2022; Doba et al., 2025). Consequently, deficits in mentalization may mediate the relationship between childhood abuse and later suicidal ideation by undermining adaptive emotion regulation and social understanding.
Objective
This study aimed to examine the relationship between childhood abuse and mentalization among students exhibiting high versus low levels of suicidal ideation using a comparative approach. Two hypotheses were formulated. The first predicted that students with elevated suicidal ideation would report substantially higher levels of childhood abuse—including emotional, physical, sexual abuse, and neglect—than those with lower suicidal ideation. The second hypothesized that students with higher suicidal ideation would show markedly greater impairments in mentalization compared to their low-risk peers.
Materials and Methods
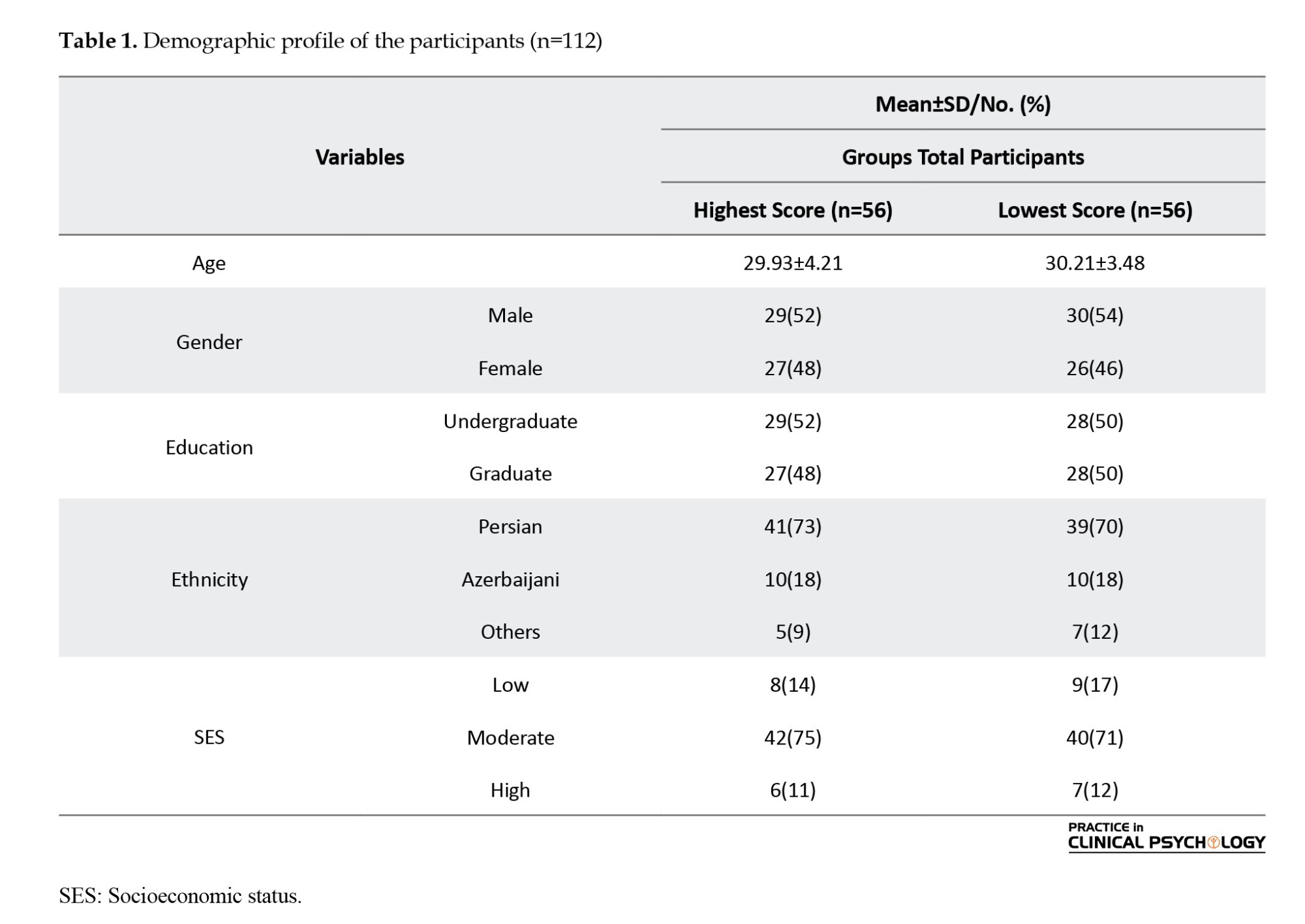
This study employed a descriptive, causal-comparative design. The population comprised all students of Shahed University in Tehran Province, Iran, during the 2024–2025 academic year. The Beck scale for suicide ideation (BSS) (Beck et al., 1979) was distributed to 528 students. In the present study, students scoring above the clinical cutoff (≥9) were organized as the high suicidal ideation group, whereas students scoring at the lower end of the scale (≤3) were classified as the low suicidal ideation group. Based on these scores, 112 students were selected and assigned to two groups: 56 students with the highest scores formed the high suicidal ideation group, and 56 students with the lowest scores formed the low suicidal ideation group (Table 1). Sample size estimation was conducted using G*Power software with the following parameters: medium effect size (d=0.2), 95% confidence level, 80% statistical power, with two groups and two variables, confirming that the selected sample size was sufficient for the study’s objectives (Faul et al., 2009).
Inclusion and exclusion criteria
The inclusion criteria included university students enrolled in universities in Tehran, Iran, during the 2024–2025 academic year, age range within the typical university student age (e.g. 18–30 years), completion of the BSS, belonging to one of the two defined groups based on BSS scores (the high suicidal ideation group: Students scoring above the clinical cutoff [≥9], the low suicidal ideation group: students scoring at the lower end of the scale [≤3]), and voluntary agreement to engage in the study and authorize their participation. The exclusion criteria included incomplete or invalid responses on the BSS or other study measures, and presence of severe neurological or cognitive impairments that interfere with completing self-report questionnaires.
Measures
BSS: The BSS (Beck et al., 1979) is a commonly employed self-report tool designed to evaluate the presence and intensity of suicidal thoughts in individuals. The instrument contains 19 items, each rated on a 3-point scale from 0 to 2, resulting in a total possible score ranging from 0 to 38, with higher scores reflecting more severe suicidal ideation. Scores above 2 are considered indicative of clinically meaningful suicidal thoughts, whereas scores of 2 or lower suggest minimal or low risk (Beck et al., 1988). The BSS has shown excellent internal consistency, with Cronbach’s α values frequently exceeding 0.90, highlighting its high reliability. Its test-re-test reliability has also been supported, with coefficients ranging from 0.54 to 0.96 over periods of one to two weeks, demonstrating sufficient temporal stability (Beck et al., 1988; Beck et al., 1993). The Persian version of the BSS demonstrated high reliability and stability, with Cronbach’s α above 0.80 and test–re-test correlations between 0.54 and 0.96 (Esfahani et al., 2015).
Childhood trauma questionnaire-short form (CTQ-SF): The CTQ-SF is a 28-item self-report instrument designed to retrospectively assess experiences of childhood abuse and neglect (Bernstein et al., 2003). It is a condensed version of the original 70-item childhood trauma questionnaire (Bernstein et al., 1997, 2003). Of the 28 items, 25 are clinical items, divided into five subscales of five items each: Emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. The remaining three items form the Minimization and Denial Scale (items 10, 16, and 22) and are not assigned to any abuse or neglect subscale. Responses are rated on a five-point Likert scale, ranging from 1 (never true) to 5 (very often true). Bernstein et al. (1997) reported acceptable internal consistency, with Cronbach’s α coefficients ranging from 0.49 to 0.85, and established convergent validity with correlations between 0.195 and 0.355 (P<0.01).
Mentalization scale (MentS): The MentS is a 28-item self-report instrument developed to assess an individual’s capacity to understand both their own and others’ behaviors in terms of underlying mental states, including beliefs, emotions, and intentions (Dimitrijević et al., 2018). Each item is rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores reflecting a greater ability to mentalize. Factor analyses have identified a three-factor structure: Self-related mentalization (MentS-S; 8 items), Other-Related Mentalization (MentS-O; 10 items), and Motivation to Mentalize (MentS-M; 10 items). Psychometric evaluations demonstrated satisfactory internal consistency in community samples (α=0.76–0.79 for subscales; α=0.84 for the total score) and acceptable reliability in clinical samples, with somewhat lower values for the motivation subscale (α=0.60). Evidence of validity includes positive associations with empathy, emotional intelligence, openness, extraversion, and conscientiousness, and negative associations with attachment avoidance, attachment anxiety, and neuroticism. Moreover, the MentS has demonstrated criterion validity, with individuals diagnosed with borderline personality disorder scoring significantly lower, particularly on MentS-S. Taken together, these findings support the MentS as a brief, reliable, and valid instrument for assessing mentalization capacity in both research and clinical contexts (Dimitrijević et al., 2018). The Persian version of the MentS demonstrated strong psychometric properties (Ahmadian & Ghamarani, 2021). Reliability analyses indicated strong internal consistency for the scale, with a Cronbach’s α of 0.86 for the overall instrument and acceptable values for the three subscales: MentS-S (α=0.73), MentS-O (α=0.80), and MentS-M (α=0.76). Construct validity was supported through confirmatory factor analysis, which confirmed the original three-factor model and demonstrated good fit indices (comparative fit index [CFI]=0.93, Tucker–Lewis index [TLI]=0.92, Root mean square error of approximation [RMSEA]=0.035). Additional evidence for validity came from significant correlations: MentS scores showed positive associations with mindfulness, secure attachment, and social cognition (convergent validity), and negative associations with avoidant and anxious attachment styles (divergent validity).
Procedure
Once the required approvals for the study were obtained, participants voluntarily agreed to take part. They were provided with information regarding the study’s objectives, procedures, and confidentiality measures, and subsequently gave written informed consent. The BSS was distributed to 528 students for initial screening. According to the BSS cut-off scores, participants with the highest scores were assigned to the high suicidal ideation group, and those with the lowest scores were assigned to the low suicidal ideation group. In the next step, self-report questionnaires related to childhood abuse and mentalization were administered in classroom settings. Research assistants provided standardized instructions and ensured that participants completed the forms independently. The entire procedure took approximately 30–40 minutes. Students identified as having high suicidal ideation were also given referral information for university counseling services.
Data analysis
Descriptive statistics, including means and standard deviations, were initially computed to summarize the data. Subsequently, inferential statistics were applied to evaluate the study hypotheses using multivariate analysis of variance (MANOVA).
Results
Descriptive statistics, including means and standard deviations, were initially computed to summarize the data. Subsequently, inferential statistics were applied to evaluate the study hypotheses, using MANOVA.
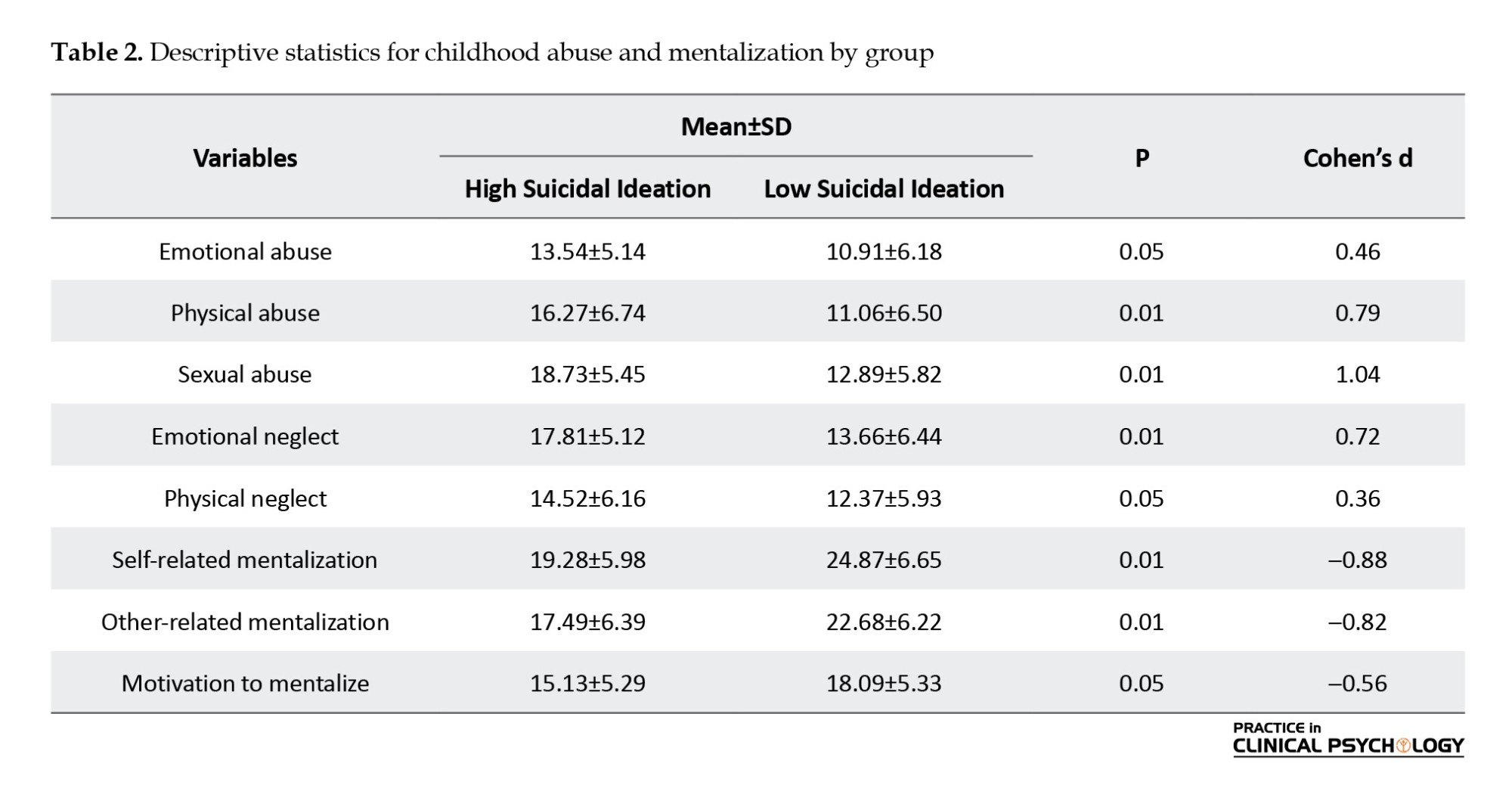
Table 2 presents the descriptive statistics comparing experiences of childhood abuse and levels of mentalization between groups with high and low suicidal ideation. The findings indicate that individuals with high suicidal ideation reported significantly higher levels of emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect compared to their low suicidal ideation counterparts, with P values ranging from 0.01 to 0.05, suggesting meaningful group differences. Conversely, the high suicidal ideation group demonstrated significantly lower scores in MentS-S, MentS-O, and MentS-M, also with significant p-values. Collectively, these results highlight that a history of greater childhood maltreatment is associated with both increased suicidal ideation and a reduced capacity for mentalization, suggesting the importance of early adverse experiences in shaping psychological vulnerabilities.
Prior to conducting the main analyses, the assumptions of MANOVA were examined. The Kolmogorov–Smirnov test indicated no significant deviation from normality for the dependent variables (P>0.05). Box’s M test of equality of covariance matrices was non-significant (P>0.05), confirming the assumption of homogeneity of covariance matrices. Levene’s test results for each dependent variable were also non-significant (P>0.05), indicating homogeneity of variances across groups. Inspection of the correlation matrix showed no evidence of multicollinearity among the dependent variables. Thus, the data satisfied all assumptions required for MANOVA.
Table 3 presents the results of the MANOVA comparing students with high and low suicidal ideation on combined childhood abuse and mentalization variables. The Pillai’s Trace value of 0.127, with a significant F statistic (F=5.526, P<0.001), indicates a statistically significant overall difference between the two groups. The effect size, reflected by a partial eta squared of 0.127, represents a small-to-moderate effect, suggesting that group membership accounts for approximately 13% of the variance in the combined dependent variables. While the confidence intervals indicate precision in the estimates, the practical or clinical significance should be interpreted with caution. Follow-up analyses of individual dependent variables are warranted, and consideration of type I error due to multiple comparisons is noted to ensure balanced interpretation of the findings.

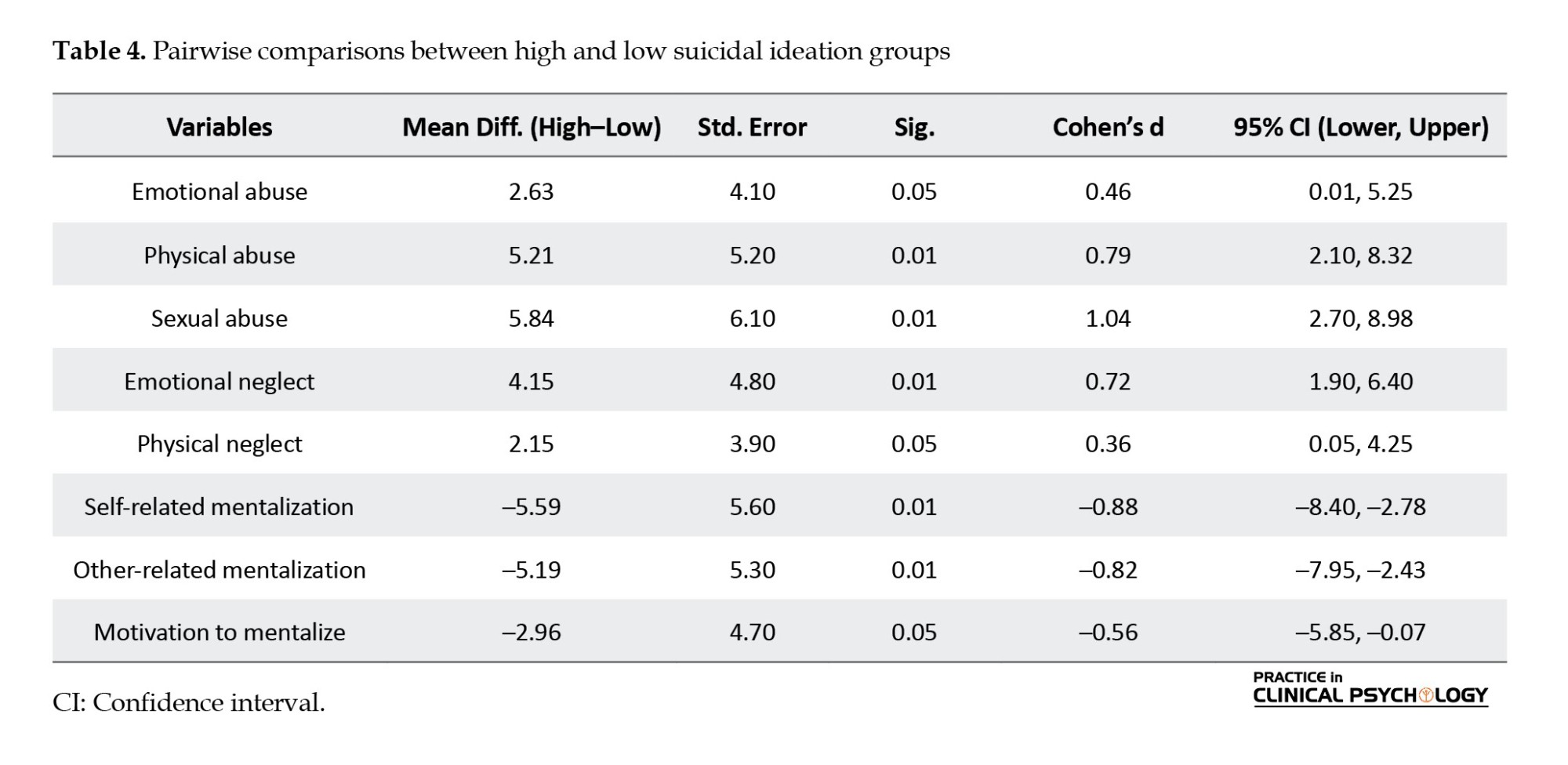
Table 4 presents significant differences across all examined variables. Specifically, individuals in the high suicidal ideation group reported significantly higher levels of abuse (emotional, physical, and sexual) and neglect (emotional and physical) compared to the low group. All comparisons reached either P=0.05 or P=0.01, suggesting statistical significance.
However, beyond statistical significance, effect size estimates (Cohen’s d) indicate varying levels of practical significance. Emotional and physical neglect showed small-to-medium effects (d=0.36, 0.46), suggesting that while differences exist, their magnitude may be modest in practical terms. In contrast, physical and sexual abuse demonstrated large effects (d=0.79, 1.04), underscoring meaningful and practically important group differences.
In terms of psychological functioning, the high suicidal ideation group demonstrated significantly lower levels of self-related and MentS-O, as well as reduced MentS-M. These differences were also moderate to large in magnitude (d=–0.56, –0.88* [*P<0.01]), suggesting that lower mentalization abilities and motivation are not only statistically significant but also practically relevant. The negative mean differences and confidence intervals entirely below zero further support this interpretation.
Taken together, the findings suggest that higher experiences of childhood abuse and neglect are associated with deficits in mentalization capacities, both self- and other-oriented, and a reduced motivation to engage in mentalization processes. This aligns with existing literature indicating that traumatic experiences can impair reflective functioning and socio-emotional development.
Discussion
This study examined the relationship between childhood abuse and mentalization in students with varying levels of suicidal ideation. Consistent with prior research, students with elevated suicidal ideation reported significantly greater exposure to all five categories of childhood maltreatment—emotional, physical, and sexual abuse, as well as emotional and physical neglect—and demonstrated lower scores across all facets of mentalization, including self-related, other-related, and motivational dimensions. These findings underscore the combined influence of developmental trauma and deficits in social-cognitive functioning on susceptibility to suicidal thoughts.
The cumulative burden of multiple abuse types appears particularly salient, with sexual abuse showing the strongest association with suicidal ideation. However, emotional abuse and neglect were also critical, consistent with evidence that less visible forms of maltreatment can profoundly impact mental health, even when controlling for depression and anxiety (Mainali et al., 2023; Kumar et al., 2021; Shafiee-Kandjani et al., 2021; Karimpourvazifehkhorani & Hekmati, 2025). Potential confounders, including social support and depressive symptoms, may partially mediate these associations and should be considered in interpreting the results.
Importantly, significant differences in mentalization suggest that difficulties understanding one’s own and others’ mental states, along with reduced motivation to engage in reflective thinking, may heighten suicide risk. These findings align with developmental theories emphasizing the role of early caregiver-child interactions in fostering reflective capacities (Fonagy & Target, 1997, 2006) and suggest that mentalization may mediate the impact of childhood maltreatment on suicidality (Ensink et al., 2016; Li et al., 2020). Cross-cultural factors, such as family dynamics and societal attitudes toward mental health among Iranian students, may also shape these pathways and warrant further investigation.
Collectively, the results indicate that suicidality arises not only from overwhelming emotional distress but also from impaired reflective functioning. Interventions targeting both trauma and mentalization—such as trauma-informed therapy and mentalization-based approaches—may help students develop adaptive coping strategies and reduce suicide risk. Future research should adopt longitudinal designs to verify the mediating role of mentalization, examine the influence of additional psychological and social factors, and evaluate culturally sensitive intervention strategies.
Practical implications
The present findings underscore the importance of integrating trauma-informed interventions into both clinical and educational settings. For clinicians, early screening for adverse childhood experiences and difficulties in mentalization can guide personalized treatment planning, particularly for individuals presenting with suicidal ideation. Approaches such as trauma-focused cognitive-behavioral therapy and mentalization-based therapy may help improve emotion regulation and reflective functioning, thereby reducing suicide risk.
Within universities, counseling centers and student support services can benefit from implementing trauma-informed policies that foster safety, empowerment, and trust. Training staff to recognize trauma-related symptoms and impaired mentalization may enhance early identification and referral. Furthermore, incorporating psychoeducational workshops on emotional awareness, stress management, and resilience building can promote mental well-being among students. Collectively, these strategies can help bridge the gap between research and practice by translating empirical findings into actionable interventions.
Conclusion
In conclusion, the present study demonstrates that both childhood abuse and impairments in mentalization are significantly associated with suicidal ideation among university students. These findings emphasize the need to consider both developmental trauma and reflective functioning when evaluating suicide risk. Integrating trauma-informed and mentalization-based approaches into prevention and intervention strategies may be critical to reducing vulnerability to suicide among young adults.
Limitations and future directions
Several limitations should be considered when interpreting the findings of this study. First, the sampling strategy focused on students with extreme BSS scores, excluding those with moderate levels of suicidal ideation. While this approach enhanced group differentiation, it may limit the generalizability of the results to the broader student population. Second, participants were recruited exclusively from Shahed University in Tehran, which constrains the cultural and demographic diversity of the sample and limits its cross-cultural applicability. Third, the reliance on self-report questionnaires (BSS, CTQ-SF, and MentS) raises concerns regarding response biases, social desirability, and shared method variance. Fourth, potential confounding factors, such as depressive symptoms, anxiety, or social support, were not controlled for, which may have influenced the observed relationships between childhood abuse, mentalization, and suicidal ideation. Finally, the cross-sectional, causal-comparative design precludes conclusions about temporal or causal pathways between variables. Future research should aim to address these limitations by employing longitudinal designs to clarify the temporal and mediating roles of mentalization in the link between childhood abuse and suicidality. Expanding recruitment to multiple universities and culturally diverse populations would enhance generalizability and cross-cultural understanding. Incorporating multimethod assessments, including clinical interviews and behavioral tasks, would improve validity and reduce reliance on self-report measures. Additionally, controlling for relevant psychological and social factors, such as depression, anxiety, and social support, will provide a more nuanced understanding of the mechanisms underlying suicidal ideation. Finally, intervention-focused research examining trauma-informed and mentalization-based strategies can inform effective preventive and therapeutic programs for at-risk students.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of Shahed University, Tehran, Iran (Code: IR.SHAHED.REC.1403.105). The study adhered to the ethical principles outlined in the Declaration of Helsinki. Participants were fully informed about the aims and procedures of the study and were assured that their responses would remain confidential and anonymous. Written informed consent was obtained from all participants before data collection commenced.
Funding
This article was extracted from the doctoral dissertation of Ehsan Akbari, approved by Shahed University, Tehran, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank all participants for their valuable contribution to this study.
References
Suicidal ideation is a key predictor of suicidal behavior and is influenced by multiple factors, including biological, psychological, social, and familial determinants (Bertule et al., 2021; Serebriakova et al., 2025). Among young people, these factors can increase the likelihood of suicide attempts, highlighting the importance of identifying key risk mechanisms (Afifi et al., 2016). Globally, suicide is a leading cause of mortality among individuals aged 15–29 (World Health Organization, 2025).
Childhood abuse—including emotional, physical, and sexual abuse, as well as emotional and physical neglect—is a well-established risk factor for suicidal ideation and behavior (Angelakis et al., 2020; Berardelli et al., 2022). Evidence suggests that specific abuse subtypes, particularly sexual abuse, may exert a direct effect on suicidal thoughts, whereas other forms may influence ideation indirectly through mediators, such as depression, anxiety, or reduced social support (Huang & Hou, 2023; McRae et al., 2022). Meta-analyses indicate substantial heterogeneity across studies, highlighting the need for more nuanced research to clarify these pathways (Dube et al., 2023; Xie et al., 2024).
Mentalization—the ability to understand one’s own and others’ mental states—plays a critical role in emotion regulation and social cognition (Arabadzhiev & Paunova, 2024; Wagner-Skacel et al., 2022). Deficits in mentalization can impair emotion regulation and social problem-solving, increasing vulnerability to psychological distress and suicidal ideation (Doba et al., 2025; Zohdi et al., 2022; Pompili et al., 2017). Childhood abuse, encompassing emotional, physical, and sexual maltreatment as well as neglect, can profoundly disrupt the development of mentalization—the ability to understand and interpret one’s own and others’ mental states. Early exposure to abusive or neglectful caregiving environments often impairs the formation of secure attachment, limits opportunities for emotional reflection, and fosters distorted self and other representations. These deficits in mentalization hinder emotional regulation and interpersonal understanding, increasing susceptibility to maladaptive coping strategies such as suicidal ideation. Consequently, impaired mentalization serves as a critical psychological mechanism through which childhood abuse contributes to elevated suicide risk in young adults (Yang & Huang, 2024; Wang et al., 2021).
Emerging evidence suggests that childhood abuse and impaired mentalization interact to heighten suicide risk (Weijers et al., 2018; Wagner-Skacel et al., 2022). Students with higher suicidal ideation not only report more adverse childhood experiences but also demonstrate greater difficulties in mentalization (Li et al., 2020; Yang et al., 2025). This interaction underscores the importance of addressing both trauma and reflective functioning in preventive and therapeutic interventions. Future research should employ longitudinal and culturally sensitive designs to further clarify these mechanisms and inform targeted strategies to reduce suicide risk among vulnerable students.
Childhood abuse can have profound effects on a child’s emotional and cognitive development, particularly in shaping the capacity for self-reflection and understanding others. The quality of early caregiving experiences plays a critical role in the development of mentalization—the ability to interpret and understand one’s own and others’ mental states (Arabadzhiev & Paunova, 2024; Fonagy & Target, 1997). When children experience maltreatment instead of sensitive and responsive caregiving, the development of mentalization may be disrupted. Traumatic interactions such as neglect, emotional invalidation, or abuse can impair the child’s ability to regulate emotions and recognize internal psychological states, leading to distorted perceptions of the self and others (Wagner-Skacel et al., 2022; Doba et al., 2025). Consequently, deficits in mentalization may mediate the relationship between childhood abuse and later suicidal ideation by undermining adaptive emotion regulation and social understanding.
Objective
This study aimed to examine the relationship between childhood abuse and mentalization among students exhibiting high versus low levels of suicidal ideation using a comparative approach. Two hypotheses were formulated. The first predicted that students with elevated suicidal ideation would report substantially higher levels of childhood abuse—including emotional, physical, sexual abuse, and neglect—than those with lower suicidal ideation. The second hypothesized that students with higher suicidal ideation would show markedly greater impairments in mentalization compared to their low-risk peers.
Materials and Methods
This study employed a descriptive, causal-comparative design. The population comprised all students of Shahed University in Tehran Province, Iran, during the 2024–2025 academic year. The Beck scale for suicide ideation (BSS) (Beck et al., 1979) was distributed to 528 students. In the present study, students scoring above the clinical cutoff (≥9) were organized as the high suicidal ideation group, whereas students scoring at the lower end of the scale (≤3) were classified as the low suicidal ideation group. Based on these scores, 112 students were selected and assigned to two groups: 56 students with the highest scores formed the high suicidal ideation group, and 56 students with the lowest scores formed the low suicidal ideation group (Table 1). Sample size estimation was conducted using G*Power software with the following parameters: medium effect size (d=0.2), 95% confidence level, 80% statistical power, with two groups and two variables, confirming that the selected sample size was sufficient for the study’s objectives (Faul et al., 2009).
Inclusion and exclusion criteria
The inclusion criteria included university students enrolled in universities in Tehran, Iran, during the 2024–2025 academic year, age range within the typical university student age (e.g. 18–30 years), completion of the BSS, belonging to one of the two defined groups based on BSS scores (the high suicidal ideation group: Students scoring above the clinical cutoff [≥9], the low suicidal ideation group: students scoring at the lower end of the scale [≤3]), and voluntary agreement to engage in the study and authorize their participation. The exclusion criteria included incomplete or invalid responses on the BSS or other study measures, and presence of severe neurological or cognitive impairments that interfere with completing self-report questionnaires.
Measures
BSS: The BSS (Beck et al., 1979) is a commonly employed self-report tool designed to evaluate the presence and intensity of suicidal thoughts in individuals. The instrument contains 19 items, each rated on a 3-point scale from 0 to 2, resulting in a total possible score ranging from 0 to 38, with higher scores reflecting more severe suicidal ideation. Scores above 2 are considered indicative of clinically meaningful suicidal thoughts, whereas scores of 2 or lower suggest minimal or low risk (Beck et al., 1988). The BSS has shown excellent internal consistency, with Cronbach’s α values frequently exceeding 0.90, highlighting its high reliability. Its test-re-test reliability has also been supported, with coefficients ranging from 0.54 to 0.96 over periods of one to two weeks, demonstrating sufficient temporal stability (Beck et al., 1988; Beck et al., 1993). The Persian version of the BSS demonstrated high reliability and stability, with Cronbach’s α above 0.80 and test–re-test correlations between 0.54 and 0.96 (Esfahani et al., 2015).
Childhood trauma questionnaire-short form (CTQ-SF): The CTQ-SF is a 28-item self-report instrument designed to retrospectively assess experiences of childhood abuse and neglect (Bernstein et al., 2003). It is a condensed version of the original 70-item childhood trauma questionnaire (Bernstein et al., 1997, 2003). Of the 28 items, 25 are clinical items, divided into five subscales of five items each: Emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. The remaining three items form the Minimization and Denial Scale (items 10, 16, and 22) and are not assigned to any abuse or neglect subscale. Responses are rated on a five-point Likert scale, ranging from 1 (never true) to 5 (very often true). Bernstein et al. (1997) reported acceptable internal consistency, with Cronbach’s α coefficients ranging from 0.49 to 0.85, and established convergent validity with correlations between 0.195 and 0.355 (P<0.01).
Mentalization scale (MentS): The MentS is a 28-item self-report instrument developed to assess an individual’s capacity to understand both their own and others’ behaviors in terms of underlying mental states, including beliefs, emotions, and intentions (Dimitrijević et al., 2018). Each item is rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores reflecting a greater ability to mentalize. Factor analyses have identified a three-factor structure: Self-related mentalization (MentS-S; 8 items), Other-Related Mentalization (MentS-O; 10 items), and Motivation to Mentalize (MentS-M; 10 items). Psychometric evaluations demonstrated satisfactory internal consistency in community samples (α=0.76–0.79 for subscales; α=0.84 for the total score) and acceptable reliability in clinical samples, with somewhat lower values for the motivation subscale (α=0.60). Evidence of validity includes positive associations with empathy, emotional intelligence, openness, extraversion, and conscientiousness, and negative associations with attachment avoidance, attachment anxiety, and neuroticism. Moreover, the MentS has demonstrated criterion validity, with individuals diagnosed with borderline personality disorder scoring significantly lower, particularly on MentS-S. Taken together, these findings support the MentS as a brief, reliable, and valid instrument for assessing mentalization capacity in both research and clinical contexts (Dimitrijević et al., 2018). The Persian version of the MentS demonstrated strong psychometric properties (Ahmadian & Ghamarani, 2021). Reliability analyses indicated strong internal consistency for the scale, with a Cronbach’s α of 0.86 for the overall instrument and acceptable values for the three subscales: MentS-S (α=0.73), MentS-O (α=0.80), and MentS-M (α=0.76). Construct validity was supported through confirmatory factor analysis, which confirmed the original three-factor model and demonstrated good fit indices (comparative fit index [CFI]=0.93, Tucker–Lewis index [TLI]=0.92, Root mean square error of approximation [RMSEA]=0.035). Additional evidence for validity came from significant correlations: MentS scores showed positive associations with mindfulness, secure attachment, and social cognition (convergent validity), and negative associations with avoidant and anxious attachment styles (divergent validity).
Procedure
Once the required approvals for the study were obtained, participants voluntarily agreed to take part. They were provided with information regarding the study’s objectives, procedures, and confidentiality measures, and subsequently gave written informed consent. The BSS was distributed to 528 students for initial screening. According to the BSS cut-off scores, participants with the highest scores were assigned to the high suicidal ideation group, and those with the lowest scores were assigned to the low suicidal ideation group. In the next step, self-report questionnaires related to childhood abuse and mentalization were administered in classroom settings. Research assistants provided standardized instructions and ensured that participants completed the forms independently. The entire procedure took approximately 30–40 minutes. Students identified as having high suicidal ideation were also given referral information for university counseling services.
Data analysis
Descriptive statistics, including means and standard deviations, were initially computed to summarize the data. Subsequently, inferential statistics were applied to evaluate the study hypotheses using multivariate analysis of variance (MANOVA).
Results
Descriptive statistics, including means and standard deviations, were initially computed to summarize the data. Subsequently, inferential statistics were applied to evaluate the study hypotheses, using MANOVA.
Table 2 presents the descriptive statistics comparing experiences of childhood abuse and levels of mentalization between groups with high and low suicidal ideation. The findings indicate that individuals with high suicidal ideation reported significantly higher levels of emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect compared to their low suicidal ideation counterparts, with P values ranging from 0.01 to 0.05, suggesting meaningful group differences. Conversely, the high suicidal ideation group demonstrated significantly lower scores in MentS-S, MentS-O, and MentS-M, also with significant p-values. Collectively, these results highlight that a history of greater childhood maltreatment is associated with both increased suicidal ideation and a reduced capacity for mentalization, suggesting the importance of early adverse experiences in shaping psychological vulnerabilities.
Prior to conducting the main analyses, the assumptions of MANOVA were examined. The Kolmogorov–Smirnov test indicated no significant deviation from normality for the dependent variables (P>0.05). Box’s M test of equality of covariance matrices was non-significant (P>0.05), confirming the assumption of homogeneity of covariance matrices. Levene’s test results for each dependent variable were also non-significant (P>0.05), indicating homogeneity of variances across groups. Inspection of the correlation matrix showed no evidence of multicollinearity among the dependent variables. Thus, the data satisfied all assumptions required for MANOVA.
Table 3 presents the results of the MANOVA comparing students with high and low suicidal ideation on combined childhood abuse and mentalization variables. The Pillai’s Trace value of 0.127, with a significant F statistic (F=5.526, P<0.001), indicates a statistically significant overall difference between the two groups. The effect size, reflected by a partial eta squared of 0.127, represents a small-to-moderate effect, suggesting that group membership accounts for approximately 13% of the variance in the combined dependent variables. While the confidence intervals indicate precision in the estimates, the practical or clinical significance should be interpreted with caution. Follow-up analyses of individual dependent variables are warranted, and consideration of type I error due to multiple comparisons is noted to ensure balanced interpretation of the findings.
Table 4 presents significant differences across all examined variables. Specifically, individuals in the high suicidal ideation group reported significantly higher levels of abuse (emotional, physical, and sexual) and neglect (emotional and physical) compared to the low group. All comparisons reached either P=0.05 or P=0.01, suggesting statistical significance.
However, beyond statistical significance, effect size estimates (Cohen’s d) indicate varying levels of practical significance. Emotional and physical neglect showed small-to-medium effects (d=0.36, 0.46), suggesting that while differences exist, their magnitude may be modest in practical terms. In contrast, physical and sexual abuse demonstrated large effects (d=0.79, 1.04), underscoring meaningful and practically important group differences.
In terms of psychological functioning, the high suicidal ideation group demonstrated significantly lower levels of self-related and MentS-O, as well as reduced MentS-M. These differences were also moderate to large in magnitude (d=–0.56, –0.88* [*P<0.01]), suggesting that lower mentalization abilities and motivation are not only statistically significant but also practically relevant. The negative mean differences and confidence intervals entirely below zero further support this interpretation.
Taken together, the findings suggest that higher experiences of childhood abuse and neglect are associated with deficits in mentalization capacities, both self- and other-oriented, and a reduced motivation to engage in mentalization processes. This aligns with existing literature indicating that traumatic experiences can impair reflective functioning and socio-emotional development.
Discussion
This study examined the relationship between childhood abuse and mentalization in students with varying levels of suicidal ideation. Consistent with prior research, students with elevated suicidal ideation reported significantly greater exposure to all five categories of childhood maltreatment—emotional, physical, and sexual abuse, as well as emotional and physical neglect—and demonstrated lower scores across all facets of mentalization, including self-related, other-related, and motivational dimensions. These findings underscore the combined influence of developmental trauma and deficits in social-cognitive functioning on susceptibility to suicidal thoughts.
The cumulative burden of multiple abuse types appears particularly salient, with sexual abuse showing the strongest association with suicidal ideation. However, emotional abuse and neglect were also critical, consistent with evidence that less visible forms of maltreatment can profoundly impact mental health, even when controlling for depression and anxiety (Mainali et al., 2023; Kumar et al., 2021; Shafiee-Kandjani et al., 2021; Karimpourvazifehkhorani & Hekmati, 2025). Potential confounders, including social support and depressive symptoms, may partially mediate these associations and should be considered in interpreting the results.
Importantly, significant differences in mentalization suggest that difficulties understanding one’s own and others’ mental states, along with reduced motivation to engage in reflective thinking, may heighten suicide risk. These findings align with developmental theories emphasizing the role of early caregiver-child interactions in fostering reflective capacities (Fonagy & Target, 1997, 2006) and suggest that mentalization may mediate the impact of childhood maltreatment on suicidality (Ensink et al., 2016; Li et al., 2020). Cross-cultural factors, such as family dynamics and societal attitudes toward mental health among Iranian students, may also shape these pathways and warrant further investigation.
Collectively, the results indicate that suicidality arises not only from overwhelming emotional distress but also from impaired reflective functioning. Interventions targeting both trauma and mentalization—such as trauma-informed therapy and mentalization-based approaches—may help students develop adaptive coping strategies and reduce suicide risk. Future research should adopt longitudinal designs to verify the mediating role of mentalization, examine the influence of additional psychological and social factors, and evaluate culturally sensitive intervention strategies.
Practical implications
The present findings underscore the importance of integrating trauma-informed interventions into both clinical and educational settings. For clinicians, early screening for adverse childhood experiences and difficulties in mentalization can guide personalized treatment planning, particularly for individuals presenting with suicidal ideation. Approaches such as trauma-focused cognitive-behavioral therapy and mentalization-based therapy may help improve emotion regulation and reflective functioning, thereby reducing suicide risk.
Within universities, counseling centers and student support services can benefit from implementing trauma-informed policies that foster safety, empowerment, and trust. Training staff to recognize trauma-related symptoms and impaired mentalization may enhance early identification and referral. Furthermore, incorporating psychoeducational workshops on emotional awareness, stress management, and resilience building can promote mental well-being among students. Collectively, these strategies can help bridge the gap between research and practice by translating empirical findings into actionable interventions.
Conclusion
In conclusion, the present study demonstrates that both childhood abuse and impairments in mentalization are significantly associated with suicidal ideation among university students. These findings emphasize the need to consider both developmental trauma and reflective functioning when evaluating suicide risk. Integrating trauma-informed and mentalization-based approaches into prevention and intervention strategies may be critical to reducing vulnerability to suicide among young adults.
Limitations and future directions
Several limitations should be considered when interpreting the findings of this study. First, the sampling strategy focused on students with extreme BSS scores, excluding those with moderate levels of suicidal ideation. While this approach enhanced group differentiation, it may limit the generalizability of the results to the broader student population. Second, participants were recruited exclusively from Shahed University in Tehran, which constrains the cultural and demographic diversity of the sample and limits its cross-cultural applicability. Third, the reliance on self-report questionnaires (BSS, CTQ-SF, and MentS) raises concerns regarding response biases, social desirability, and shared method variance. Fourth, potential confounding factors, such as depressive symptoms, anxiety, or social support, were not controlled for, which may have influenced the observed relationships between childhood abuse, mentalization, and suicidal ideation. Finally, the cross-sectional, causal-comparative design precludes conclusions about temporal or causal pathways between variables. Future research should aim to address these limitations by employing longitudinal designs to clarify the temporal and mediating roles of mentalization in the link between childhood abuse and suicidality. Expanding recruitment to multiple universities and culturally diverse populations would enhance generalizability and cross-cultural understanding. Incorporating multimethod assessments, including clinical interviews and behavioral tasks, would improve validity and reduce reliance on self-report measures. Additionally, controlling for relevant psychological and social factors, such as depression, anxiety, and social support, will provide a more nuanced understanding of the mechanisms underlying suicidal ideation. Finally, intervention-focused research examining trauma-informed and mentalization-based strategies can inform effective preventive and therapeutic programs for at-risk students.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of Shahed University, Tehran, Iran (Code: IR.SHAHED.REC.1403.105). The study adhered to the ethical principles outlined in the Declaration of Helsinki. Participants were fully informed about the aims and procedures of the study and were assured that their responses would remain confidential and anonymous. Written informed consent was obtained from all participants before data collection commenced.
Funding
This article was extracted from the doctoral dissertation of Ehsan Akbari, approved by Shahed University, Tehran, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank all participants for their valuable contribution to this study.
References
Afifi, T. O., Taillieu, T., Zamorski, M. A., Turner, S., Cheung, K., & Sareen, J. (2016). Association of child abuse exposure with suicidal ideation, suicide plans, and suicide attempts in military personnel and the general population in Canada. JAMA Psychiatry, 73(3), 229-238. [DOI:10.1001/jamapsychiatry.2015.2732] [PMID]
Ahmadian, Z., & Ghamarani, A. (2021). Reliability and validity of Persian version of mentalization scale in university students. Journal of Fundamentals of Mental Health, 23(4), 233-240. [Link]
Angelakis, I., Austin, J. L., & Gooding, P. (2020). Association of childhood maltreatment with suicide behaviors among young people: A systematic review and meta-analysis. JAMA Network Open, 3(8), e2012563-e2012563. [DOI:10.1001/jamanetworkopen.2020.12563] [PMID]
Arabadzhiev, Z., & Paunova, R. (2024). Complexity of mentalization. Frontiers in Psychology, 15, 1353804. [DOI:10.3389/fpsyg.2024.1353804] [PMID]
Beck, A. T., Kovacs, M., & Weissman, A. (1979). Assessment of suicidal intention: The scale for suicide ideation. Journal of Consulting and Clinical Psychology, 47(2), 343-352. [DOI:10.1037/0022-006X.47.2.343] [PMID]
Beck, A. T., Steer, R. A., Beck, J. S., & Newman, C. F. (1993). Hopelessness, depression, suicidal ideation, and clinical diagnosis of depression. Suicide and Life-Threatening Behavior, 23(2), 139-145. [DOI:10.1111/j.1943-278X.1993.tb00378.x] [PMID]
Beck, A. T., Steer, R. A., & Ranieri, W. F. (1988). Scale for suicide ideation: Psychometric properties of a self-report version. Journal of Clinical Psychology, 44(4), 499-505. [DOI:10.1002/1097-4679(198807)44:43.0.CO;2-6] [PMID]
Berardelli, I., Sarubbi, S., Rogante, E., Erbuto, D., Giuliani, C., Lamis, D. A., Innamorati, M., & Pompili, M. (2022). Association between childhood maltreatment and suicidal ideation: A path analysis study. Journal of Clinical Medicine, 11(8), 2179. [DOI:10.3390/jcm11082179] [PMID]
Bernstein, D. P., Ahluvalia, T., Pogge, D., & Handelsman, L. (1997). Validity of the Childhood Trauma Questionnaire in an adolescent psychiatric population. Journal of the American Academy of Child & Adolescent Psychiatry, 36(3), 340-348. [DOI:10.1097/00004583-199703000-00012] [PMID]
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., et al. (2003). Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse & Neglect, 27(2), 169-190. [DOI:10.1016/S0145-2134(02)00541-0] [PMID]
Bertule, M., Sebre, S. B., & Kolesovs, A. (2021). Childhood abuse experiences, depression and dissociation symptoms in relation to suicide attempts and suicidal ideation. Journal of Trauma & Dissociation, 22(5), 598-614. [DOI:10.1080/15299732.2020.1869652] [PMID]
Dimitrijević, A., Hanak, N., Altaras Dimitrijević, A., & Jolić Marjanović, Z. (2018). The mentalization scale (MentS): A self-report measure for the assessment of mentalizing capacity. Journal of Personality Assessment, 100(3), 268-280. [DOI:10.1080/00223891.2017.1310730] [PMID]
Doba, K., Debbané, M., Auger, E., & Nandrino, JL. (2025). Suicide risk, mentalizing and emotion regulation in adolescents: The role of maternal maladaptive emotion regulation. Journal of Affective Disorders, 374, 342-349. [DOI:10.1016/j.jad.2025.01.052] [PMID]
Dube, S. R., Li, E. T., Fiorini, G., Lin, C., Singh, N., Khamisa, K., McGowan, J., & Fonagy, P. (2023). Childhood verbal abuse as a child maltreatment subtype: A systematic review of the current evidence. Child Abuse & Neglect, 144, 106394. [DOI:10.1016/j.chiabu.2023.106394] [PMID]
Ensink, K., Bégin, M., Normandin, L., & Fonagy, P. (2016). Maternal and child reflective functioning in the context of child sexual abuse: Pathways to depression and externalising difficulties. European Journal of Psychotraumatology, 7(1), 30611. [DOI:10.3402/ejpt.v7.30611] [PMID]
Esfahani, M., Hashemi, Y., & Alavi, K. (2015). Psychometric assessment of beck scale for suicidal ideation (BSSI) in general population in Tehran. Medical journal of the Islamic Republic of Iran, 29, 268.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149-1160. [DOI:10.3758/BRM.41.4.1149] [PMID]
Fonagy, P., & Target, M. (1997). Attachment and reflective function: Their role in self-organization. Development and Psychopathology, 9(4), 679-700. [DOI:10.1017/S0954579497001399] [PMID]
Fonagy, P., & Target, M. (2006). The mentalization-focused approach to self pathology. Journal of Personality Disorders, 20(6), 544-576. [DOI:10.1521/pedi.2006.20.6.544] [PMID]
Huang, M., & Hou, J. (2023). Childhood maltreatment and suicide risk: The mediating role of self-compassion, mentalization, and depression. Journal of Affective Disorders, 341, 52-61. [DOI:10.1016/j.jad.2023.08.112] [PMID]
Karimpourvazifehkhorani, A., & Hekmati, I. (2025). Habit loop in addictive behaviors formation among adolescents: The mediating role of impulsivity. Current Psychology, 44(6), 4313-4325. [DOI:10.1007/s12144-025-07480-0]
Kumar, P., Srivastava, S., Mishra, P. S., & Sinha, D. (2021). Suicidal ideation among adolescents-the role of sexual abuse, depression, and impulsive behavior. Frontiers in Psychiatry, 12, 726039. [DOI:10.3389/fpsyt.2021.726039] [PMID]
Li, E. T., Carracher, E., & Bird, T. (2020). Linking childhood emotional abuse and adult depressive symptoms: The role of mentalizing incapacity. Child Abuse & Neglect, 99, 104253. [DOI:10.1016/j.chiabu.2019.104253] [PMID]
Mainali, P., Motiwala, F., Trivedi, C., Vadukapuram, R., Mansuri, Z., & Jain, S. (2023). Sexual abuse and its impact on suicidal ideation and attempts and psychiatric illness in children and adolescents with posttraumatic stress disorder. The Primary Care Companion for CNS Disorders, 25(1), 45095. [DOI:10.4088/PCC.22m03239] [PMID]
McRae, E., Stoppelbein, L., O’Kelley, S., Smith, S., & Fite, P. (2022). Pathways to suicidal behavior in children and adolescents: Examination of child maltreatment and post-traumatic symptoms. Journal of Child & Adolescent Trauma, 15(3), 715-725. [DOI:10.1007/s40653-022-00439-4] [PMID]
Pompili, M., Innamorati, M., Erbuto, D., Amore, M., & Girardi, P. (2017). Deficits in mentalization predict suicide risk among psychiatric inpatients. European Psychiatry, 41(S1), S264-S265. [DOI:10.1016/j.eurpsy.2017.02.080]
Serebriakova, J., Forkmann, T., Teismann, T., Paashaus, L., Schreiber, D., Schönfelder, A., Juckel, G., & Glaesmer, H. (2025). Exploring the impact of child maltreatment on adult suicidal ideation and suicide attempts. Journal of Affective Disorders, 378, 1-12. [DOI:10.1016/j.jad.2025.02.019] [PMID]
Shafiee-Kandjani, A. R., Alizadeh, M., Nasirzadehghan, A., Kehtary-Harzang, L., Vahedi, M., & Poursadeqiyan, M., et al. (2021). Socioeconomic status and dimensions of mental health with suicidal ideations among students. Iranian Journal of Public Health, 50(10), 2158-2160. [DOI:10.18502/ijph.v50i10.7525] [PMID]
Wagner-Skacel, J., Riedl, D., Kampling, H., & Lampe, A. (2022). Mentalization and dissociation after adverse childhood experiences. Scientific Reports, 12(1), 6809. [DOI:10.1038/s41598-022-10787-8] [PMID]
Wang, B., Xiao, S., & Wang, H. Possible causes of mentalization deficiency and later diagnosed borderline personality disorder: A systematic review. Paper presented at: 2021 5th International Seminar on Education, Management and Social Sciences, Chengdu, China, 2021, July, 1. [DOI:10.2991/assehr.k.210806.188]
Weijers, J., Fonagy, P., Eurelings-Bontekoe, E., Termorshuizen, F., Viechtbauer, W., & Selten, J. P. (2018). Mentalizing impairment as a mediator between reported childhood abuse and outcome in nonaffective psychotic disorder. Psychiatry Research, 259, 463-469. [DOI:10.1016/j.psychres.2017.11.010] [PMID]
World Health Organization. (2025). Suicide worldwide in 2021: Global health estimates. Geneva: World Health Organization. [Link]
Xie, X., Li, Y., Liu, J., Zhang, L., Sun, T., & Zhang, C., et al. (2024). The relationship between childhood maltreatment and non-suicidal self-injury in adolescents with depressive disorders. Psychiatry Research, 331, 115638. [DOI:10.1016/j.psychres.2023.115638] [PMID]
Yang, L., Du, X., & Huang, M. (2025). Childhood maltreatment and non-suicidal self-injury: The mediating role of mentalization and depression. European Journal of Psychotraumatology, 16(1), 2466279. [DOI:10.1080/20008066.2025.2466279] [PMID]
Zohdi, Y., Mohammadkhani, P., & Karimpour-Vazifehkhorani, A. (2022). The role of anhedonia and low arousal in substance use disorder among adolescents with conduct disorder symptoms. Practice in Clinical Psychology, 10(2), 111-120. [DOI:10.32598/jpcp.10.2.815.1]
Type of Study: Original Research Article |
Subject:
Cognitive behavioral
Received: 2025/09/19 | Accepted: 2025/11/2 | Published: 2026/04/27
Received: 2025/09/19 | Accepted: 2025/11/2 | Published: 2026/04/27
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
