

Volume 10, Issue 4 (Autumn 2022)
PCP 2022, 10(4): 287-298 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadeghi N, Izanloo B, Dehghan Nezhad S, Emaminia M. Risk Perception and Social Factors Affecting Protective Behaviors During the COVID-19 Pandemic in an Iranian Sample. PCP 2022; 10 (4) :287-298
URL: http://jpcp.uswr.ac.ir/article-1-821-en.html
URL: http://jpcp.uswr.ac.ir/article-1-821-en.html



1- Department of Psychology, Faculty of Psychology & Education, Kharazmi University, Tehran, Iran.
2- Department of Psychology, Faculty of Psychology & Education, Kharazmi University, Tehran, Iran. , b.ezanloo@gmail.com
3- Department of Psychology, Faculty of Psychology & Education, University of Tehran, Tehran, Iran.
4- Department of Medical Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
2- Department of Psychology, Faculty of Psychology & Education, Kharazmi University, Tehran, Iran. , b.ezanloo@gmail.com
3- Department of Psychology, Faculty of Psychology & Education, University of Tehran, Tehran, Iran.
4- Department of Medical Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
Full-Text [PDF 568 kb]
(458 Downloads)
| Abstract (HTML) (1233 Views)
Full-Text: (292 Views)
1. Introduction
The COVID-19 pandemic is an infectious disease that has affected many people worldwide. This disease spread rapidly across the countries, led to the illness or death of many people, and damaged public and individual health. The consequences of this disease may continue for years, however, the way we interact with it can minimize the health consequences for public health. Prevention is always the best way to control an infectious disease. Most infectious diseases could be prevented through behavioral changes or protective behaviors. These behavioral changes during pandemics include personal hygiene, social distancing, and self-quarantine. In contrast, some people do not pursue these behaviors which causes the spread of the disease in the community. Considering the role of protective behaviors in controlling a pandemic, it is important to assess the risk factors that may cause people to disregard the protective behaviors and not take the threats of this disease seriously. For example, people are expected to become tired of performing health-related behaviors after the onset of pandemics and reduce the risk perception and feeling of vulnerability to infectious disease or by realizing the real risk of the disease, replace their behaviors with new ones that protect their health during the pandemic.
Accordingly, risk perception is an influential factor that should be considered. Many people who do not pursue protective behaviors believe that their susceptibility to the disease is not too great or they will not be infected and will not be at risk if they become sick. Therefore, from a psychological point of view, assessing the risk perception and vulnerability to the disease can predict how people react and interact with it. Lau et al. (2007) examined the role of many factors in protective behaviors during the H1N1 influenza pandemic. In this study, the feeling of vulnerability to the pandemic was significantly associated with protective behaviors. Leung et al. (2003) also found that people with high and moderate risk perceptions, namely women, the elderly, and people with higher education are more likely to pursue protective behaviors against infectious diseases (Leung et al., 2003). Savadori and Lauriola (2021) investigated risk perception and protective behaviors during the rise of COVID-19 in Italy. They found that promoting hygiene and cleaning was mediated by an affective appraisal of risk and the dimension of risk perception predicted avoiding social closeness.
Ning et al. (2020) studied the impacts of risk perception on citizens’ protective behaviors during the outbreak of COVID-19. Their result showed that the majority of Chinese citizens embraced protective behaviors. Higher levels of protective behaviors are associated with higher knowledge, perceived severity, negative emotion, and attention to and trust in the official governmental media. The risk perception and the implementation of protective behaviors have been studied in many studies in the field of pandemics (Barr et al., 2008; Bults et al., 2011; Taglioni et al., 2013).
On the other hand, risk perception can be defined differently in different people and situations. For instance, individuals of different ages, gender, and economic situations may have different risk perceptions. Consequently, these factors can affect protective behaviors. We suppose that social factors, such as gender, age, family structure, and economic situation can be important in protective behaviors and have to be considered. The literature has shown that gender differences can be important and women show more protective behaviors against various diseases. For example, Liu et al. (2020) concluded in a study on psychological status and behavioral changes during the COVID-19 pandemic in China that women have shown more anxiety about this disease (Liu et al., 2020). Moran and Del Valle (2016) in her meta-analysis about the role of gender in supportive behaviors during pandemics found that women are 50% more likely to follow non-drug protective behaviors when compared to men (Moran & Del Valle, 2016). This study showed that there are inherent differences in the type of response by men and women to pandemics. De Zwart et al. (2007) investigated risk perception of avian influenza in Asian and European populations and concluded that in both populations, risk perception was higher among women and the elderly (De Zwart et al., 2007).
Another factor is age. Considering that most victims of this disease are elderly people, it is expected that older people will follow health protocols more and even turn to self-quarantine. On the other hand, many young people believe that they are less likely to be at risk of injury or death from the disease. Commodari (2017) in a study on the role of demographic and psychological variables concluded that older people have a higher risk perception of the flu while younger people in this study showed a lower risk perception.
Another influential factor in protective behaviors is the family structure, namely the number of family members, underlying health conditions among family members which increases the vulnerability to the disease, and interpersonal communication between the members. It seems that this factor is insufficiently investigated. In families where interpersonal communication is more frequent, the likelihood of cluster infection and mortality increases, especially in families where members had repeated communication as a lifestyle before the COVID-19 outbreak. Other interpersonal relationships between friends or colleagues should be investigated as well because, for many people, high social interactions before the outbreak made the quarantine more difficult to tolerate.
Economic condition is also a determining factor that causes people to quit quarantine. In this regard, Di Giuseppe et al. (2008). found that the rate of infection is higher in the lower economic and social classes, especially when they do not receive sufficient information about how the disease is transmitted.
The current study aims to investigate the affecting factors of protective behaviors in COVID-19. We believe that prevention is the best way to cope with pandemic situations. Therefore, knowing more about the factors that impact protective behaviors is necessary. We hypothesized that risk perception is the main factor to adhere to protective behaviors and risk perception can be different in different people. The study intends to determine the variables affecting risk perception and protective behaviors in an Iranian sample and answer whether protective behaviors are different based on social factors and risk perception. In this study, protective behaviors include self-quarantine and adherence to health protocols. Our hypothesis in this study is that risk perception and social variables can affect these behaviors.
2. Participants and Methods
Study participants
The participants were 371 adults with ages 18-60 (224 females and 147 males), which were selected via the convenience sampling method from Karaj City, Iran. Given the study of social and economic conditions, participants were selected from different parts of the age and occupational spectrum. The research data were collected from July to September 2020. Half of the data was completed through an online questionnaire and the other half was collected through a paper-pencil questionnaire. The average time for answering the questions was 30 min.
Study measures
A set of questionnaires were used to collect the data, including demographic questions, perceived vulnerability to disease questionnaire, and questions on protective behaviors following the World Health Organization (WHO) protocol on the COVID-19 disease.
Social variables
Social variables were assessed by demographic questions on age, gender, number of family members, and number of family members who had an underlying disease. A set of questions was used to collect the economic data. In the economic section, job, income, and savings were considered and participants were asked to express their occupations. In the income section, the participants were asked how their income changed during the COVID-19 outbreak (increased/decreased/did not change /had no income). The participants were also asked if they had savings for unpredictable issues before the COVID-19 outbreak. In the interpersonal relationships section, the participants were asked to rate their relationships with family and friends before the COVID-19 outbreak over 3 months (once a week/twice a week/once a month/three times a month).
Risk perception
To assess risk perception, the Duncan et al. vulnerability questionnaire was used to assess the vulnerability to infectious diseases. The vulnerability to disease questionnaire is designed by Duncan et al. (2009) to assess the perceived risk of pandemic infectious diseases. This scale has 15 questions on a scale of 1 to 7, and participants rate their agreement or disagreement with each option on this scale. The questionnaire has 2 subscales: the first measures the perceived infectability and the second shows germ aversion. Duncan et al. (2009) obtained the validity of the scale equal to 0.82 via the Cronbach α method. This scale has been studied in various studies and its validity has been reported as favorable (Ahmadzadeh et al., 2013; Fukukawa et al., 2014; Díaz et al., 2016). In Iran, this questionnaire has been used in the research by Moradi Motlagh et al. (2019) and its validity has been reported in the range of 0.70 to 0.81 through retesting and internal consistency (Moradi et al., 2019). Also, participants were asked two questions about how much risk they rate the disease if they or their family members get infected. Questions were scored on a 7-point Likert scale (very low/low/moderate/much/very much/I don’t know).
Preventive behaviors
WHO protocol on preventive behaviors
To assess the preventive behaviors, according to the WHO protocol, 10 questions were designed for protective behaviors, and participants were asked to rate their adherence to each of these behaviors. The questionnaire’s grade consisted of 5 options, namely “always,” “most often,” “sometimes,” “rarely,” and “never.” The options are scored from 1 to 5. Also, limited contact with individuals in the form of self-quarantine and the extent of communication with family and friends over three months (once a week/twice a week/once a month/three times a month) was measured after the outbreak of COVID-19.
Data analysis
The data were analyzed using the SPSS software, v. 21. Multivariate analysis of variance was used to identify differences between individuals and their social and economic conditions in keeping with self-quarantine and adherence to preventive behaviors. Regression analysis was also used to determine variables that predict protective behaviors more than others.
3. Results
Results were conducted using analysis of variance. Table 1 shows the descriptive indices, namely Mean±SD of the two groups of participants. In the study population, 60% were women and 40% were men. The majority of the participants were under 40 years old and the number of their family members was between 3 to 5; meanwhile, about 23% of the families had a family member with an underlying disease. More than 50% of people had family contacts twice a week. The income of 50% of the participants was not changed during the COVID-19 outbreak, more than half of them had no savings for the quarantine period and less than 50% of the study population remained in quarantine for 3 months. Also, 38% rated the risk of the disease as too high for themselves, while 58% rated the risk perception of the disease as too high for others and family members.
.jpg)
First, we investigated the homogeneity of variances through the Levene test. The results of the Levene test showed that the significance of all components was higher than 0.05. Therefore, error variances were equal in groups.
After examining the homogeneity of the variance, the differences between the independent variables in protective behaviors were analyzed by the analysis of variance method (Table 2).
.jpg)
These results showed that protective behaviors varied according to the number of family members, the duration of quarantine, the assessment of disease risk for themselves and others, and the vulnerability to infectious diseases. Thus, in families with a population of 5 and more, people had more preventive behaviors. Also, people who were kept in quarantine for more than a month had more preventive behaviors. Regarding psychological variables, people who have a moderate and high level of risk perception for themselves and family members also implemented more preventive behaviors. Table 3 shows the results of the analysis of the variance of protective behaviors based on demographic variables.

In this study, regression analysis was used to predict the effect of each variable. The regression analysis of the quarantine variable on independent variables showed that only the variables of gender, family relationships after the COVID-19 outbreak, and self-risk assessment have a significant relationship with the variable of quarantine duration. In total, about 18% of the variance of quarantine is explained, of which 1.4% is gender, 3.1% is family communication after the outbreak, and 2.2% is self-risk assessment. The results of the quarantine variable regression analysis are provided in Table 4.

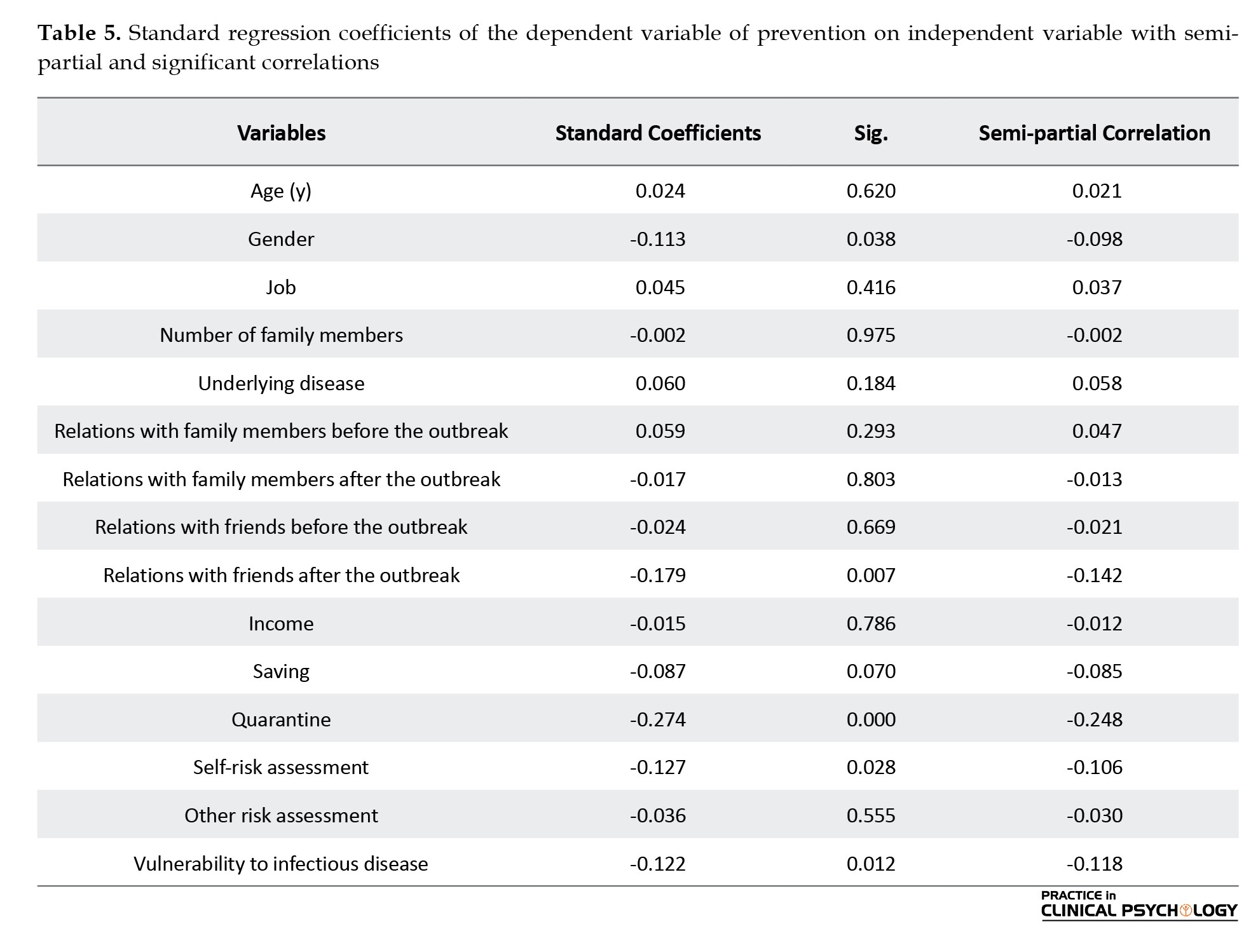
Also, the regression of the prevention variable on independent variables showed that only the variables of gender, relationship with friends after the outbreak, quarantine, self-risk, and vulnerability to infectious diseases have a significant relationship with the prevention variable (Table 5). In total, about 21% of the variance in prevention was explained, of which 0.1% was gender, 2.01% was communication with friends after COVID-19, 1.6% was quarantine, 1.1% was self-risk assessment and 4.1% was a vulnerability to disease.
4. Discussion
This study aimed to investigate the psychological and social risk factors affecting protective behaviors during the COVID-19 pandemic in Iran. The results showed that in the psychological dimension, self-risk assessment and vulnerability to infectious diseases can predict protective behaviors in COVID-19. Participants who rated the risk of COVID-19 as above average for themselves showed more preventative behaviors. On the other hand, protective behaviors were more common in people who were kept in quarantine for more than a month. The duration of quarantine has made a difference in the rate of using preventive measures and this may suggest that people who were kept in quarantine are more protective of their health. It is also possible that these people assess a higher risk of the disease. The results of quarantine regression analysis on the risk perception variable confirm this hypothesis. Based on these results, people with moderate and high risk perceptions are more likely to stay in quarantine and pursue preventative behaviors. In this regard, Wise et al. (2020) investigated changes in risk assessment and protective behaviors during the first week of the onset of the COVID-19 pandemic in the United States. Results of this study showed that protective behaviors, such as social distancing and hand washing were strongly predictable by the perceived risk of this disease. Dryhurst et al. (2020) studied risk perceptions of COVID-19 in 10 American, European, and Asian countries and their results showed that, apart from differences in risk perceptions in these countries, risk perceptions were associated with protective behaviors in all of them. Research on risk perception and protective behaviors in other pandemics worldwide are consistent with this study in that risk perception and vulnerability to the disease are associated with the increase in protective behaviors (Abdelrahman, 2020; Walter et al., 2012; Liao et al., 2014; van der Weerd et al., 2011; Dai et al., 2020). In the social dimension, the family number was different in preventive behaviors, and families with a population of 3 to 5 had the most differences in preventive behaviors. Gender was also another factor that made a difference between the groups. Analysis of the variance of prevention variable based on gender variable showed a significant difference between men and women and the results of the regression analysis showed that gender can predict both protective behaviors and keeping self-quarantine. Previous research also supports the proposition that women exhibit more protective behaviors.
In the current study, women likely feel more vulnerable to infectious diseases. Analysis of gender variance on vulnerability showed a significant difference between men and women (F=075; Sig.=0.05) and this could be one of the possible explanations for why women will be quarantined and implement protective behaviors compared to men. In this regard, Bish and Michie (2010) in a meta-analysis examined the effective demographic and attitudinal factors during the flu pandemic in 2009. They found that vulnerability to the disease was an important factor in protective behaviors. The results of this study showed that women feel more vulnerable to the flu and implement protective behaviors, such as wearing a mask, regular hand washing, surface cleaning, and finally vaccination when compared to men. Finally, the last significant factor in the present study was familial and social relationships.
Family communication in Iran is relatively high and regular and descriptive data indicated that in most cases, communication existed twice a week before the COVID-19 outbreak among family members. On the other hand, communication with family members in most families has decreased sharply after the outbreak and has become once a month; therefore, family communication after the outbreak has predicted the duration of quarantine in individuals. In contrast, communication with friends after the outbreak predicts protective behaviors. The participants appear to keep quarantine for family members but use other protective behaviors for friends. People may tend to reduce the risk to their family members but feel less at risk when communicating with friends. It should be noted that none of the economic variables made a significant difference.
5. Conclusion
According to the results of the present study, it can be concluded that each of the psychological and social variables contributes to the protective behaviors of people in society and this can be different in different societies. This is important because in collectivist societies, social factors may be more prominent than individual factors and conversely in individualistic societies, individual factors may be more important. However, recognizing the impact of each of these factors is essential in health planning to control pandemics. For example, it should be considered that men are more at risk than women in the Iranian sample because they had fewer protective behaviors and to control the disease in this sample, the perceived risk for the disease needs to increase. Also, due to the cultural context of Iranian society, interpersonal communication is of particular importance and this issue can lead to the spread of the disease during the pandemic which must be properly managed. Finally, simplifying the disease and reducing risk perception can lead to the abandonment of protective behaviors in the target community and this study showed that risk perception of the disease is important and can be used as leverage to increase protective behaviors.
Limitations and future research
The first limitation of this research is in terms of data collection during quarantine. Half of the data were completed online and the other half was collected through a paper-pencil questionnaire. Therefore, people who completed the questionnaires online could not use the questionnaire’s guidance like other people. Also, the ratio of women to men in this study was higher and in terms of age, most people were under the age of 40. Finally, another limitation of the present study is related to its generalizability. Considering that the data of this study were collected only from 18- to 65-year-old residents of Karaj City, Iran, the data obtained from this community cannot be generalized to all ages and groups, and generalizing the results should be done carefully. To reach more valid and practical results, cultural differences should be considered and limitations based on generalizability should be minimized. Therefore, research in this area should be done in wider areas and with samples from different and larger communities to ensure the generalizability of the results.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Abdelrahman, M. (2020). Personality traits, risk perception, and protective behaviors of Arab residents of Qatar during the COVID-19 pandemic. International Journal of Mental Health and Addiction, 20(1), 237–248. [PMID]
Ahmadzadeh, M., Ghamarani, A., Samadi, M., Shamsi, A., & Azizollah, A. (2013). The investigation of validity and reliability of a scale of perceived vulnerability to disease in Iran. British Journal of Social Sciences, 1(4), 43-51. [Link]
Barr, M., Raphael, B., Taylor, M., Stevens, G., Jorm, L.,& Giffin, M., et al. (2008). Pandemic influenza in Australia: Using telephone surveys to measure perceptions of threat and willingness to comply. BMC Infectious Diseases, 8, 117. [PMID] [PMCID]
Bish, A., & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. British Journal of Health Psychology, 15(Pt 4), 797–824. [PMID] [PMCID]
Bults, M., Beaujean, D. J., de Zwart, O., Kok, G., van Empelen, P., & van Steenbergen, J. E., et al. (2011). Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: results of three consecutive online surveys. BMC Public Health, 11, 2. [PMID] [PMCID]
Commodari, E. (2017). The role of sociodemographic and psychological variables on risk perception of the flu. Sage Open, 7(3), 2158244017718890. [PMID] [PMCID]
Dai, B., Fu, D., Meng, G., Liu, B., Li, Q., & Liu, X. (2020). The effects of governmental and individual predictors on COVID‐19 protective behaviors in China: A path analysis model. Public Administration Review, 80(5), 797-804. [PMID] [PMCID]
de Zwart, O., Veldhuijzen, I. K., Elam, G., Aro, A. R., Abraham, T., & Bishop, G. D., et al. (2007). Avian influenza risk perception, Europe and Asia. Emerging Infectious Diseases, 13(2), 290–293. [PMID] [PMCID]
Díaz, A., Soriano, J. F., & Beleña, Á. (2016). Perceived vulnerability to disease questionnaire: Factor structure, psychometric properties and gender differences. Personality and Individual Differences, 101, 42-49. [DOI:10.1016/j.paid.2016.05.036]
Di Giuseppe, G., Abbate, R., Albano, L., Marinelli, P., & Angelillo, I. F. (2008). A survey of knowledge, attitudes and practices towards avian influenza in an adult population of Italy. BMC Infectious Diseases, 8, 36. [PMID] [PMCID]
Dryhurst, S., Schneider, C. R., Kerr, J., Freeman, A. L., Recchia, G., & Van Der Bles, A. M., et al. (2020). Risk perceptions of COVID-19 around the world. Journal of Risk Research, 23(7-8), 994-1006. [DOI:10.1080/13669877.2020.1758193]
Duncan, L. A., Schaller, M., & Park, J. H. (2009). Perceived vulnerability to disease: Development and validation of a 15-item self-report instrument. Personality and Individual differences, 47(6), 541-546. [DOI:10.1016/j.paid.2009.05.001]
Fukukawa, Y., Oda, R., Usami, H., & Kawahito, J. (2014). [Development of a Japanese version of the Perceived Vulnerability to Disease Scale (Japanese)]. Shinrigaku kenkyu: The Japanese Journal of Psychology, 85(2), 188–195. [PMID]
Lau, J. T., Kim, J. H., Tsui, H. Y., & Griffiths, S. (2007). Anticipated and current preventive behaviors in response to an anticipated human-to-human H5N1 epidemic in the Hong Kong Chinese general population. BMC Infectious Diseases, 7, 18. [PMID]
Leung, G. M., Lam, T. H., Ho, L. M., Ho, S. Y., Chan, B. H., Wong, I. O., et al. (2003). The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. Journal of Epidemiology & Community Health, 57(11), 857-863. [PMID]
Liao, Q., Cowling, B. J., Lam, W. W., Ng, D. M., & Fielding, R. (2014). Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infectious Diseases, 14, 169. [PMID]
Liu, X., Luo, W. T., Li, Y., Li, C. N., Hong, Z. S., & Chen, H. L., et al. (2020). Psychological status and behavior changes of the public during the COVID-19 epidemic in China. Infectious Diseases of Poverty, 9(1), 58. [PMID] [PMCID]
Moradi Motlagh, M., Nainian, M. R., Fata, L., Gholami Fesharaki, M., & Ghaedi, G. (2019). [Investigation of the moderating role of perceived vulnerability to infectious diseases regarding the relationship between disgust and fear of contamination (Persian)]. Avicenna Journal of Clinical Medicine, 26(1), 34-43. [DOI:10.29252/ajcm.26.1.34]
Moran, K. R., & Del Valle, S. Y. (2016). A meta-analysis of the association between gender and protective behaviors in response to respiratory epidemics and pandemics. PloS One, 11(10), e0164541. [PMID] [PMCID]
Ning, L., Niu, J., Bi, X., Yang, C., Liu, Z., & Wu, Q., et al. (2020). The impacts of knowledge, risk perception, emotion and information on citizens’ protective behaviors during the outbreak of COVID-19: A cross-sectional study in China. BMC Public Health, 20(1), 1751. [PMID] [PMCID]
Savadori, L., & Lauriola, M. (2021). Risk perception and protective behaviors during the rise of the COVID-19 outbreak in Italy. Frontiers in Psychology, 11, 577331. [PMID]
Taglioni, F., Cartoux, M., Dellagi, K., Dalban, C., Fianu, A., & Carrat, F., et l. (2013). The influenza A (H1N1) pandemic in Re:union: Island: Knowledge, perceived risk and precautionary behaviour. BMC Infectious Diseases, 13, 34. [PMID] [PMCID]
van der Weerd, W., Timmermans, D. R., Beaujean, D. J., Oudhoff, J., & van Steenbergen, J. E. (2011). Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health, 11, 575. [PMID] [PMCID]
Wise, T., Zbozinek, T. D., Michelini, G., Hagan, C. C., & Mobbs, D. (2020). Changes in risk perception and protective behavior during the first week of the COVID-19 pandemic in the United States. Royal Society Open Science, 7(9), 200742. [PMID]
Walter, D., Bohmer, M., Reiter, S., Krause, G., & Wichmann, O. (2012). Risk perception and information-seeking behaviour during the 2009/10 influenza A (H1N1) pdm09 pandemic in Germany. Euro Surveillance : Bulletin Europeen Sur les Maladies Transmissibles=European Communicable Disease Bulletin, 17(13), 20131. [PMID]
The COVID-19 pandemic is an infectious disease that has affected many people worldwide. This disease spread rapidly across the countries, led to the illness or death of many people, and damaged public and individual health. The consequences of this disease may continue for years, however, the way we interact with it can minimize the health consequences for public health. Prevention is always the best way to control an infectious disease. Most infectious diseases could be prevented through behavioral changes or protective behaviors. These behavioral changes during pandemics include personal hygiene, social distancing, and self-quarantine. In contrast, some people do not pursue these behaviors which causes the spread of the disease in the community. Considering the role of protective behaviors in controlling a pandemic, it is important to assess the risk factors that may cause people to disregard the protective behaviors and not take the threats of this disease seriously. For example, people are expected to become tired of performing health-related behaviors after the onset of pandemics and reduce the risk perception and feeling of vulnerability to infectious disease or by realizing the real risk of the disease, replace their behaviors with new ones that protect their health during the pandemic.
Accordingly, risk perception is an influential factor that should be considered. Many people who do not pursue protective behaviors believe that their susceptibility to the disease is not too great or they will not be infected and will not be at risk if they become sick. Therefore, from a psychological point of view, assessing the risk perception and vulnerability to the disease can predict how people react and interact with it. Lau et al. (2007) examined the role of many factors in protective behaviors during the H1N1 influenza pandemic. In this study, the feeling of vulnerability to the pandemic was significantly associated with protective behaviors. Leung et al. (2003) also found that people with high and moderate risk perceptions, namely women, the elderly, and people with higher education are more likely to pursue protective behaviors against infectious diseases (Leung et al., 2003). Savadori and Lauriola (2021) investigated risk perception and protective behaviors during the rise of COVID-19 in Italy. They found that promoting hygiene and cleaning was mediated by an affective appraisal of risk and the dimension of risk perception predicted avoiding social closeness.
Ning et al. (2020) studied the impacts of risk perception on citizens’ protective behaviors during the outbreak of COVID-19. Their result showed that the majority of Chinese citizens embraced protective behaviors. Higher levels of protective behaviors are associated with higher knowledge, perceived severity, negative emotion, and attention to and trust in the official governmental media. The risk perception and the implementation of protective behaviors have been studied in many studies in the field of pandemics (Barr et al., 2008; Bults et al., 2011; Taglioni et al., 2013).
On the other hand, risk perception can be defined differently in different people and situations. For instance, individuals of different ages, gender, and economic situations may have different risk perceptions. Consequently, these factors can affect protective behaviors. We suppose that social factors, such as gender, age, family structure, and economic situation can be important in protective behaviors and have to be considered. The literature has shown that gender differences can be important and women show more protective behaviors against various diseases. For example, Liu et al. (2020) concluded in a study on psychological status and behavioral changes during the COVID-19 pandemic in China that women have shown more anxiety about this disease (Liu et al., 2020). Moran and Del Valle (2016) in her meta-analysis about the role of gender in supportive behaviors during pandemics found that women are 50% more likely to follow non-drug protective behaviors when compared to men (Moran & Del Valle, 2016). This study showed that there are inherent differences in the type of response by men and women to pandemics. De Zwart et al. (2007) investigated risk perception of avian influenza in Asian and European populations and concluded that in both populations, risk perception was higher among women and the elderly (De Zwart et al., 2007).
Another factor is age. Considering that most victims of this disease are elderly people, it is expected that older people will follow health protocols more and even turn to self-quarantine. On the other hand, many young people believe that they are less likely to be at risk of injury or death from the disease. Commodari (2017) in a study on the role of demographic and psychological variables concluded that older people have a higher risk perception of the flu while younger people in this study showed a lower risk perception.
Another influential factor in protective behaviors is the family structure, namely the number of family members, underlying health conditions among family members which increases the vulnerability to the disease, and interpersonal communication between the members. It seems that this factor is insufficiently investigated. In families where interpersonal communication is more frequent, the likelihood of cluster infection and mortality increases, especially in families where members had repeated communication as a lifestyle before the COVID-19 outbreak. Other interpersonal relationships between friends or colleagues should be investigated as well because, for many people, high social interactions before the outbreak made the quarantine more difficult to tolerate.
Economic condition is also a determining factor that causes people to quit quarantine. In this regard, Di Giuseppe et al. (2008). found that the rate of infection is higher in the lower economic and social classes, especially when they do not receive sufficient information about how the disease is transmitted.
The current study aims to investigate the affecting factors of protective behaviors in COVID-19. We believe that prevention is the best way to cope with pandemic situations. Therefore, knowing more about the factors that impact protective behaviors is necessary. We hypothesized that risk perception is the main factor to adhere to protective behaviors and risk perception can be different in different people. The study intends to determine the variables affecting risk perception and protective behaviors in an Iranian sample and answer whether protective behaviors are different based on social factors and risk perception. In this study, protective behaviors include self-quarantine and adherence to health protocols. Our hypothesis in this study is that risk perception and social variables can affect these behaviors.
2. Participants and Methods
Study participants
The participants were 371 adults with ages 18-60 (224 females and 147 males), which were selected via the convenience sampling method from Karaj City, Iran. Given the study of social and economic conditions, participants were selected from different parts of the age and occupational spectrum. The research data were collected from July to September 2020. Half of the data was completed through an online questionnaire and the other half was collected through a paper-pencil questionnaire. The average time for answering the questions was 30 min.
Study measures
A set of questionnaires were used to collect the data, including demographic questions, perceived vulnerability to disease questionnaire, and questions on protective behaviors following the World Health Organization (WHO) protocol on the COVID-19 disease.
Social variables
Social variables were assessed by demographic questions on age, gender, number of family members, and number of family members who had an underlying disease. A set of questions was used to collect the economic data. In the economic section, job, income, and savings were considered and participants were asked to express their occupations. In the income section, the participants were asked how their income changed during the COVID-19 outbreak (increased/decreased/did not change /had no income). The participants were also asked if they had savings for unpredictable issues before the COVID-19 outbreak. In the interpersonal relationships section, the participants were asked to rate their relationships with family and friends before the COVID-19 outbreak over 3 months (once a week/twice a week/once a month/three times a month).
Risk perception
To assess risk perception, the Duncan et al. vulnerability questionnaire was used to assess the vulnerability to infectious diseases. The vulnerability to disease questionnaire is designed by Duncan et al. (2009) to assess the perceived risk of pandemic infectious diseases. This scale has 15 questions on a scale of 1 to 7, and participants rate their agreement or disagreement with each option on this scale. The questionnaire has 2 subscales: the first measures the perceived infectability and the second shows germ aversion. Duncan et al. (2009) obtained the validity of the scale equal to 0.82 via the Cronbach α method. This scale has been studied in various studies and its validity has been reported as favorable (Ahmadzadeh et al., 2013; Fukukawa et al., 2014; Díaz et al., 2016). In Iran, this questionnaire has been used in the research by Moradi Motlagh et al. (2019) and its validity has been reported in the range of 0.70 to 0.81 through retesting and internal consistency (Moradi et al., 2019). Also, participants were asked two questions about how much risk they rate the disease if they or their family members get infected. Questions were scored on a 7-point Likert scale (very low/low/moderate/much/very much/I don’t know).
Preventive behaviors
WHO protocol on preventive behaviors
To assess the preventive behaviors, according to the WHO protocol, 10 questions were designed for protective behaviors, and participants were asked to rate their adherence to each of these behaviors. The questionnaire’s grade consisted of 5 options, namely “always,” “most often,” “sometimes,” “rarely,” and “never.” The options are scored from 1 to 5. Also, limited contact with individuals in the form of self-quarantine and the extent of communication with family and friends over three months (once a week/twice a week/once a month/three times a month) was measured after the outbreak of COVID-19.
Data analysis
The data were analyzed using the SPSS software, v. 21. Multivariate analysis of variance was used to identify differences between individuals and their social and economic conditions in keeping with self-quarantine and adherence to preventive behaviors. Regression analysis was also used to determine variables that predict protective behaviors more than others.
3. Results
Results were conducted using analysis of variance. Table 1 shows the descriptive indices, namely Mean±SD of the two groups of participants. In the study population, 60% were women and 40% were men. The majority of the participants were under 40 years old and the number of their family members was between 3 to 5; meanwhile, about 23% of the families had a family member with an underlying disease. More than 50% of people had family contacts twice a week. The income of 50% of the participants was not changed during the COVID-19 outbreak, more than half of them had no savings for the quarantine period and less than 50% of the study population remained in quarantine for 3 months. Also, 38% rated the risk of the disease as too high for themselves, while 58% rated the risk perception of the disease as too high for others and family members.
First, we investigated the homogeneity of variances through the Levene test. The results of the Levene test showed that the significance of all components was higher than 0.05. Therefore, error variances were equal in groups.
After examining the homogeneity of the variance, the differences between the independent variables in protective behaviors were analyzed by the analysis of variance method (Table 2).
These results showed that protective behaviors varied according to the number of family members, the duration of quarantine, the assessment of disease risk for themselves and others, and the vulnerability to infectious diseases. Thus, in families with a population of 5 and more, people had more preventive behaviors. Also, people who were kept in quarantine for more than a month had more preventive behaviors. Regarding psychological variables, people who have a moderate and high level of risk perception for themselves and family members also implemented more preventive behaviors. Table 3 shows the results of the analysis of the variance of protective behaviors based on demographic variables.
In this study, regression analysis was used to predict the effect of each variable. The regression analysis of the quarantine variable on independent variables showed that only the variables of gender, family relationships after the COVID-19 outbreak, and self-risk assessment have a significant relationship with the variable of quarantine duration. In total, about 18% of the variance of quarantine is explained, of which 1.4% is gender, 3.1% is family communication after the outbreak, and 2.2% is self-risk assessment. The results of the quarantine variable regression analysis are provided in Table 4.
Also, the regression of the prevention variable on independent variables showed that only the variables of gender, relationship with friends after the outbreak, quarantine, self-risk, and vulnerability to infectious diseases have a significant relationship with the prevention variable (Table 5). In total, about 21% of the variance in prevention was explained, of which 0.1% was gender, 2.01% was communication with friends after COVID-19, 1.6% was quarantine, 1.1% was self-risk assessment and 4.1% was a vulnerability to disease.
4. Discussion
This study aimed to investigate the psychological and social risk factors affecting protective behaviors during the COVID-19 pandemic in Iran. The results showed that in the psychological dimension, self-risk assessment and vulnerability to infectious diseases can predict protective behaviors in COVID-19. Participants who rated the risk of COVID-19 as above average for themselves showed more preventative behaviors. On the other hand, protective behaviors were more common in people who were kept in quarantine for more than a month. The duration of quarantine has made a difference in the rate of using preventive measures and this may suggest that people who were kept in quarantine are more protective of their health. It is also possible that these people assess a higher risk of the disease. The results of quarantine regression analysis on the risk perception variable confirm this hypothesis. Based on these results, people with moderate and high risk perceptions are more likely to stay in quarantine and pursue preventative behaviors. In this regard, Wise et al. (2020) investigated changes in risk assessment and protective behaviors during the first week of the onset of the COVID-19 pandemic in the United States. Results of this study showed that protective behaviors, such as social distancing and hand washing were strongly predictable by the perceived risk of this disease. Dryhurst et al. (2020) studied risk perceptions of COVID-19 in 10 American, European, and Asian countries and their results showed that, apart from differences in risk perceptions in these countries, risk perceptions were associated with protective behaviors in all of them. Research on risk perception and protective behaviors in other pandemics worldwide are consistent with this study in that risk perception and vulnerability to the disease are associated with the increase in protective behaviors (Abdelrahman, 2020; Walter et al., 2012; Liao et al., 2014; van der Weerd et al., 2011; Dai et al., 2020). In the social dimension, the family number was different in preventive behaviors, and families with a population of 3 to 5 had the most differences in preventive behaviors. Gender was also another factor that made a difference between the groups. Analysis of the variance of prevention variable based on gender variable showed a significant difference between men and women and the results of the regression analysis showed that gender can predict both protective behaviors and keeping self-quarantine. Previous research also supports the proposition that women exhibit more protective behaviors.
In the current study, women likely feel more vulnerable to infectious diseases. Analysis of gender variance on vulnerability showed a significant difference between men and women (F=075; Sig.=0.05) and this could be one of the possible explanations for why women will be quarantined and implement protective behaviors compared to men. In this regard, Bish and Michie (2010) in a meta-analysis examined the effective demographic and attitudinal factors during the flu pandemic in 2009. They found that vulnerability to the disease was an important factor in protective behaviors. The results of this study showed that women feel more vulnerable to the flu and implement protective behaviors, such as wearing a mask, regular hand washing, surface cleaning, and finally vaccination when compared to men. Finally, the last significant factor in the present study was familial and social relationships.
Family communication in Iran is relatively high and regular and descriptive data indicated that in most cases, communication existed twice a week before the COVID-19 outbreak among family members. On the other hand, communication with family members in most families has decreased sharply after the outbreak and has become once a month; therefore, family communication after the outbreak has predicted the duration of quarantine in individuals. In contrast, communication with friends after the outbreak predicts protective behaviors. The participants appear to keep quarantine for family members but use other protective behaviors for friends. People may tend to reduce the risk to their family members but feel less at risk when communicating with friends. It should be noted that none of the economic variables made a significant difference.
5. Conclusion
According to the results of the present study, it can be concluded that each of the psychological and social variables contributes to the protective behaviors of people in society and this can be different in different societies. This is important because in collectivist societies, social factors may be more prominent than individual factors and conversely in individualistic societies, individual factors may be more important. However, recognizing the impact of each of these factors is essential in health planning to control pandemics. For example, it should be considered that men are more at risk than women in the Iranian sample because they had fewer protective behaviors and to control the disease in this sample, the perceived risk for the disease needs to increase. Also, due to the cultural context of Iranian society, interpersonal communication is of particular importance and this issue can lead to the spread of the disease during the pandemic which must be properly managed. Finally, simplifying the disease and reducing risk perception can lead to the abandonment of protective behaviors in the target community and this study showed that risk perception of the disease is important and can be used as leverage to increase protective behaviors.
Limitations and future research
The first limitation of this research is in terms of data collection during quarantine. Half of the data were completed online and the other half was collected through a paper-pencil questionnaire. Therefore, people who completed the questionnaires online could not use the questionnaire’s guidance like other people. Also, the ratio of women to men in this study was higher and in terms of age, most people were under the age of 40. Finally, another limitation of the present study is related to its generalizability. Considering that the data of this study were collected only from 18- to 65-year-old residents of Karaj City, Iran, the data obtained from this community cannot be generalized to all ages and groups, and generalizing the results should be done carefully. To reach more valid and practical results, cultural differences should be considered and limitations based on generalizability should be minimized. Therefore, research in this area should be done in wider areas and with samples from different and larger communities to ensure the generalizability of the results.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Abdelrahman, M. (2020). Personality traits, risk perception, and protective behaviors of Arab residents of Qatar during the COVID-19 pandemic. International Journal of Mental Health and Addiction, 20(1), 237–248. [PMID]
Ahmadzadeh, M., Ghamarani, A., Samadi, M., Shamsi, A., & Azizollah, A. (2013). The investigation of validity and reliability of a scale of perceived vulnerability to disease in Iran. British Journal of Social Sciences, 1(4), 43-51. [Link]
Barr, M., Raphael, B., Taylor, M., Stevens, G., Jorm, L.,& Giffin, M., et al. (2008). Pandemic influenza in Australia: Using telephone surveys to measure perceptions of threat and willingness to comply. BMC Infectious Diseases, 8, 117. [PMID] [PMCID]
Bish, A., & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. British Journal of Health Psychology, 15(Pt 4), 797–824. [PMID] [PMCID]
Bults, M., Beaujean, D. J., de Zwart, O., Kok, G., van Empelen, P., & van Steenbergen, J. E., et al. (2011). Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: results of three consecutive online surveys. BMC Public Health, 11, 2. [PMID] [PMCID]
Commodari, E. (2017). The role of sociodemographic and psychological variables on risk perception of the flu. Sage Open, 7(3), 2158244017718890. [PMID] [PMCID]
Dai, B., Fu, D., Meng, G., Liu, B., Li, Q., & Liu, X. (2020). The effects of governmental and individual predictors on COVID‐19 protective behaviors in China: A path analysis model. Public Administration Review, 80(5), 797-804. [PMID] [PMCID]
de Zwart, O., Veldhuijzen, I. K., Elam, G., Aro, A. R., Abraham, T., & Bishop, G. D., et al. (2007). Avian influenza risk perception, Europe and Asia. Emerging Infectious Diseases, 13(2), 290–293. [PMID] [PMCID]
Díaz, A., Soriano, J. F., & Beleña, Á. (2016). Perceived vulnerability to disease questionnaire: Factor structure, psychometric properties and gender differences. Personality and Individual Differences, 101, 42-49. [DOI:10.1016/j.paid.2016.05.036]
Di Giuseppe, G., Abbate, R., Albano, L., Marinelli, P., & Angelillo, I. F. (2008). A survey of knowledge, attitudes and practices towards avian influenza in an adult population of Italy. BMC Infectious Diseases, 8, 36. [PMID] [PMCID]
Dryhurst, S., Schneider, C. R., Kerr, J., Freeman, A. L., Recchia, G., & Van Der Bles, A. M., et al. (2020). Risk perceptions of COVID-19 around the world. Journal of Risk Research, 23(7-8), 994-1006. [DOI:10.1080/13669877.2020.1758193]
Duncan, L. A., Schaller, M., & Park, J. H. (2009). Perceived vulnerability to disease: Development and validation of a 15-item self-report instrument. Personality and Individual differences, 47(6), 541-546. [DOI:10.1016/j.paid.2009.05.001]
Fukukawa, Y., Oda, R., Usami, H., & Kawahito, J. (2014). [Development of a Japanese version of the Perceived Vulnerability to Disease Scale (Japanese)]. Shinrigaku kenkyu: The Japanese Journal of Psychology, 85(2), 188–195. [PMID]
Lau, J. T., Kim, J. H., Tsui, H. Y., & Griffiths, S. (2007). Anticipated and current preventive behaviors in response to an anticipated human-to-human H5N1 epidemic in the Hong Kong Chinese general population. BMC Infectious Diseases, 7, 18. [PMID]
Leung, G. M., Lam, T. H., Ho, L. M., Ho, S. Y., Chan, B. H., Wong, I. O., et al. (2003). The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. Journal of Epidemiology & Community Health, 57(11), 857-863. [PMID]
Liao, Q., Cowling, B. J., Lam, W. W., Ng, D. M., & Fielding, R. (2014). Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infectious Diseases, 14, 169. [PMID]
Liu, X., Luo, W. T., Li, Y., Li, C. N., Hong, Z. S., & Chen, H. L., et al. (2020). Psychological status and behavior changes of the public during the COVID-19 epidemic in China. Infectious Diseases of Poverty, 9(1), 58. [PMID] [PMCID]
Moradi Motlagh, M., Nainian, M. R., Fata, L., Gholami Fesharaki, M., & Ghaedi, G. (2019). [Investigation of the moderating role of perceived vulnerability to infectious diseases regarding the relationship between disgust and fear of contamination (Persian)]. Avicenna Journal of Clinical Medicine, 26(1), 34-43. [DOI:10.29252/ajcm.26.1.34]
Moran, K. R., & Del Valle, S. Y. (2016). A meta-analysis of the association between gender and protective behaviors in response to respiratory epidemics and pandemics. PloS One, 11(10), e0164541. [PMID] [PMCID]
Ning, L., Niu, J., Bi, X., Yang, C., Liu, Z., & Wu, Q., et al. (2020). The impacts of knowledge, risk perception, emotion and information on citizens’ protective behaviors during the outbreak of COVID-19: A cross-sectional study in China. BMC Public Health, 20(1), 1751. [PMID] [PMCID]
Savadori, L., & Lauriola, M. (2021). Risk perception and protective behaviors during the rise of the COVID-19 outbreak in Italy. Frontiers in Psychology, 11, 577331. [PMID]
Taglioni, F., Cartoux, M., Dellagi, K., Dalban, C., Fianu, A., & Carrat, F., et l. (2013). The influenza A (H1N1) pandemic in Re:union: Island: Knowledge, perceived risk and precautionary behaviour. BMC Infectious Diseases, 13, 34. [PMID] [PMCID]
van der Weerd, W., Timmermans, D. R., Beaujean, D. J., Oudhoff, J., & van Steenbergen, J. E. (2011). Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health, 11, 575. [PMID] [PMCID]
Wise, T., Zbozinek, T. D., Michelini, G., Hagan, C. C., & Mobbs, D. (2020). Changes in risk perception and protective behavior during the first week of the COVID-19 pandemic in the United States. Royal Society Open Science, 7(9), 200742. [PMID]
Walter, D., Bohmer, M., Reiter, S., Krause, G., & Wichmann, O. (2012). Risk perception and information-seeking behaviour during the 2009/10 influenza A (H1N1) pdm09 pandemic in Germany. Euro Surveillance : Bulletin Europeen Sur les Maladies Transmissibles=European Communicable Disease Bulletin, 17(13), 20131. [PMID]
Type of Study: Research |
Subject:
Psychometric
Received: 2022/03/13 | Accepted: 2022/09/28 | Published: 2022/10/1
Received: 2022/03/13 | Accepted: 2022/09/28 | Published: 2022/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Practice in Clinical Psychology (PCP)
University of Social Welfare and Rehabilitation Sciences, Koodakyar Alley, Daneshjoo Blv., Evin, Tehran, Iran
Journal Tel: +9821 71732826
Publisher Tel: +9821 4535 5555 , 4535 5000
Website: http://jpcp.uswr.ac.ir
Email: iranianjcp@gmail.com
